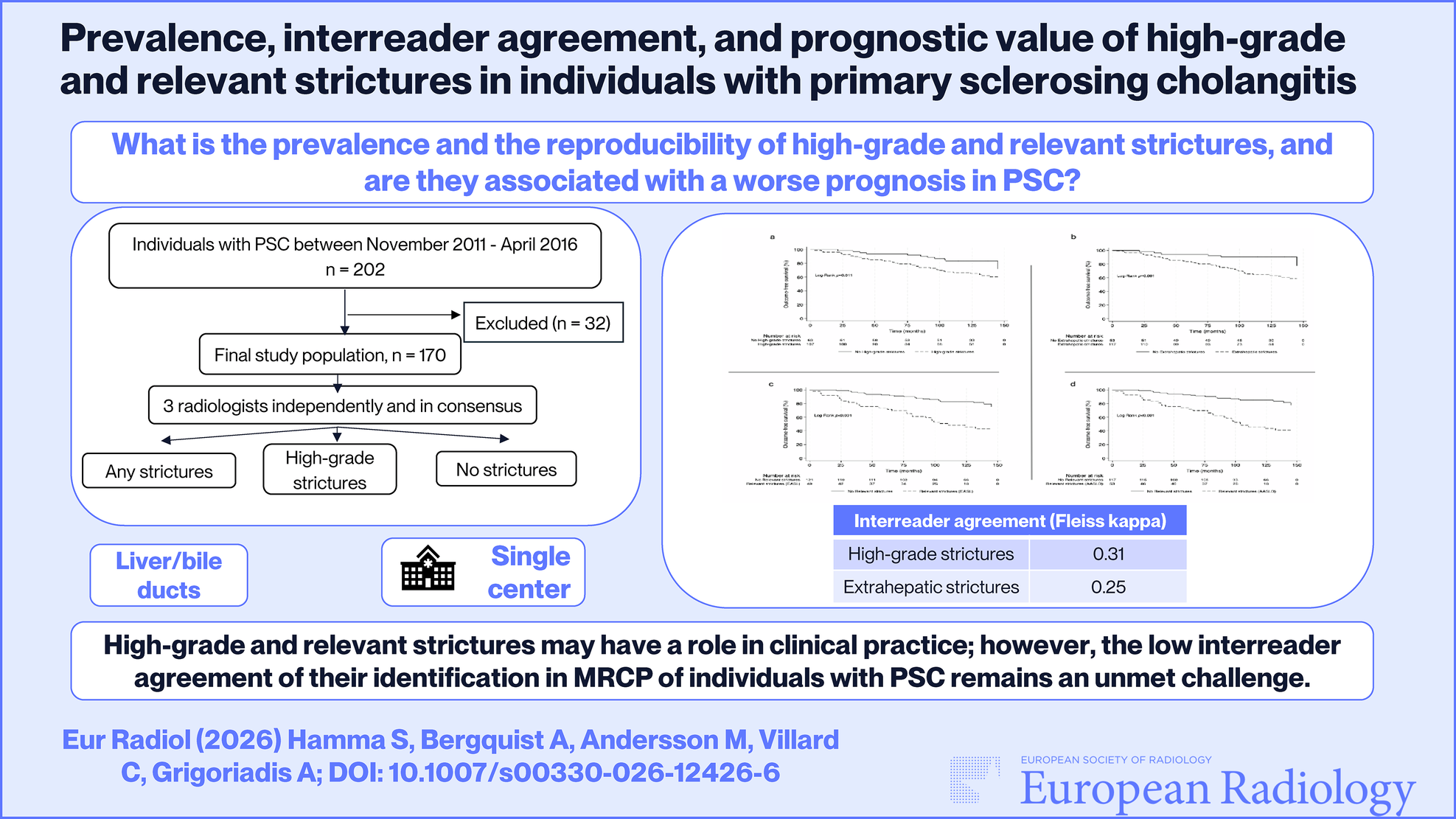
In this study, we evaluated the prevalence and prognostic ability of the new definitions of high-grade and relevant strictures, which are recommended to be used in clinical practice by AASLD and EASL in individuals with large duct PSC. Our findings demonstrated that high-grade strictures were common, occurring in 63% of individuals, while relevant strictures were diagnosed in one-third. Extrahepatic strictures, high-grade strictures, and relevant strictures were all significantly associated with outcomes.
High-grade strictures were a more common finding (63%) in our study than in a previous study, where their prevalence was reported as 50% [14]. This may be attributed to both differences in patient selection and definitions. As suggested by the international liver organizations, we did not include prestenotic dilatation in the definition of high-grade strictures [6,7,8]. Moreover, the prevalence of high-grade strictures in our study was substantially higher (63%) than that of DS reported in a similar cohort of unselected ERCP surveillance setting (25%) [15]. Relevant strictures were present in 30% in our study, which aligns more closely with the aforementioned prevalence of DS. The term DS, based on ERCP, should be avoided in MRI reports; instead, the term high-grade stricture is recommended [6,7,8]. It is, however, worth mentioning that the definitions of relevant strictures/high-grade strictures and DS are fundamentally different. Therefore, the presence of relevant strictures or high-grade strictures at MRCP cannot be interpreted as a definite indicator for the presence of DS at ERCP. Correlation with ERCP findings was beyond the scope of this study, which focused exclusively on the prevalence and prognostic value of the terms high-grade and relevant strictures. Dedicated studies on the correlation between high-grade strictures at MRI, relevant strictures (according to the definitions proposed by EASL and AASLD), and DS at ERCP are an interesting and important topic for future research.
In the development study of the ANALI scores, extrahepatic strictures were not associated with radiological progression [16]. The ANALI scores were subsequently shown to be associated with outcomes in PSC, without including extrahepatic strictures as a variable [17]. However, in the present study, we showed that the presence of extrahepatic strictures is important for prognosis in PSC. Relevant strictures in PSC were introduced to better identify strictures of clinical relevance by combining information from MRCP (strictures) and clinical data, including obstructive cholestasis and bacterial cholangitis. As expected, slightly more individuals had relevant strictures according to the AASLD (31%) definition compared to the EASL (29%) definition, since the former is more inclusive and considers all types of strictures of the extrahepatic biliary tree. We found that more than half of individuals with relevant strictures (55–57%) developed outcomes, compared to 36% among those with high-grade strictures. Outcomes occurred within a median time of approximately 5 years. Despite the difference in the definition of a relevant stricture, with the AASLD definition being more inclusive, both definitions seem to have a similar prognostic ability. Having relevant strictures increased the hazard of developing outcomes about two and a half to three times (HR (EASL) = 2.43, HR (AASLD) = 2.90) in our study. Regarding the classifiers of relevant strictures, the most common was itch, followed by increased ALP. Considering the potential of high-grade and relevant strictures as prognostic biomarkers, one probable disadvantage is that both apply only to strictures of the extrahepatic biliary tree, whereas ductal changes of the intrahepatic biliary tree have been associated with clinical outcomes in PSC [17, 18]. The DiStrict score, another cholangiographic morphological imaging score, includes both intrahepatic and extrahepatic ductal changes, and has shown a strong and independent predictive ability [18]. Additionally, the DiStrict score includes dilatation of the bile ducts upstream strictures as a measure of their strength and potential to affect the liver function, and not their grade, as high-grade strictures do. The ANALI score without gadolinium also includes dilatation of the intrahepatic ducts [17]. In clinical practice, MRCP-based stricture metrics are likely to be most informative when integrated with parenchymal MRI scores and functional measurements, such as the potential functional stricture [14, 19], rather than interpreted in isolation, to provide a more comprehensive risk stratification in PSC.
Three out of four individuals with CCA had high-grade strictures, but only one of them had a relevant stricture according to the definition of both AASLD and EASL. However, CCA was diagnosed at a median time of 7.8 years after the MRI was performed. The occurrence of CCA was rare, and the high prevalence of benign high-grade strictures illustrates the challenge of diagnosing CCA and the need for additional biomarkers for CCA detection beyond the mere presence of strictures in the extrahepatic biliary tree.
We showed that the agreement for the identification of high-grade strictures was unsatisfactory, which is a crucial aspect of their clinical application. The agreement observed in our study was lower compared to the only other study on high-grade strictures [14], where the agreement was moderate. Notably, despite the readers´ long experience, the identification of any type of stricture was only fair (k = 0.25), suggesting a potential need for further standardization of stricture identification and evaluation of bile ducts with MRCP in general. Investigation of the usefulness of findings from other sequences, such as diffusion-weighted images, or from T1-w cholangiography after injection of gadoxetic acid (such as potential functional stricture (PFS) [14]), may be useful and more reproducible. Utilization of all types of clinical features, specifically radiological ones, demands robustness and reproducibility. We did not have a formal consensus training before the study, which may have influenced interreader agreement. However, these results align with several previous studies examining the interreader agreement of the evaluation of radiological findings in PSC [11, 20, 21]. The observed low agreement is a challenge that is yet to be overcome, undermining the clinical utilization of radiological findings, such as high-grade strictures and relevant strictures.
Our study has limitations. There is no well-accepted definition of cholangitis in PSC [5]. We used prospectively collected data where cholangitis was defined as cholangitis that needed medical treatment with antibiotics, which seemed to be a reasonable approach. We did not use information obtained from imaging after intravenous contrast injection to identify cholangitis, which could have contributed to a more objective definition of cholangitis. However, the goal of the study was to utilize MRCP images only. Fourteen individuals, of whom 4 developed outcomes, were excluded due to low MRCP quality. Bilirubin values were significantly higher in the excluded patients; nevertheless, within the normal range of values, suggesting slightly more advanced disease. However, all other laboratory parameters, including MELD score, albumin, and ALP, were not statistically different. Furthermore, we focused on assessing the interreader agreement and did not assess the intrareader agreement. Despite the relatively large sample size of our study population (n = 170), the number of individuals without high-grade strictures was somehow small, due to the high prevalence of high-grade strictures in our cohort, which may have affected our results. Moreover, we did not assess the longitudinal changes of strictures, namely whether strictures developed between exams, which may impact the potential usefulness of these strictures and warrant further evaluation in future studies. Lastly, although major hardware and software upgrades did not occur during the study period and MRCP parameters were kept stable, minor protocol variations over time cannot be completely excluded.
We conclude that extrahepatic and high-grade strictures are common in PSC, yet their identification and consequently identification of relevant strictures seem to be challenging even for experienced radiologists. The presence of all types of extrahepatic strictures, including those classified as relevant by either EASL or AASLD definition, seems to be associated with a poorer prognosis. However, the insufficient agreement for their identification limits the potential of direct clinical implementation. These findings, nevertheless, encourage the simultaneous utilization of radiological and clinical features in the pursuit of good surrogate endpoints for clinical trials; however, larger multicenter studies are needed.

Comments (0)