
Remember me






78 patients were identified. Patient characteristics are displayed in Table 2 with the denominator for each variable restricted to those with available data. The mean and median ages at presentation were similar at 50 years (range: 13–89) and 50.5 years (interquartile range: 43.25–59.75) respectively. A male predilection (F: M = 0.66) was noted; and the majority (68/76, 89%) presented to our institution with primary disease. Most patients (48/64, 75%) were treated surgically by EEA alone and received adjuvant radiotherapy (61/75, 81%), with only 13% receiving neoadjuvant radiotherapy.
Table 2 Patient characteristics and clinicopathologic featuresThe majority were either Kadish Stage B or C (13/69, 19%; and 45/69, 65% respectively). As such, tumors commonly (59/67, 88%) involved at least two sinonasal compartments. A significant proportion (27/69, 39%) had intradural extension. Extension into brain or cutaneous/soft tissue was noted in 12% (8/69) and 3% (2/69), respectively. About 9% (6/68) had nodal disease on presentation.
Grade and Other Histologic FeaturesOriginal Hyams grade was assigned in only 63% (43/68) of primary ONB. Modified Hyams grade could be assigned in 87% (59/68). The majority under both original and modified Hyams grade were grades II or III (38/43, 88% for original grade, and 55/59, 93% for modified grade). Notably under Modified Hyams grade, there were no cases assigned grade I.
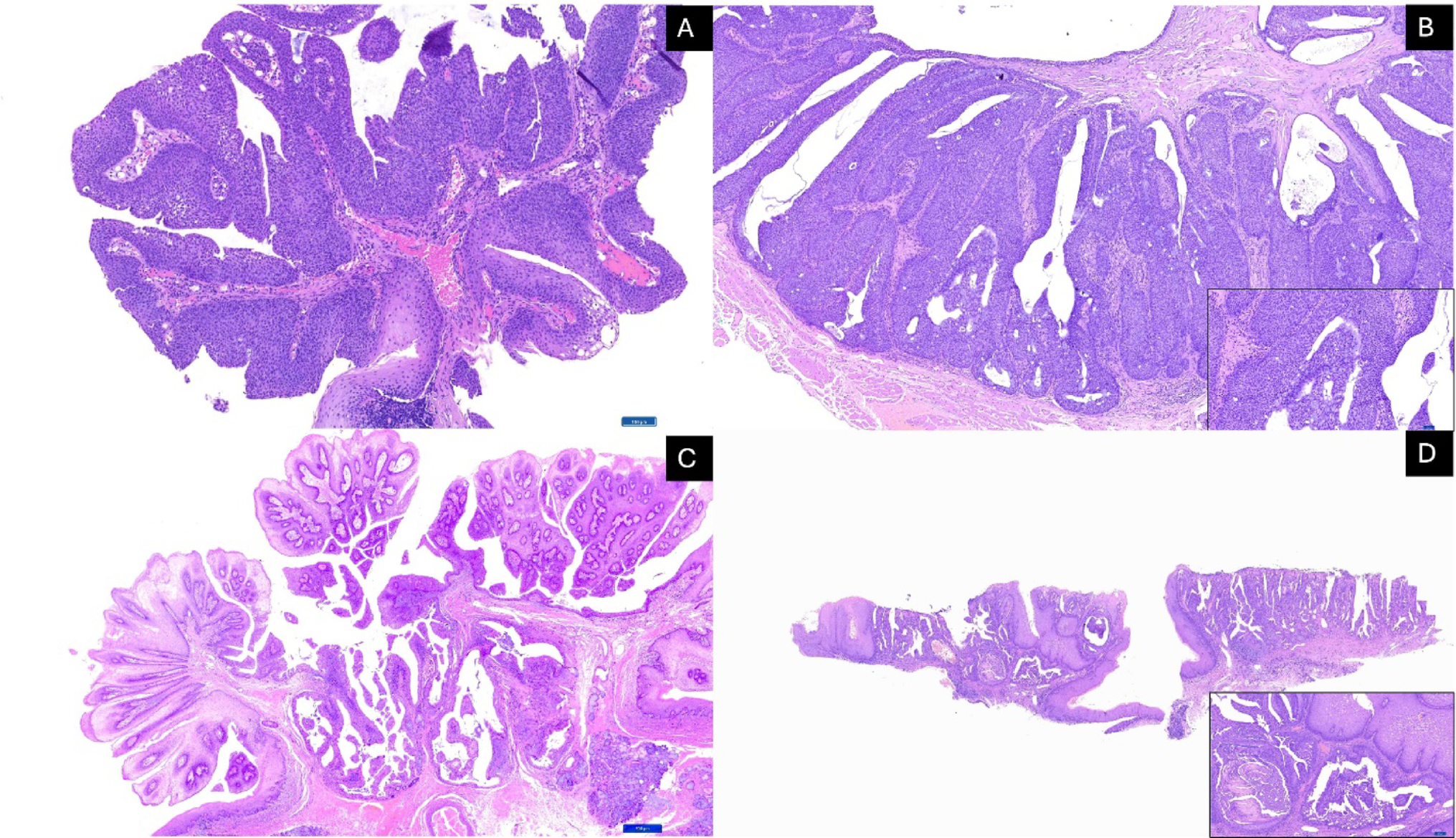
Figure 1 shows select cases displaying the spectrum of histologic maturation that was used to help define the grading categories for each histologic feature. Original Hyams grade distribution (in the 43 cases where it had been assigned at the time of initial diagnosis) was: I: 4 (9%), II: 27 (63%), III: 11 (26%), and IV: 1 (2%). Modified Hyams grade distribution on 59 cases was: II: 29 (49%), III: 26 (44%), and IV: 4 (7%) with no grade I cases.
Fig. 1
Morphologic features for Hyams grade parameters. A-C: Lobule and matrix characteristics. A- Large confluent fibrillary matrix rich lobules (10x). B- Smaller lobules with < 25% matrix (10x) C Infiltrative growth. D-G: Rosette types. D- Pinealocytomatous pseudorosettes (20x). E- Homer Wright pseudorosettes (40x). F- Flexner-Wintersteiner rosettes (40x). G- No rosettes or matrix (40x). H-J: Degrees of nuclear pleomorphism. H- Isomorphic with size variation < 2:1 (20x) I- Modest atypia with size variation ~ 2-<4:1 (20x). J- Severe atypia with nuclear size variation ≥ 4:1 (arrows– mitoses). K-L: Degrees of necrosis. K- Punctate (25x). L- Confluent (25x). M: Calcifications (10x)
Figure 2 depicts the flow of cases for which either Original Hyams or Modified Hyams grade were available (n = 65). Twenty-two cases did not have an Original Hyams grade assigned, however these were assigned a modified Hyams grade on histologic review. Conversely, six cases for which there was an original Hyams grade could not be reviewed and assigned Modified Hyams grade. For the 37 cases for which both systems were applied, only one case (3%) was downgraded by the Modified Hyams grade (III-> II). Thus, 8/37 (22%) were upgraded with two (5%) being two-step upgrades (I -> III, and II-> IV).
Fig. 2
Alluvial chart demonstrating flow of cases from original Hyams grade to modified Hyams grade. Only one case was downgraded by the Modified Hyams grade (III-> II) while 8 were upgraded with two being two-step upgrades (I -> III, and II-> IV)
Components of Hyams grade and other histologic parameters are stratified by grade grouping in Table 3. For grading parameters, only mitotic rate, pleomorphism and rosette type (specifically the presence or absence of rosettes) varied significantly between low- and high-grade groups.
Table 3 Histopathologic featuresOther key features are illustrated in Fig. 3. Clear cell/oncocytic change (53%, 31/59) and spindling (22%, 13/59) were not uncommon in our cohort, but did not vary significantly between grade groups though spindling was somewhat more frequent in high grade tumors. Similarly, ganglioneuromatous stroma though rare, did not vary between grade groups.
Fig. 3
Other morphologies. A) Clear cell (40x), and B) oncocytic (40x) change were fairly common. C) Spindle cell change was somewhat more common in high grade tumors (20x). D,E: Ganglioneuronal differentiation. D) Conventional ONB (top left) transitioning to a spindled stroma (4x). Inset: Scattered embedded ganglion cells (40x). E) The spindled stroma is S100 positive. Inset: A subset of ganglion cells was Neuronal nuclear protein positive (40x)
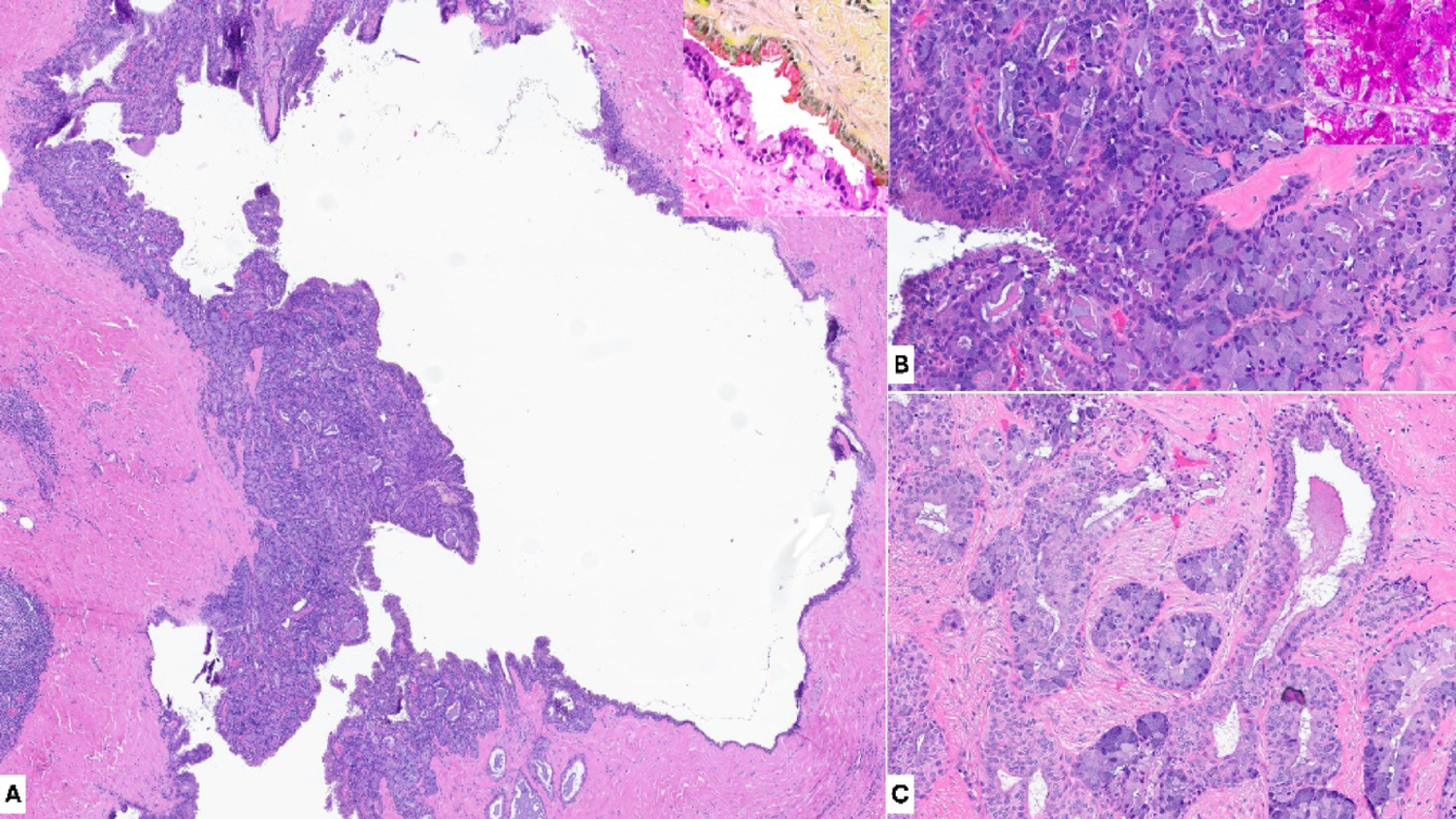
Only one case (2%) in the low-grade group showed a surface intraepithelial component. Epithelial interactions with seromucinous glands on the other hand were overall somewhat more frequent in the high-grade group, but not significantly so. While divergent epithelial differentiation was exclusive to the high-grade group, only three cases were noted (5%). The spectrum of epithelial interaction is shown in Fig. 4.
Fig. 4
Spectrum of epithelial interactions. A) Gland entrapment with glands showing prominent mucous cell predominance (10x). B) Gland entrapment with proliferative change with complex back-to-back seromucinous glands (10x). Inset (40x): The nuclei of the seromucinous glands are considerably smaller than those of the tumor (left of inset). C) Surface or intraepithelial involvement with accumulation of lesional cells basally (10x). Inset (20x): Intraepithelial component highlighted by an SSTR2 immunostain. D-F: Olfactory neuroblastoma with divergent epithelial differentiation (olfactory carcinoma). D) Anastomosing reticular patterned eosinophilic epithelium admixed with the ONB component (10x, inset: 40x). E) The tumor shows synaptophysin staining of the ONB component (10x) along with S100 staining of sustentacular cells (inset: 10x). F) Cytokeratin AE1/3 highlights an inverse pattern, restricted to the epithelial component
Perineural, lymphatic/vascular and bone invasion showed no difference in prevalence in each grade group.
OutcomesFive-, ten- and twenty-year overall survival (OS), disease specific survival (DSS), and disease-free survival (DFS) are summarized in Table 4 and Kaplan Meier Curves in Fig. 5. Median follow-up on live patients was 121.8 months (range: 0.2-309.4 months). Complete Cox univariable analysis of prognostic variables in terms of OS, DSS, and DFS is shown in Table 5. Significant adverse prognostic features for OS on Cox univariable analysis were: transcranial approach [Hazard Ratio (HR):8.012, (95% confidence interval (CI):1.48-30.487), p = 0.02], and brain invasion [HR:4.462 (95%CI:1.067–20.303), p = 0.041], with age being nearly significant [HR:1.03 (95% CI:1-1.06), p = 0.05]. Significant adverse prognostic features for DSS were: severe nuclear pleomorphism [HR: 8.092 (95% CI:1.329–83.564), p = 0.024], combined approach [HR:6.713 (95%CI:1.519–26.229), p = 0.015], and transcranial approach [HR:8.092 (95%CI:1.329–83.564), p = 0.024], with brain invasion being nearly significant [HR: 5.08 (95%CI:0.97-31.032), p = 0.054]. Significant adverse prognostic features for DFS included: severe nuclear pleomorphism [HR:3.81 (95%CI:1.125–12.902), p = 0.033], combined approach [HR:4.014 (95%CI:1.177–11.596), p = 0.029], transcranial approach [HR:9.687 (95% CI:1.786–36.877), p = 0.013], Kadish-Morita Stage C [HR: 8.069 (95% CI:1.11-NA), p = 0.035], Kadish-Morita Stage D [HR:17.433 (1.842-NA), p = 0.009], intradural invasion [HR:5.553 (95%CI:1.941–21.365), p = 0.001], and brain invasion [HR: 7.103 (95%CI:1.64-33.638), P = 0.01].
Fig. 5
A) OS, B) DSS, and C) DFS in ONB. For each figure, the solid grey drop-down line is 5-year survival, dark grey dashed line is 10-year survival, and black dotted line is 20-year survival
Table 5 Cox univariable analysis of prognostic variables in terms of overall survival (OS), disease specific survival (DSS), and disease-free survival (DFS)Neither Original Hyams Grade nor Modified Hyams grade show significant prognostic value in terms of OS, DSS, or DFS, nor did any individual histologic parameter aside from nuclear pleomorphism noted above. However, Modified Hyams grade did progressively increase in HR for all endpoints in contrast to Original Hyams grade, for which the HRs for grades II-IV were actually lower than the reference (grade I). Dichotomizing into low (grade I-II) and high grade (III-IV) also did not show a significant difference by Kaplan Meier method (Fig. 6) for either grading system, but separation of curves was qualitatively superior for the Modified Hyams grade with DFS between low and high-grade showing a trend towards significance (Log rank p = 0.088). By Kaplan Meier method, nuclear atypia across degrees (mild, moderate, severe) showed a trend towards significance for both DSS (p = 0.059), and DFS (p = 0.088).
Fig. 6
OS, DSS, and DFS by grade and nuclear pleomorphism. A-C: Original Hyams grade OS, DSS, and DFS respectively. Note the crossover of KM curves for DFS in C. D-F: Modified Hyams grade OS, DSS, and DFS. G-I: Nuclear pleomorphism OS, DSS, and DFS
The final multivariable Cox regression model for DFS is summarized in Table 6 and includes age, procedure type, nuclear pleomorphism, and Kadish-Morita Stage. Only procedure type (combined and transcranial approaches) remained significant prognosticators [HR:8.616 (95%CI:2.052–37.138), p = 0.004, and HR: 17.559 (95%CI:1.727–175.65), p = 0.017, respectively]. Kadish-Morita Stage D was nearly significant [HR:14.35 (95%CI:0.963-NA), p = 0.054].
Table 6 Multivariable Cox regression model for disease free survival
Comments (0)