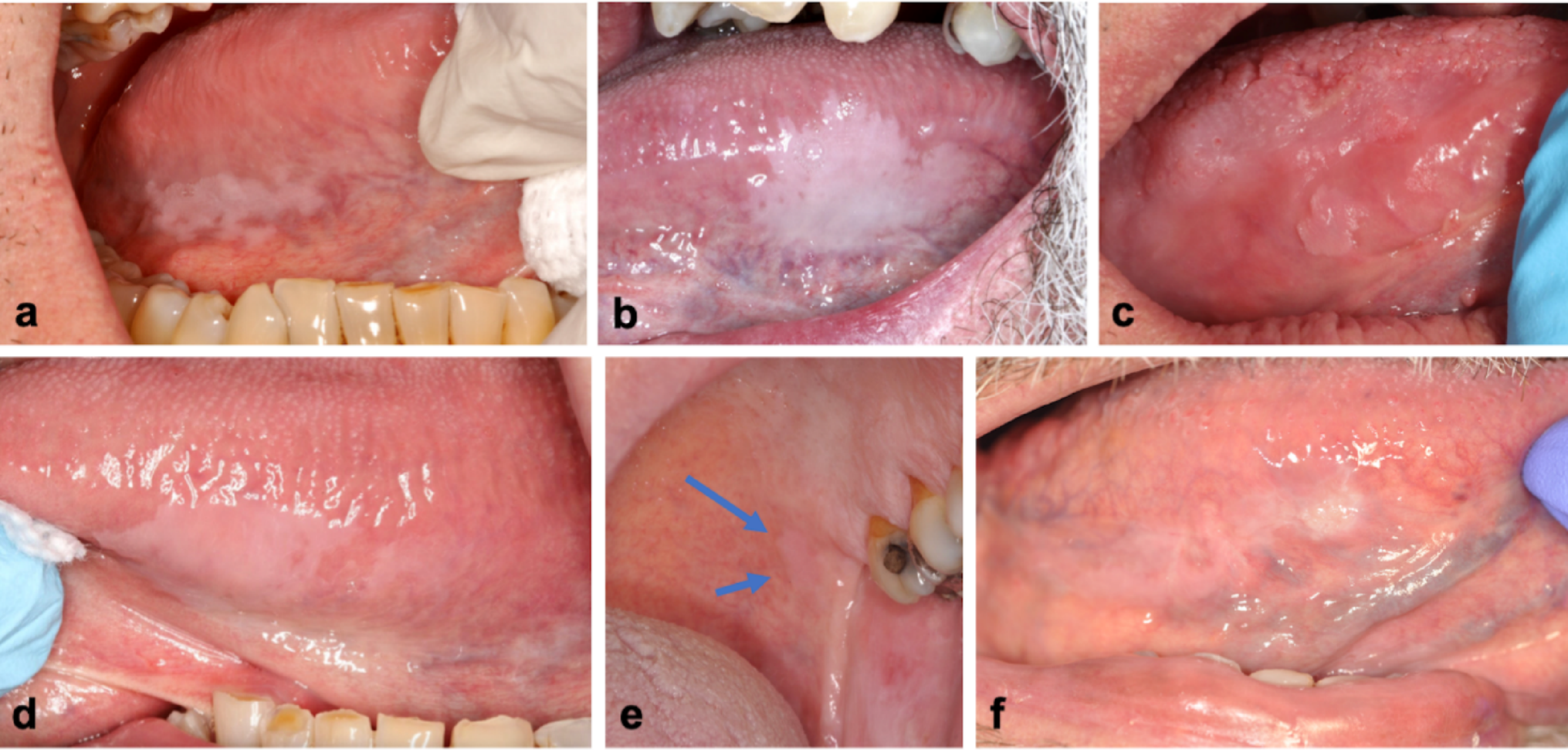
The detection of a submucosal swelling arising in the floor of the mouth should prompt clinicians to initially rule out any infectious or non-infectious odontogenic processes first. Then, other common pathoses within the clinical differential diagnosis of such a presentation would include salivary gland inflammatory lesions (ranula, sialadenitis, sialolithiasis), developmental entities (dermoid cyst, epidermoid cyst), or primary soft tissue neoplasms, such as benign (lipoma, rhabdomyoma, schwannoma) or malignant lesions (squamous cell carcinoma, mucoepidermoid carcinoma, adenoid cystic carcinoma, polymorphous adenocarcinoma, rhabdomyosarcoma).
Historically, LGFMS had been included in a group of hyalinizing spindle cell tumors (HSCT) with giant rosettes and an indolent growth in the early follow-up period [11]. This distinction was functionally erased by a comprehensive clinicopathologic study by Folpe et al., which reevaluated a large cohort of cases and demonstrated that LGFMS and HSCT were opposing ends of the same disease spectrum [5]. This conclusion was later conclusively proven by the identification of the shared FUS::CREB3L2 chromosomal translocation t(7;16)(q33;p11), establishing them as a single biological diagnosis [12]. Longer-term follow-up assessments of LGFMS also revealed their significantly increased potential for metastasis [13, 14].
Another nosological confusion was the consideration that LGFMS represented a histomorphological variant of sclerosing epithelioid fibrosarcoma (SEF) [15]. While LGFMS is defined by the FUS::CREB3L2 gene fusion and SEF by EWSR::CREB3L1 fusion, the presence of some microscopic features alone was unsatisfactory, blurring the lines of distinction and confidence with classification. As such, a significant diagnostic challenge exists with many of the earlier published cases of LGFMS of the head and neck, as they lacked modern molecular or IHC supportive testing, and should be interpreted with caution. At present, SEF is characterized by its greater aggressive biology, older age of onset, increased tendency for metastasis, poorer prognosis, and varied gene expressions [9].
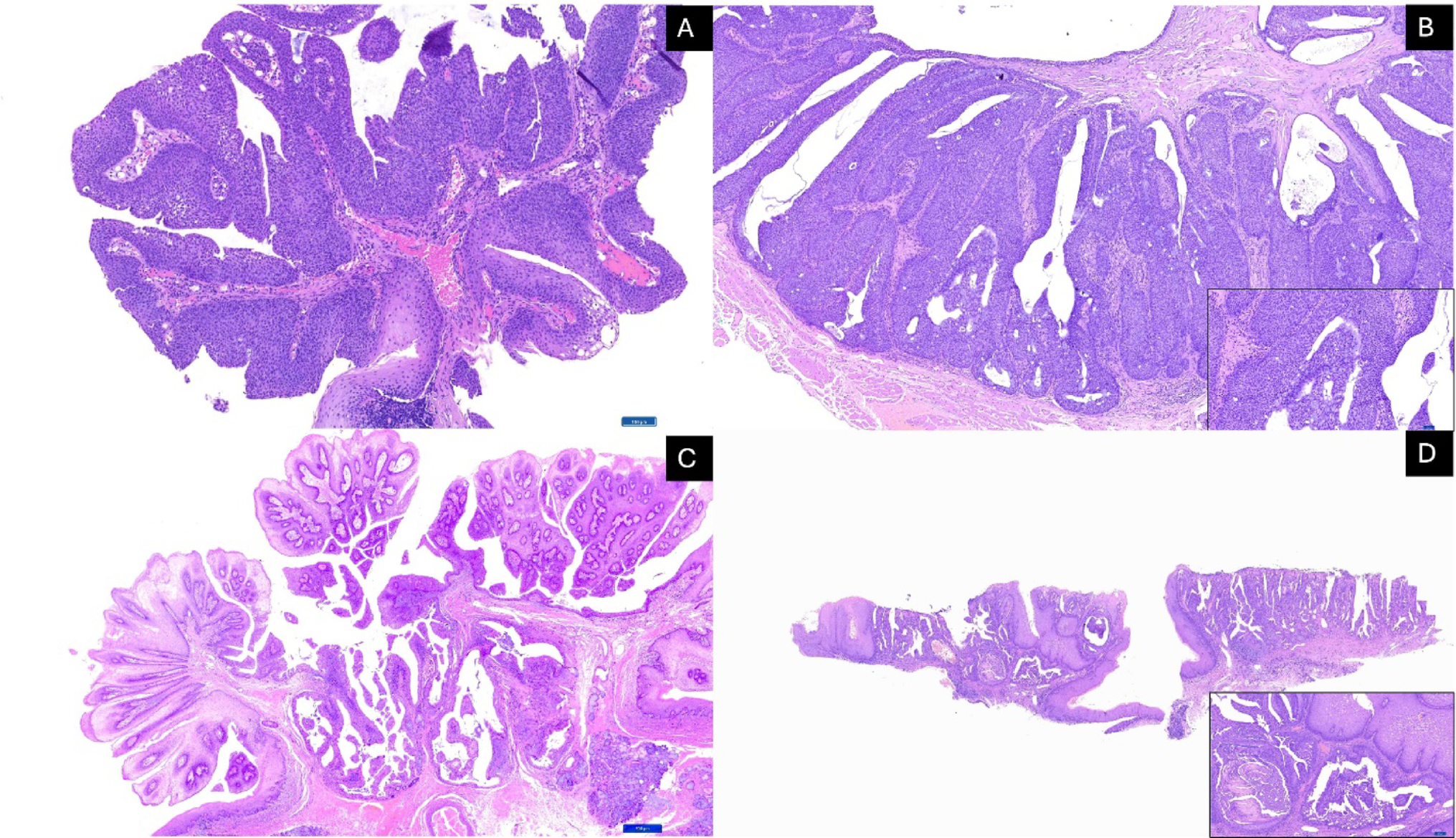
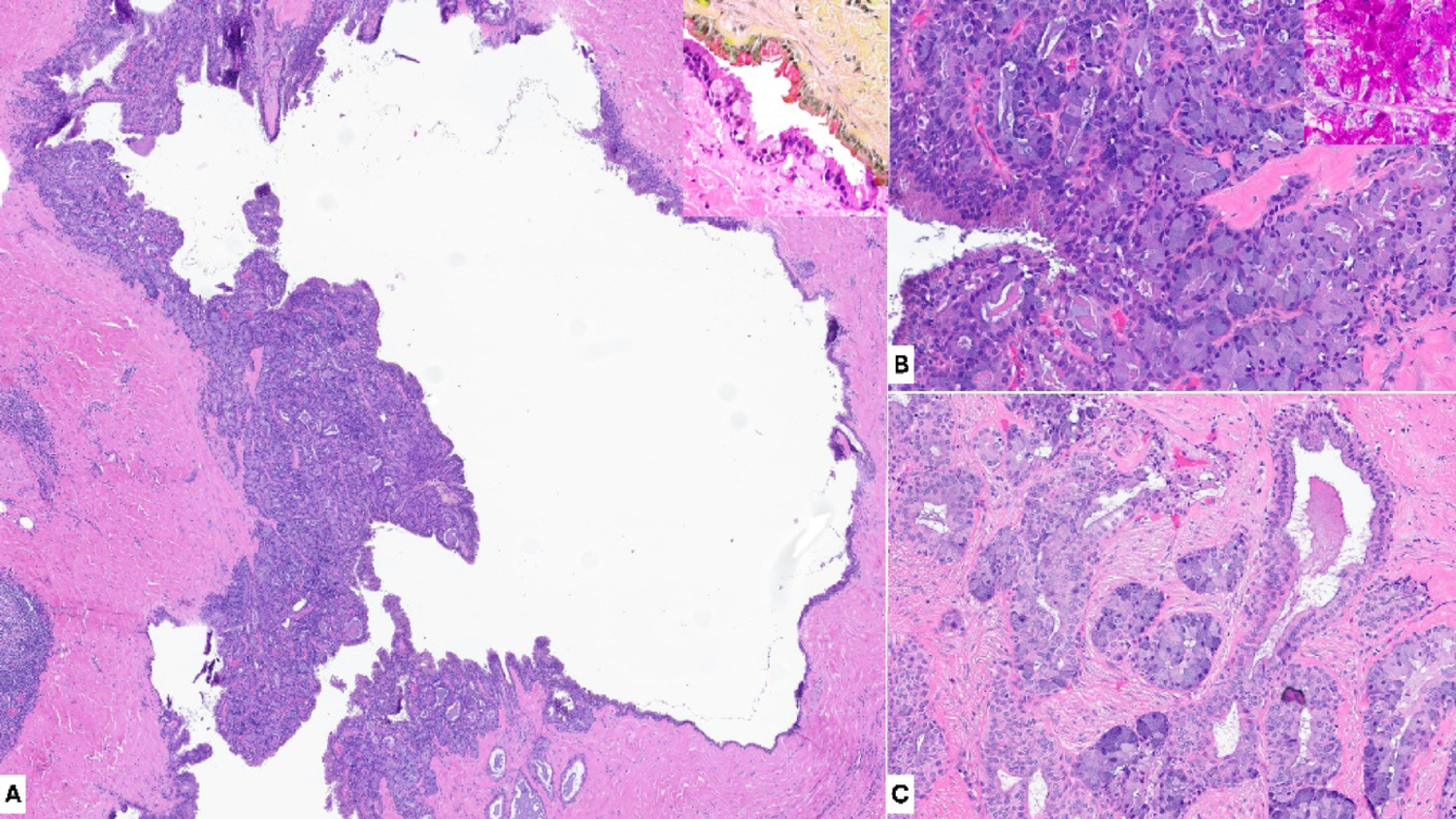
Histologically, LGFMS overlaps with a broad category of fibroblastic spindle cell neoplastic entities, characterized by bland spindle cells arranged in a whorled pattern within alternating collagenous and myxoid areas, and lesions may exhibit gross infiltration into surrounding tissues [16]. MUC4 has proven to be a sensitive IHC diagnostic tumor marker, in combination with the negativity of S100, desmin, caldesmon, cytokeratin, SMA and CD117, which aid in excluding other morphologically overlapping entities, including malignant peripheral nerve sheath tumor, nodular fasciitis, and other myxoid spindle cell tumors (such as myxoid neurofibroma and perineurioma) [6, 17].
Nonetheless, some LGFMS cases confirmed by FUS::CREB3L2 gene fusion on molecular analysis have shown MUC4 negativity [18]. Consequently, the reported descriptive features overlapped considerably with several benign and low-grade malignant spindle cell lesions, particularly neurofibroma, fibromatosis, and low-grade myxofibrosarcoma. MUC4 immunoreactivity is highly sensitive for LGFMS but has also been reported in other neoplasms, such as glandular cell populations occurring in synovial sarcoma, malignant ossifying fibromyxoid tumor, and SEF, indicating that this biomarker and the overlapping spectrum of fusion variants are not entirely specific for LGFMS [6, 19,20,21,22]. Moreover, hybrid LGFMS/SEF tumors have been reported with overlapping EWSR1::CREB3L1 gene fusions and demonstrated positive MUC4 immunoexpression [20, 23].
Demographically, overall case series of LGFMS have shown a slight male predominance [14, 24, 25] or with near-equal sex predilection [7, 10, 26], with a mean age at diagnosis of 32.7 to 38.6 years (range: 2 to 98 years) [7, 9, 14, 25]. The majority of tumors have been found in the deep soft tissue sites of the lower extremities, trunk wall, and viscera [7]. Within the head and neck, most cases of LGFMS have been located with the soft tissues of the neck, with fewer lesions involving the face, ear, oropharynx, tongue, salivary glands, palate, maxillary/ethmoid sinuses, and buccal/labial mucosa; intraosseous sites have mainly involved the jaws and less often with orbit and intracranial extension [7, 27, 28]. The diagnosis of LGFMS is rare and typically relies on correlation between CT/magnetic resonance imaging and histopathological examination, and confirmed by molecular analysis.
Despite its bland microscopic appearance, long-term follow-up evaluations of LGFMS have been reported with rates of recurrence of 25.8 to 66.6% (with median age at diagnosis of 3.2 to 3.5 years) and risk of distant metastasis of 18.5% [2, 7, 14]. Isolated cases of LGFMS have metastasized from 45 to 50 years from initial pathologic diagnosis [2, 5]. Sites of metastatic spread of LGFMS have mainly involved the lung, pleura, and bone [2, 5]. Thus, the significant risks of late recurrence and metastasis potential emphasize the need for indefinite surveillance [7, 29]. The primary modality of treatment has involved wide en bloc surgical resection, although radiotherapy or chemotherapy has been utilized in severe or recurrent cases [7, 26]. Incident death associated with LGFMS has varied widely, from 3.2% of (6/186) to 42.4% (14/33) of patients with follow-up periods ranging from 3 months to 50 years [5, 14].
Our literature search yielded only 22 cases of LGFMS (including our featured case), within the head and neck that included genetic results, limiting rigorous clinicopathologic analysis; 18 of these published cases included treatment outcomes, and have been summarized in Table 1 [2, 6, 7, 12, 24,25,26, 30,31,32,33,34,35,36,37]. None of the affected patients died of disease. All patients were initially managed with surgically (biopsy and/or excision), with margins ranging from < 1 mm to 1 cm. Sixty-percent of patients (15/22) remained without evidence of disease at last follow up (ranging from 1 month to 21 years). However, 4 patients developed tumor recurrence, resulting in a recurrence rate of 22.2%, ranging from 3 to 156 months [2, 25, 30]. Notably, 2 patients had minimal or uncertain tumor margins, 1 of whom experienced recurrence at 156 months and developed lung metastasis [30]. One case of LGFMS of the mandible underwent transformation to SEF at 20 years (with unstated outcome) [35]. Three cases underwent surgery (1 each: biopsy, en bloc resection, excisional biopsy) and received supplemental radiotherapy, resulting in 1 patient with recurrence at 3 months, 1 alive with disease at 48 months, and our patient, who had prophylactic radiotherapy due to concerns about adequate tumor margins) and demonstrated no evidence at 1 year [25, 26]. Giani et al. proposed that affected patients with incomplete resection and minimal tumor-free margins will likely benefit with follow-up radiotherapy [29].
Table 1 Reported cases of low-grade fibromyxoid sarcoma with molecular findings in the head and neck regionTo our knowledge, the presented case is the first published account of LGFMS arising in the floor of the mouth and confirmed with FUS::CREB3L2 fusion. At a 1-year postoperative assessment, Signatera testing indicated no detectable tumor ctDNA. It remains unclear whether the negative result with Signatera at the 1-year follow-up offered any long-term prognostic benefit. A recent preliminary study of various soft tissue sarcomas showed that use of this diagnostic modality offered comparable measures of tumor progression with radiologic imaging [38]. In addition, other investigations have corroborated its prognostic utility, such as with undifferentiated pleomorphic sarcoma [39], uterine malignancies [40], and a diversity of pediatric solid tumors [41]. As far as could be ascertained, this article represents the first published case report on the employment of the Signatera assay for postoperative surveillance of LGFMS of the head and neck.
There are several limitations with this report, principally with the clinical utility of a novel case and the short-term (1-year) postoperative follow-up. Furthermore, the prognostic applicability of the molecular analysis and postoperative biomarker assay should be viewed with caution in the context of single cases. It is advocated that more cases of LGFMS of the head and neck are published that contain enhanced diagnostic and prognostic techniques.







Comments (0)