
Remember me
This manuscript follows TRIPOD reporting guidelines [19]. We conducted a retrospective study of 252 patients with BAVMs who underwent GKRS at our institution between 2011 and 2020. All patients had undergone both MRI and DSA diagnostic procedures before treatment. The exclusion criteria included a history of treatment for BAVMs (n = 50), such as embolization, radiosurgery, or microsurgery; MRI and clinical follow-up less than 2 years after GKRS (n = 44); inadequate quality of pre-GKRS DSA images for subsequent QDSA analysis (n = 17); and presence of infratentorial BAVMs (n = 10). Patients previously treated for BAVMs were excluded because these treatments cause permanent changes to the surrounding brain parenchyma. A total of 131 patients were included in subsequent analyses (Fig. 1). Demographic information (age and sex) and clinical presentations (such as headache, seizure, neurologic deficits, and hemorrhage) were collected through chart reviews. The local institutional review board waived the need for consent in consideration of the retrospective nature of the study.
Fig. 1
Patient selection flowchart. BAVM, brain arteriovenous malformation; DSA, digital subtraction angiography; GKRS, Gamma Knife radiosurgery
MRI and DSA acquisitionMRI was performed using 1.5-T scanners following a protocol that included axial fast spin-echo T2-weighted imaging with 3-mm-thick slices and axial unenhanced 3-dimensional time-of-flight MRA with 1.5-mm-thick slices. DSA examination was conducted for all patients by using a standardized protocol in the angiosuites, Artis zee (2011–2019) and Artis Q (2019–2020) (Siemens Healthcare). After a 4-Fr angiocatheter was placed in the ipsilateral common carotid artery at the C4 vertebral level, a bolus of 12 to 14 mL iodine contrast medium was administered using a power injector within 1.5 s (Liebel-Flarsheim Angiomat, Illumena). The image acquisition protocol involved obtaining 7.5 frames/s for the first 5 s, followed by 4 frames/s for 3 s, 3 frames/s for 2 s, and 2 frames/s for the final 2 s [18, 20].
Stereotactic radiosurgery and clinical follow-up protocolStereotactic radiosurgery was performed using Gamma Knife (Elekta AB) models 4C (2011 to 2012) and Perfexion (2012 to 2020). Stereotactic MRI and DSA were conducted after a Leksell model G (Elekta AB) stereotactic frame was fixed to the patient’s head. MRI and DSA images were integrated for BAVM nidus delineation to determine GKRS target and dose [8, 17]. After GKRS, patients completed outpatient follow-up for neurological assessments at least every 3 months and underwent MRI every 6 months.
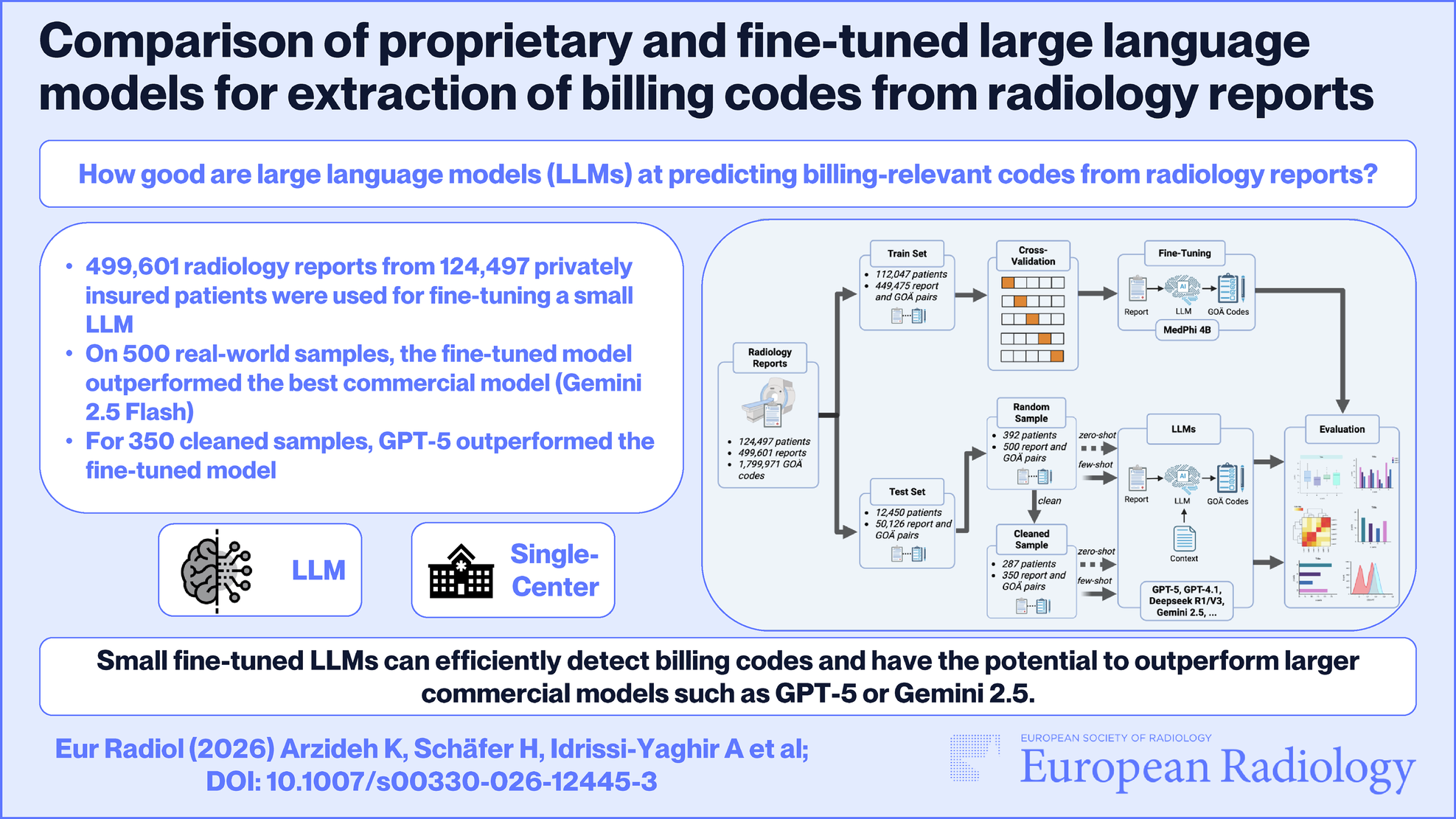
Follow-up MRI findings and outcomesFollow-up MRI was conducted to determine whether RICs were present, as indicated by increased or newly developed perinidal T2 high signal intensity after GKRS [5, 8, 9]. RICs severity was evaluated according to the grading system proposed by Yen et al, with grade I (mild) constituting increased T2 hyperintensity < 1 cm, grade II (moderate) constituting increased T2 hyperintensity ≥ 1 cm and ventricular compression or sulcus effacement, and grade III (severe) constituting cerebral midline shift (Fig. 2) [7]. Symptomatic RICs were defined as the development of neurological symptoms, such as headache, seizure, or neurological deficits, attributable to RICs [8, 9]. The timing of symptomatic RICs development following GKRS and subsequent management strategies were documented. CO was confirmed through MRI based on an absence of flow-related enhancement on MRA and flow voids on T2-weighted images or through DSA based on the disappearance of abnormal arteriovenous shunting [8, 17, 18].
Fig. 2
Examples of the three grades of radiation-induced changes (RICs) severity on axial T2-weighted images. A Grade I (mild) RICs at left parietal lobe with increased T2 hyperintensity < 1 cm (arrow) and no mass effect. B Grade II (moderate) RICs at left posterior frontal lobe with increased T2 hyperintensity ≥ 1 cm and mild ventricular compression (arrow). C Grade III (severe) RICs at right frontal lobe with severe mass effect, marked ventricular compression (arrow), and cerebral midline shift (arrowhead)
BAVM and angioarchitectural featuresIn addition to the location, eloquence, nidal volume, and Spetzler–Martin grade of BAVMs, we investigated angioarchitectural features with reference to previous studies. These features were defined in accordance with the reporting terminology provided by the American Society of Interventional and Therapeutic Neuroradiology [8, 17, 18, 20,21,22]. Flow-related aneurysm was defined as an aneurysm arising from an artery supplying the nidus [8, 17, 18, 20, 22]. Intranidal aneurysm was defined as an aneurysm located within the boundaries of or contiguously with the nidus [8, 17, 18, 22]. Neoangiogenesis was defined as the presence of dilated perinidal arteries or the recruitment of leptomeningeal collateral arteries due to arterial steal caused by a high-flow nidus [8, 17, 18, 20]. Deep venous drainage was defined as drainage through internal cerebral or precentral cerebral veins [8, 17, 18, 21, 22]. Venous stenosis was defined as the presence of a main drainer with a focal diameter 50% smaller than the adjacent venous diameter [8, 17, 18, 20, 22]. Venous ectasia was defined as a diameter change of more than 200% in the draining veins [8, 20]. Pseudophlebitic pattern was defined as tortuous and dilated collateral veins that drained brain parenchyma in the venous phase [8, 17, 18, 20]. BAVMs with superior sagittal sinus (SSS) drainage or parietal cortical drainage were recorded.
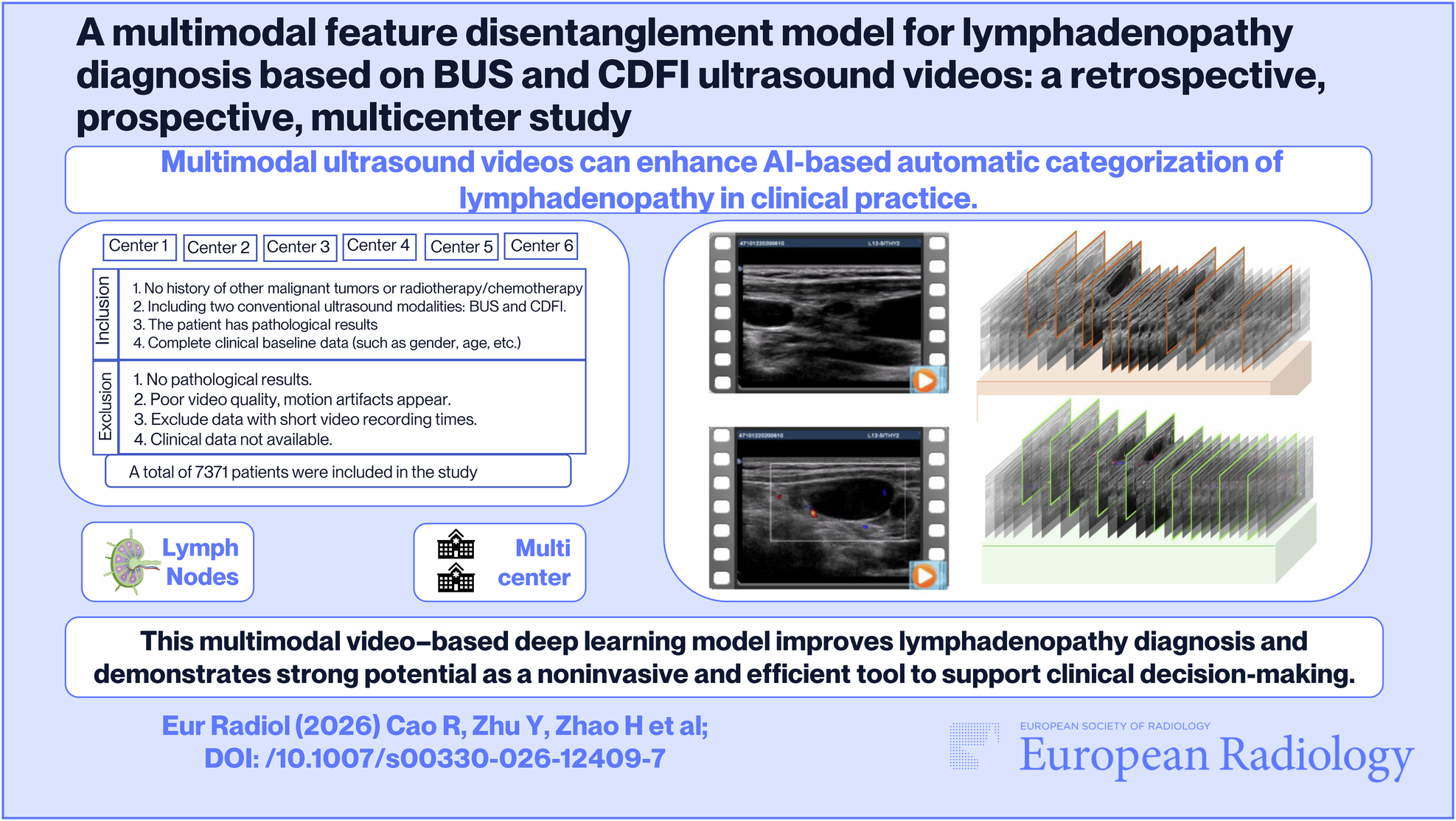
Quantitative angiographic measurementsThe VA ratio, defined as the sum of all draining vein diameters divided by the sum of all supplying artery diameters (see Electronic Supplementary Material) [18]. Anteroposterior and lateral views of DSA images were both used to determine the diameters of individual draining veins and supplying arteries. The narrowest portion of each draining vein was measured if caliber change was observed between the proximal and distal segments. The supplying arteries were defined as the trunk arteries giving rise to the arterial pedicles feeding the BAVM nidus. Figure 3 illustrates the QDSA analysis, which involved postprocessing analysis of the lateral view of the ipsilateral common carotid angiography [8, 17, 18, 20, 22]. The regions of interest (ROIs) included the cavernous segment of the internal carotid artery (ICA) supplying the BAVM, proximal and distal portions of the draining veins, and parietal vein outlet. The time-density curves of the selected ROIs were fitted with a gamma variate function using a customized program (MATLAB, MathWorks). Bolus arrival time (BAT) was defined as the first time point at which density exceeded 20 arbitrary units [18, 20, 22]. Transnidal time was defined as the BAT difference between the cavernous ICA and the proximal portion of the main draining vein [20]. Transvenous time was defined as the BAT difference between the proximal and distal portions of the main draining vein [20]. Modified cerebral circulation time (mCCT) was defined as the BAT difference between the cavernous ICA and the parietal vein outlet [18, 20]. Flow gradients were derived using the linear least-squares method, which involved sequentially fitting four consecutive temporal data points in the gamma variate function. The inflow and outflow gradients were defined as the largest and smallest slopes, respectively, among all fitted linear functions. The stasis index was defined as the inflow gradient divided by the absolute value of the outflow gradient, indicating the degree of venous outflow stagnation [17, 22]. The average stasis index of all distal draining veins was used for subsequent calculations. All angioarchitectural features and quantitative angiographic measurements were analyzed by two neuroradiologists blinded to the clinical data, who respectively had 18 and 9 years of neuroimaging experience. Consensus interpretations and average measurements were used for the subsequent analysis.
Fig. 3
Illustration of quantitative DSA (QDSA) analysis for BAVMs. A Lateral view of QDSA images color-coded on the basis of bolus arrival time (BAT, seconds). Regions of interest (ROIs) included the cavernous segment of the internal carotid artery (ICA), proximal and distal portions of draining veins (DVs), and parietal vein outlet. B QDSA parameters and time-density curve. BAT was defined as the first time point at which the density exceeded 20 arbitrary units (AUs). Modified cerebral circulation time (mCCT) was defined as the BAT difference between ROIs of the cavernous ICA and parietal vein. Inflow and outflow gradients were defined as the largest and smallest slopes, respectively, of all fitted linear functions. The stasis index was defined as the inflow gradient divided by the absolute value of the outflow gradient
Statistical analysisStatistical analysis was performed using SPSS version 24.0 (SPSS, IBM). For categorical and continuous variables, results were presented as numbers (percentages) and median values (interquartile ranges), respectively. Fisher’s exact test was used to compare differences for categorical variables, and the Mann–Whitney U test was used for continuous variables. Spearman correlation was used to determine correlations among continuous variables. Following univariable Firth logistic regression analysis, variables with p < 0.10 were included in subsequent multivariable analysis. Receiver operating characteristic (ROC) analysis was used to determine VA ratio and mCCT cutoff values on the basis of the Youden index. Angioarchitectural and quantitative angiographic models were built to compare their performance in association with symptomatic RICs. The DeLong test was used to compare the area under the ROC curve between models. The Kaplan–Meier method and log-rank tests were used to determine differences in the time to initial development of symptomatic RICs. The statistical significance level was set at p < 0.05.
Comments (0)