Thrombosis is increasingly recognized in the pediatric age group, especially venous thromboembolism (VTE). However, recent studies showed increasing incidences of childhood thrombotic events due to improved diagnosis, increased survival of children with severe underlying diseases, and increased use of interventions such as central venous lines (CVL). Moreover, the diagnosis of VTE in hospitalized children increased from 34 to 58 cases per 10,000 in the United States from 2001 to 2007. The increased incidence of thrombosis was observed in all pediatric age categories; nevertheless, neonates, infants (< 2 years old), and adolescents have the greatest risk for VTE [8, 9]. Egyptian children who have more than one heterozygous mutation, even if weakly thrombophilic, are prone to developing significant thrombotic events either spontaneously or when exposed to minor risk factors [10].
No previous study for global incidence of pediatric VTE, but a few country-based studies. The majority of them focused on hospital-based populations. Longitudinal data from a population-based cohort study in Québec, QC, Canada, found a stable VTE incidence of 0.29 events per 10,000 person-years in children less than 18 years old over the 11-year study period ending in 2004 [11]. In Korea, the incidence was reported to be 3.27 per 10,000 admissions [12]. In Hong Kong, it was 0.074 per 10,000 children [13].
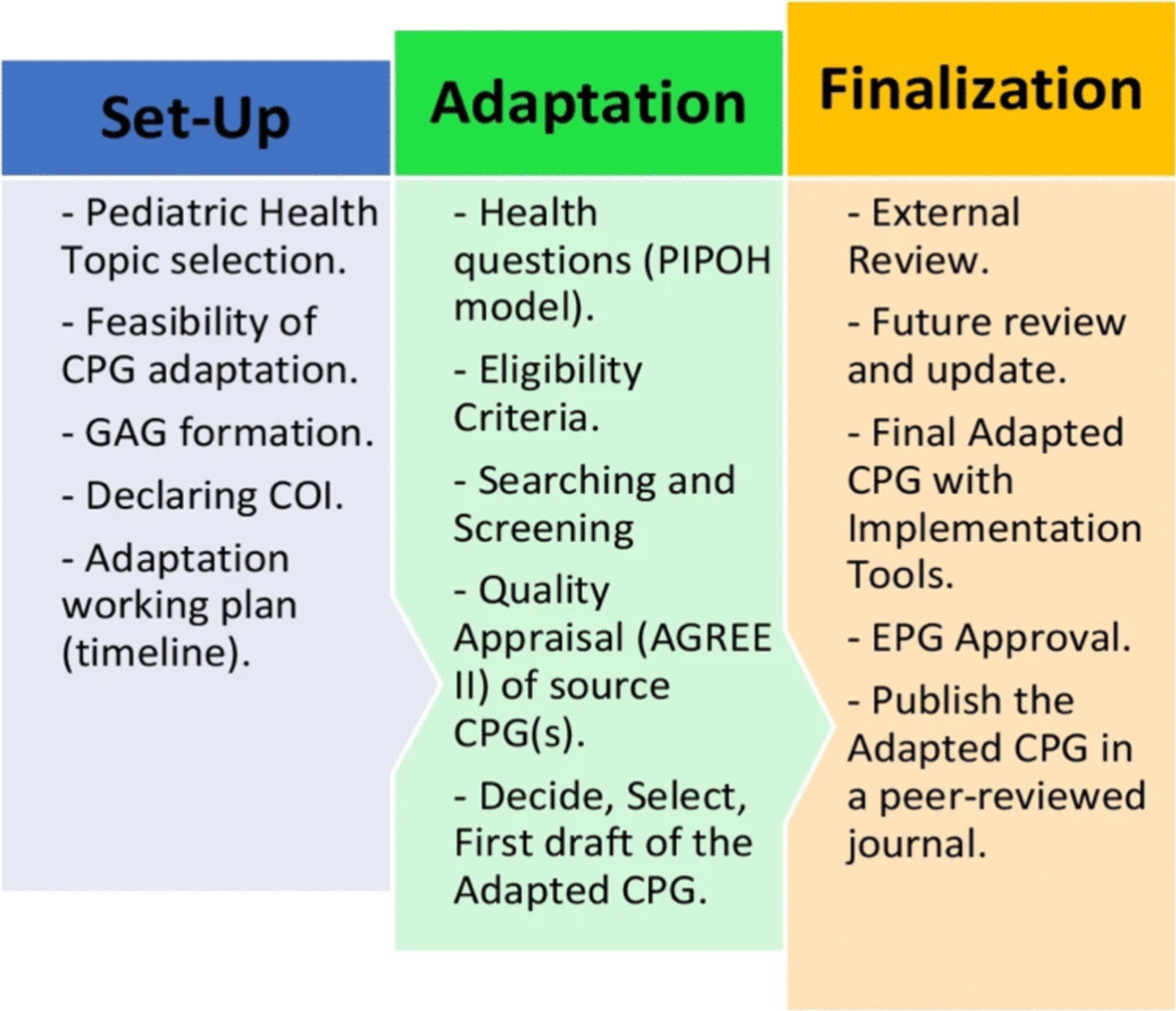
In Egypt, no previous studies have stood on the national epidemiology of pediatric VTE. While different recent standard guidelines for pediatric VTE from different international societies have been released, the clinical implications of such standard guidelines face diversity of challenges in Egypt. The financial constraints, the availability of well-trained specialized health care personnel, the demography, the variability and complexity of the genetic background in different areas in Egypt, and the availability of well-equipped tertiary hospitals that can handle such patients. All these mandate the adaptation of the standard guidelines for pediatric VTE to cop with these challenges and to secure the best available diagnostic and therapeutic chance for such patients.
Thrombosis is a serious disease that leads to mortality and morbidity. The mortality rate is about 2%. Morbidity includes lack of thrombus resolution in 50% of the patients, the development of post-thrombotic syndrome (PTS) in 9%, and recurrent thrombosis in 8.1% with an average follow-up period of 2.86 years [14].
Most of the venous thrombi in children are associated with clinical risk factors such as inheritance of prothrombotic defects, CVL insertion, cardiac disease, surgery, obesity, inflammatory conditions, immobility, medications such as asparaginase and estrogen-containing contraceptives, and cancer patients [15]. Also, there are some diseases with an increased tendency to thrombosis called acquired thrombophilia diseases, such as antiphospholipid syndrome (APS), paroxysmal nocturnal hemoglobinuria (PNH), myeloproliferative neoplasms (MPN), and the presence of a Janus Kinase 2 (JAK2) mutation in the absence of an MPN phenotype [2].
The inheritance of prothrombotic defects is called inherited thrombophilia diseases, which refers to genetic disorders of specific hemostatic proteins that include the factor V Leiden (FVL) variant (F5 G1691A), the prothrombin gene variant (F2 G20210A), protein C (PC) deficiency, protein S (PS) deficiency, and antithrombin (AT) deficiency. The homozygous or combined heterozygous inheritance of any of these prothrombotic genetic defects may lead to spontaneous VTE (unprovoked VTE), VTE with severity disproportionate to the stimulus (provoked VTE), recurrent thrombosis, or VTE at a young age. However, it is still a matter of debate whether it is useful to test for genetic thrombophilia defects in children with a first venous thrombotic event [16].
Cancer patients are at high risk of recurrent VTE; on one side, they are at high risk for anticoagulant-related bleeding, which is associated with high morbidity and resource use [17].
The mainstay of treatment for acute pediatric thrombosis is anticoagulation with heparins and/or vitamin K antagonists. The immediate goals of anticoagulation are to prevent the propagation of acute thrombosis, prevent embolization, and prevent secondary VTE. The duration of therapy is, therefore, predicated on the time-dependent risk of recurrent VTE. Unfortunately, there is limited data with which to accurately define the frequency of VTE recurrence and anticoagulation-associated adverse events in pediatric VTE [6]. Bleeding is the primary complication of anticoagulant therapy and is a risk for all anticoagulants, even when maintained within usual therapeutic ranges. Ironically, whereas unfractionated heparin and coumarin, the oldest and most widely used anticoagulants, have specific antidotes for their anticoagulant effect, many of the newer agents currently undergoing clinical evaluation do not have specific antidotes; thus, the best ways to reverse their actions remain to be determined [7].
The aim of this adapted clinical practice guideline (CPG) is to provide evidence-based recommendations to pediatricians and junior hematologists for the diagnosis, treatment, and prevention of thrombosis in pediatric age groups.



Comments (0)