
Remember me
The study population comprised 48 patients: 21 with Vp1-2 (44%, 21/48) and 27 with Vp3 (56%, 27/48). The largest tumor diameter was 7.1 ± 3.0 cm (mean ± standard deviation (SD)) (Table 1). The mean administered activity was 4.1 ± 1.6 GBq, corresponding to a mean absorbed dose of 283 ± 141 Gy to the perfused liver lobe, as calculated using the single-compartment MIRD method (Table 2). In terms of the treatment plan, RS, lobar treatment, and the tandem approach were performed for 2 patients (4.2%, 2/48), 8 patients (16.7%, 8/48), and 38 patients (79.2%, 38/48), respectively.
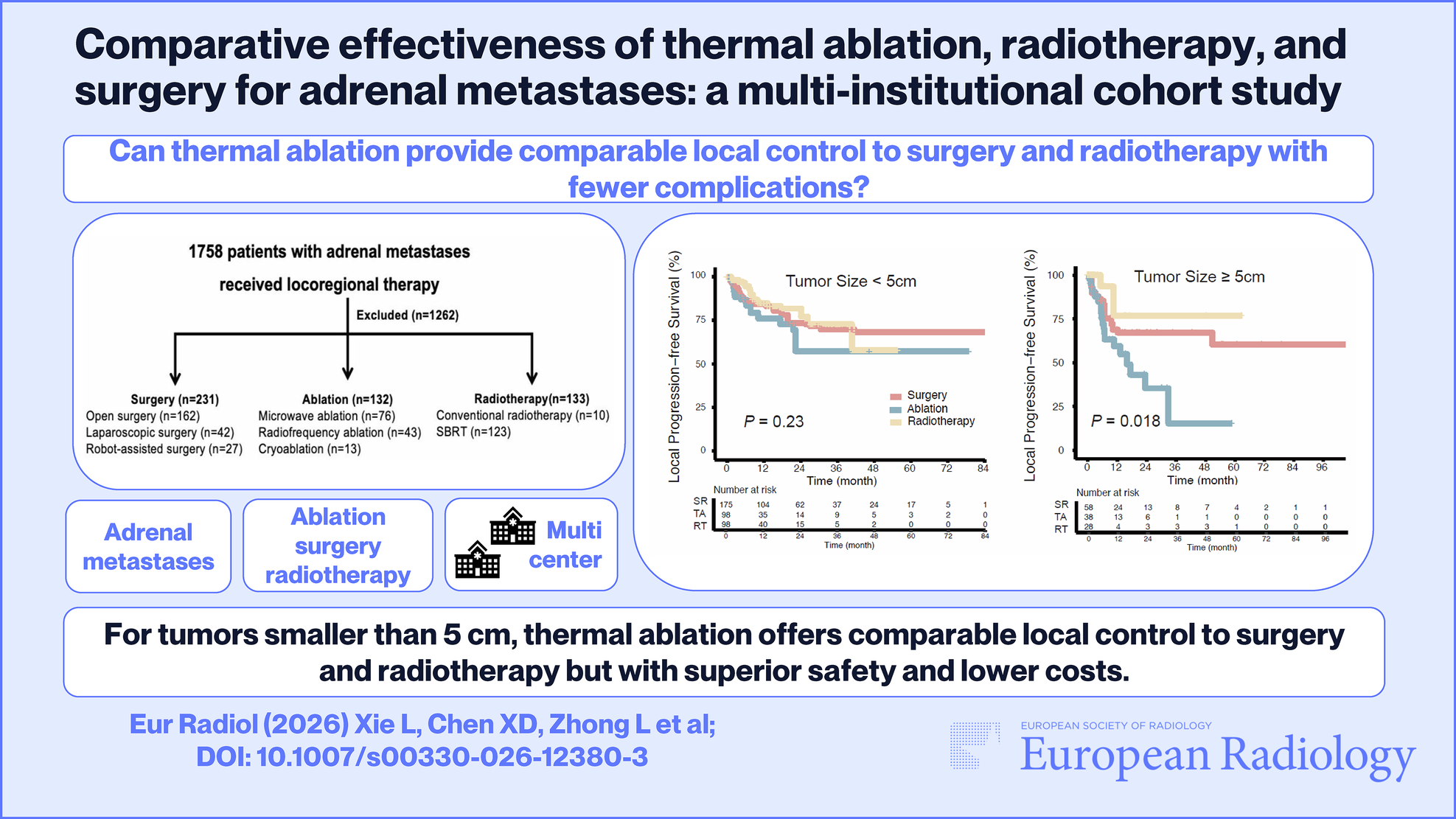
Table 1 Baseline characteristics of the 48 patients treated by radioembolization for hepatocellular carcinoma with localized portal vein invasion (PVI)Table 2 Planning of radioembolization for hepatocellular carcinoma with localized portal vein invasionEffectivenessThe best radiologic tumor responses, as evaluated by mRECIST, were as follows: CR in 22 patients (46%, 22/48), partial response in 18 patients (38%, 18/48), stable disease in 5 patients (10%, 5/48), and progressive disease in 3 patients (6%, 3/48). According to localized mRECIST, the local tumor responses were: CR in 25 patients (52%, 25/48), partial response in 17 patients (35%, 17/48), stable disease in 5 patients (10%, 5/48), and progressive disease in 1 patient (2%, 1/48). The ORRs were 83% (40/48) by mRECIST and 88% (42/48) by localized mRECIST. The DoR for responders was 11.2 months (95% confidence interval (CI), 5.5–20.3 months) by mRECIST and 30.0 months (95% CI, 10.5–30.0 months) by localized mRECIST. The median PFS was 8.5 months (95% CI, 4.6–14.3 months), HPFS was 12.2 months (95% CI, 6.5–21.6 months), and OS was 47.2 months (95% CI, 19.1–52.1 months). The Vp1-2 group demonstrated significantly longer PFS (p = 0.023; hazard ratio (HR) = 0.462; 95% CI, 0.238–0.900) and HPFS (p = 0.004; HR = 0.338; 95% CI, 0.163–0.702) compared to the Vp3 group (Fig. 3). While the Vp1-2 group also exhibited longer OS (median, 49.5 months) than the Vp3 group (median, 35.1 months), the difference did not achieve statistical significance (p = 0.061; HR = 0.480; 95% CI, 0.222–1.035) in this study.
Fig. 3
Post-radioembolization survival outcomes in patients with localized PVI. A Progression-free survival of the Vp1-2 group (median, 15.2 months; 95% confidence interval (CI), 4.4 to 23.3 months) and Vp3 group (median 6.9 months; 95% CI, 3.3 to 11.2 months) (p = 0.023). B Hepatic progression-free survival of the Vp1-2 group (median, 23.3 months; 95% CI, 12.2 to 23.3 months) and Vp3 group (median, 8.3 months; 95% CI, 3.6 to 12.7 months) (p = 0.004). C Overall survival of the Vp1-2 group (median, 49.5 months; 95% CI, 33.2 to 49.5 months) and Vp3 group (median, 35.1 months; 95% CI, 8.5 to 51.0 months) (p = 0.061)
SafetySixteen of the 48 patients (33%) experienced grade 3 or higher adverse events. The most common events were a decrease in lymphocyte count (17%, 8/48) and anemia (10%, 5/48) (Table 3). One case of radiation pneumonitis occurred following 90Y-RE with an estimated lung dose of 26.3 Gy. This patient developed fever and dyspnea 14 days post-treatment and was managed with steroid therapy. However, 5 weeks later, while tapering the steroids, the patient contracted SARS-CoV-2, developed acute respiratory distress syndrome, and experienced grade 4 elevations in aspartate aminotransferase and alanine aminotransferase levels. Despite intensive care unit management for 19 days, the patient expired. Aside from this case, no other patients died within 3 months of 90Y-RE.
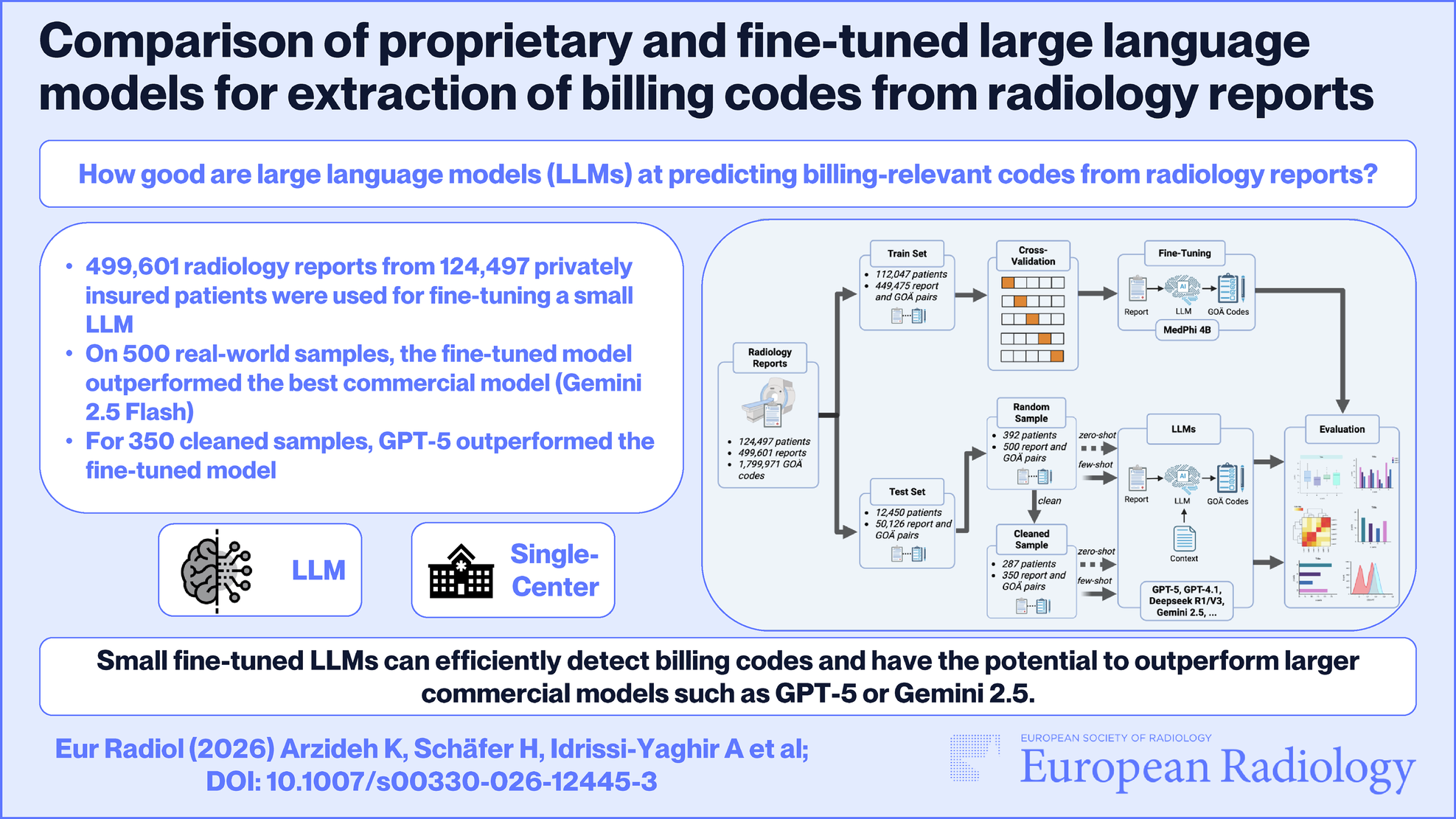
Table 3 Adverse events following radioembolization for hepatocellular carcinoma with localized portal vein invasionPost-treatment clinical courseAlthough OS was assessed for all patients, the clinical course was evaluated for 45 patients, excluding 3 who were lost to follow-up. The median follow-up duration for the clinical course was 46.6 months. Nine patients (20.0%, 9/45) did not receive any cancer-directed treatment after 90Y-RE due to a durable radiologic CR. Curative resection was conducted as the second treatment for 8 patients (17.8%, 8/45). Twenty patients (44.4%, 20/45) underwent locoregional treatments as their second-line therapy, including transarterial chemoembolization, repeat 90Y-RE, percutaneous ablation, or external beam radiotherapy (Fig. 4). During the follow-up periods, curative resection (n = 9) or liver transplantation (n = 1) was performed in 10 of the 48 patients (20.8%, 10/48). The median time from 90Y-RE to surgery was 3.8 months (interquartile range, 1.6 to 8.3 months). Among surgically treated patients, the median OS was 49.5 months. For patients with Vp1-2 (n = 6) who underwent surgery, the median OS was not reached, while for those with Vp3 (n = 4), the median OS was 19.1 months (95% CI, 13.2–27.4 months). Although the difference approached significance, it did not reach statistical significance (p = 0.058).
Fig. 4
Sankey plot depicting the clinical course following radioembolization in patients with hepatocellular carcinoma and localized portal vein tumor thrombosis. PVI, portal vein tumor thrombosis; Vp1-2, segmental to sectional PVI; Vp3, lobar PVI; RS, radiation segmentectomy; N/A, not applicable due to the cancer-free status; TACE, transarterial chemoembolization; EBRT, external beam radiotherapy; ATEZ/BEV, atezolizumab plus bevacizumab; TKI, tyrosine kinase inhibitor; F/U, follow-up; BSC, best supportive care for palliation
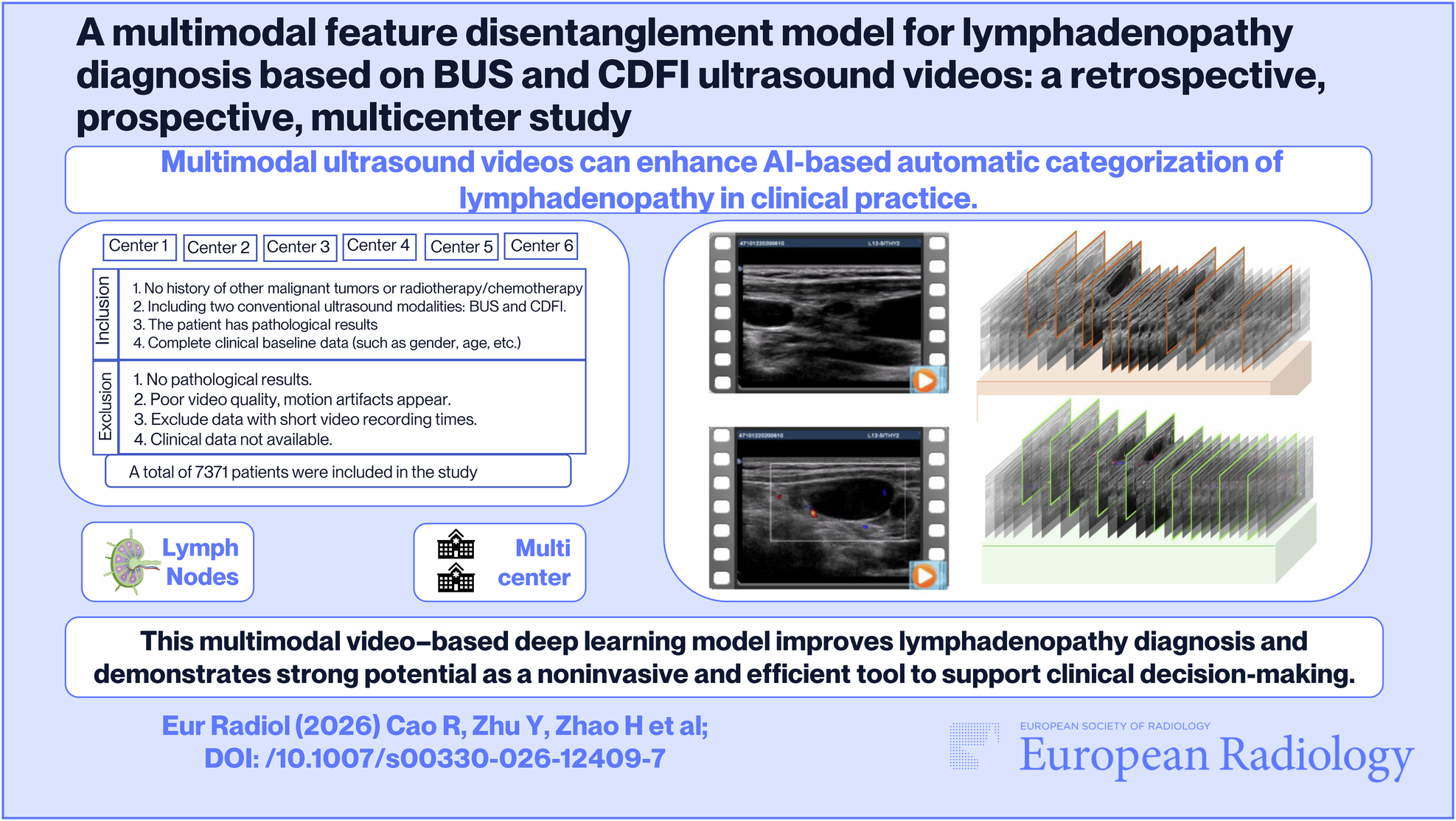
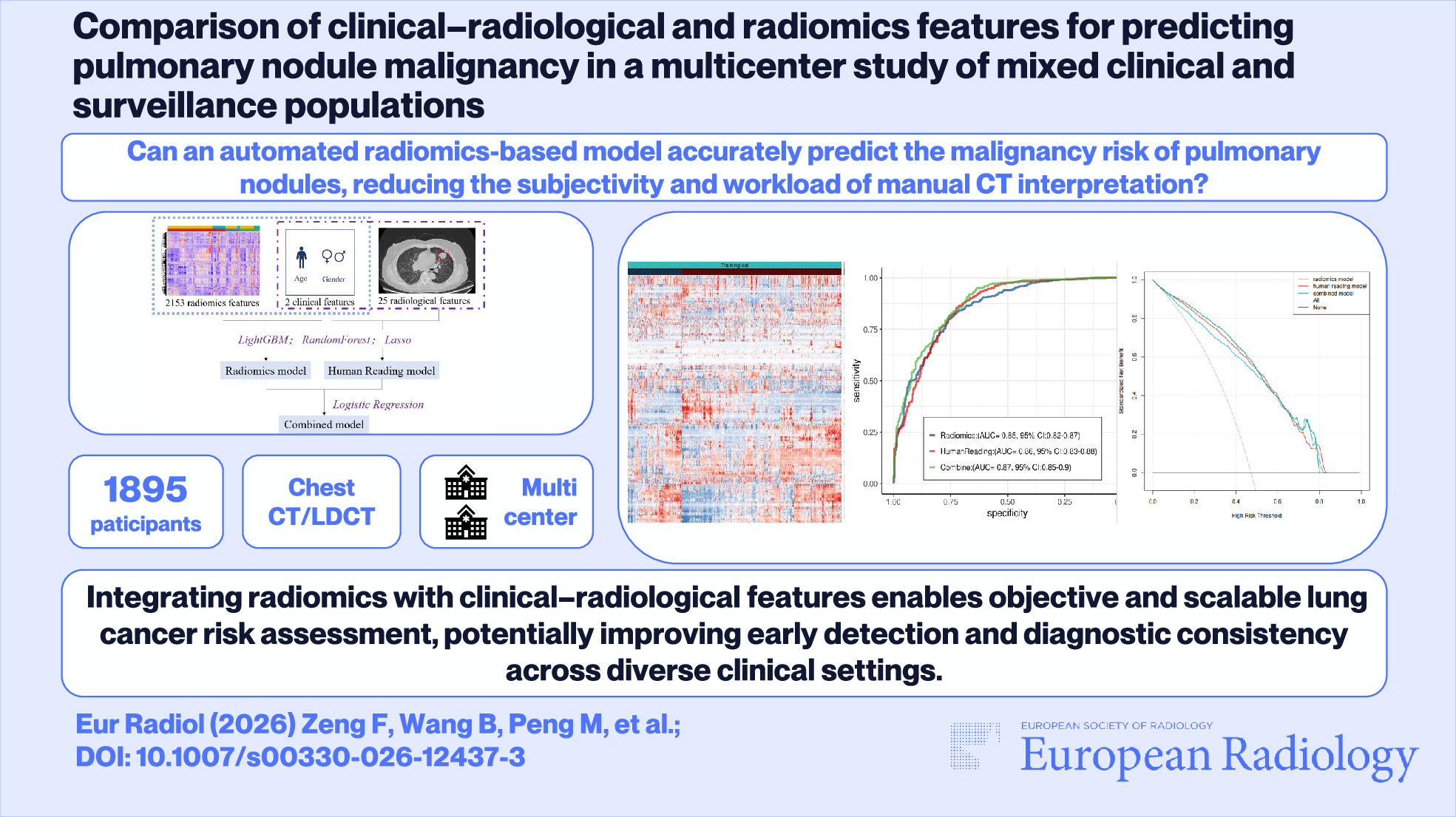
Dosimetry analysisOn pre-treatment SPECT-CT images, the tumor-to-normal liver uptake ratios (TNRs) were 3.7 ± 1.9 for patients with Vp1-2 and 2.6 ± 1.6 for those with Vp3. Notably, the TNR on Y90 PET-CT nearly doubled in patients with Vp1-2, where the tandem approach was frequently employed, reaching 7.4 ± 11.5. Correspondingly, the mean TAD was higher in patients with Vp1-2 (628 ± 377 Gy) compared to those with Vp3 (397 ± 248 Gy) (Table 4). The ROC analysis showed that the area under the curve was 0.725 (95% CI: 0.572–0.848; p = 0.004) (Fig. 5). Using a threshold of 335 Gy for the mean TAD, the sensitivity and specificity for predicting radiologic CR by localized mRECIST were 79% and 67%, respectively. To obtain higher specificity while maintaining acceptable sensitivity, a mean TAD threshold of 574 Gy provided 50% sensitivity and 86% specificity for predicting radiologic CR (positive predictive value, 80%). Post-treatment Y90 PET-CT analyses were performed for all but three patients who did not undergo Y90 PET-CT. Based on the univariate analyses, TAD (p = 0.031), PVI level (p = 0.067), and largest tumor size (p = 0.027) were included in the multivariate Cox proportional hazards analysis, and the TAD was identified as the only significant factor influencing OS (p = 0.032, hazard ratio = 0.862 per 100 Gy, 95% CI = 0.753 to 0.988). As a proposed threshold dose for HCC with localized PVI, 586 Gy was drawn as the cutoff with the lowest p-value (p = 0.021) (Fig. 6). The median OS of patients whose mTAD > 586 Gy and ≤ 586 Gy were 49.5 months and 21.9 months, respectively.
Fig. 5
The receiver operating characteristics curve demonstrating the tumor-absorbed dose threshold and predictability of radiologic complete response by localized mRECIST (area under the curve, 0.725; 95% confidence interval, 0.572–0.848; p = 0.004)
Fig. 6
Post-radioembolization overall survival based on the proposed threshold dose of 586 Gy in patients with localized PVI. A Optimal cutoff determination using the minimum p-value approach. B Overall survival of the patients with a tumor-absorbed dose > 586 Gy and those with a tumor-absorbed dose ≤ 586 Gy
Table 4 Retrospective multi-compartment dosimetry
Comments (0)