Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and its variants have caused COVID-19, a highly infectious disease that has led to a pandemic starting in 2019 and lasting over three years, resulting in more than 6 million deaths worldwide [1, 2]. Remdesivir has been established as a safe treatment for patients with COVID-19 [3]. Additionally, ritonavir-boosted Nirmatrelvir, Molnupiravir, and high-titer COVID-19 convalescent plasma have emergency authorizations for treating this disease [2, 3]. Given the random mutations of SARS-CoV-2 and the limitations of existing vaccines, guidelines are frequently updated to incorporate newly emerging therapies that demonstrate greater efficacy [4].
Whether therapies will remain effective against SARS-CoV-2 mutations remains an open question [5]. The 3-chymotrypsin-like (3-CL) protease of SARS-CoV-2 cleaves the viral polyproteins pp1a and pp1ab to produce functional viral proteins and stabilize substrate-binding pockets [6, 7]. As an important target for small-molecule therapies, it may play an important role against newly emerging variants [8]. Consequently, SARS-CoV-2 3CL protease inhibitors have emerged as promising therapeutic candidates for the treatment of patients with mild to moderate COVID-19, given their potential effectiveness against both current and future variants [7]. However, these individual trials had a small sample size and statistical power, which limits generalizability of their findings [9,10,11].
Despite the availability of antiviral agents and monoclonal antibodies, the emergence of new SARS-CoV-2 variants with potential resistance mechanisms has underscored the need for broadly effective antiviral strategies. Notably, agents such as Nirmatrelvir, Simnotrelvir, Olgotrelvir, Ensitrelvir, and Leritrelvir are examples of 3CL protease inhibitors that have been evaluated in clinical trials designed to assess their safety and efficacy in patients with COVID-19 [7, 10, 12,13,14,15,16]. Therefore, we aimed to perform a systematic review with meta-analysis of randomized controlled trials (RCTs) comparing the efficacy and safety of SARS-CoV-2 3CL protease inhibitors with placebo in patients with mild and moderate COVID-19, to elucidate their therapeutic role.
Methods
This systematic review and meta-analysis were performed and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement guidelines and the Cochrane Collaboration Handbook for Systematic Reviews of Interventions guidelines [17, 18]. The prospective meta-analysis protocol has been uploaded to the International Prospective Register of Systematic Reviews (PROSPERO; CRD42024562860).
Eligibility criteria
Inclusion in this meta-analysis was limited to studies that met all the following eligibility criteria: RCTs; enrolling patients with COVID-19 with mild or moderate symptoms; comparing 3CL protease inhibitors with placebo; reporting at least one of the outcomes of interest, and COVID-19 diagnosis requiring confirmation by RT-PCR or other approved molecular testing methods. Mild-to-moderate COVID-19 was defined according to the original criteria of each study. In general, mild cases included symptomatic patients without respiratory compromise, while moderate cases involved evidence of lower respiratory tract involvement (e.g., cough, dyspnea, or radiographic abnormalities) with oxygen saturation (SpO₂) > 93% on room air and no need for supplemental oxygen [19]. The 3CL protease inhibitors considered included RAY1216, Simnotrelvir, Nirmatrelvir, GST-HG171, Ensitrelvir, and Olgotrelvir. There were no restrictions on language or publication date. Observational studies, studies with overlapping patient populations, without a control group, head-to-head comparisons between 3CL protease inhibitors, abstracts, editorials, letters to the editor, preprints, reviews, systematic reviews, and meta-analyses were excluded.
Search strategy and study selection
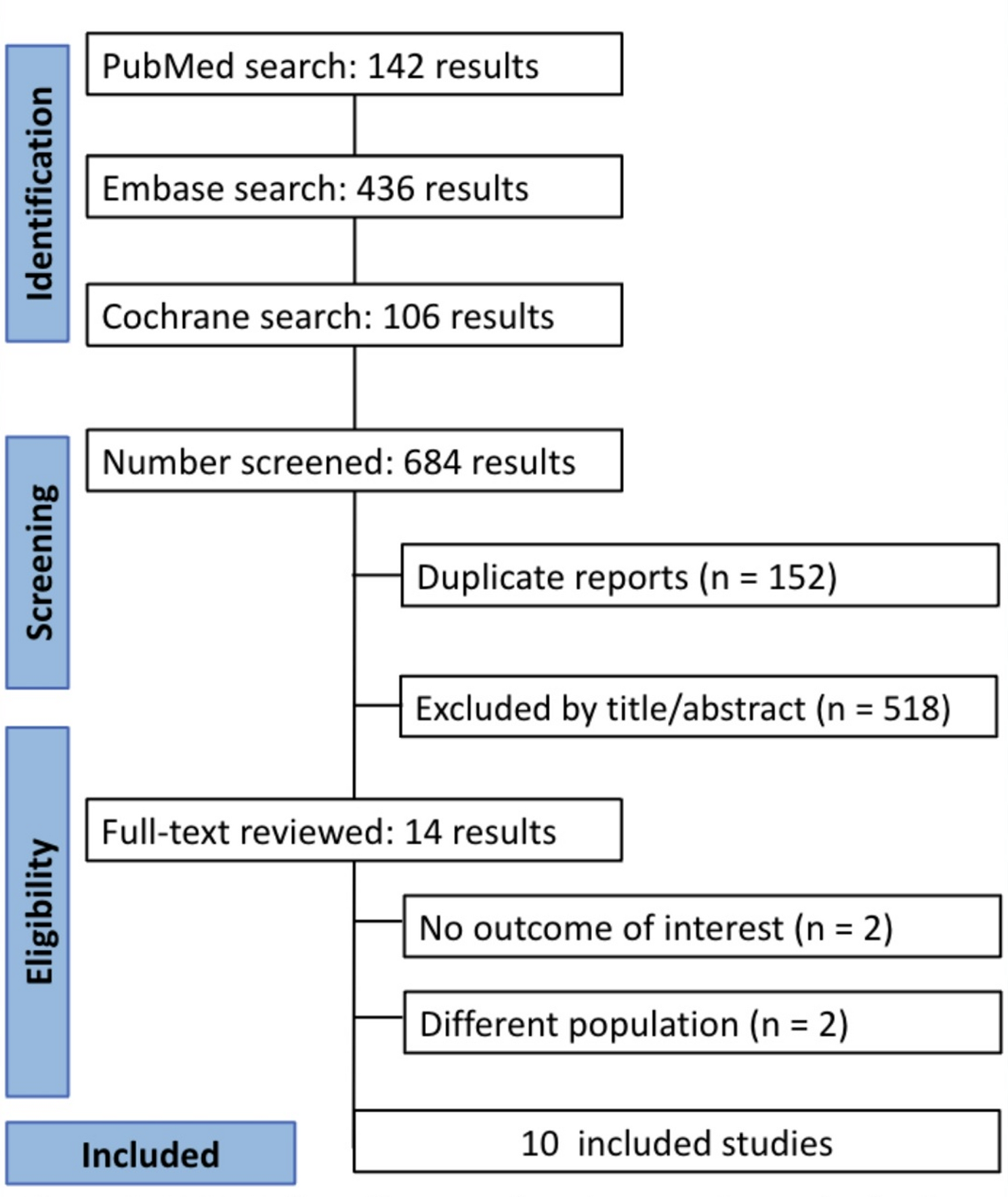
We conducted a systematic review of PubMed, Embase, and Cochrane Library on April 1st, 2024. The search strategy was adapted to the different databases according to support for special characters. References of eligible papers, previous systematic reviews, and meta-analyses were also searched for additional studies of interest.
Two reviewers (C.F and W.N) conducted the search, imported results into Rayyan software, and triaged the studies. After excluding duplicates and titles/abstracts unrelated to the clinical question, we assessed the eligibility of each remaining study based on a full-text review of the articles. In instances of disagreement, we consulted a third reviewer (N.L). A full description of our search strategy can be found in Supplementary Methods 3.
Data extraction
Two independent authors (C.K e W.N) extracted the data in a double-blinded method; in case of any conflict, a third author was consulted. The following data from individual studies was extracted: (1) country; (2) blinding method; (3) number of patients; (4) type of 3CL protease inhibitor; (5) dosage; (6) follow-up in days; (7) mean age; (8) sex distribution; (9) vaccination status proportion; (10) proportion of patients with risk factors for severe COVID-19; (11) proportion of patients with Covid-19 symptoms at baseline; (12) proportion of patients with stratified genetic variants; and (13) initial virus copy number. A full disclosure on how the Kaplan-Meier Curve extraction was performed can be found in our Supplemental Methods 4.
Endpoints and subgroup analysis
We defined our primary endpoints as the number of patients with symptomatic resolution, viral Ribonucleic Acid (RNA) loading change from baseline, and any adverse events. We collected data on the following secondary endpoints: recovery rate, sustained alleviation rate, and severe/serious adverse events.
We performed a prespecified subgroup analysis of low-dosage (125 mg) versus high-dosage (250 mg) on patients undergoing Ensitrelvir for the viral load endpoint. A full definition of the outcomes can be found in Supplementary Methods 5. Additionally, a post-hoc subgroup analysis was conducted between the different 3CL-inhibitors drugs for the symptomatic resolution endpoint.
Risk of bias and evidence quality assessment
Six authors (N.L., E.K., C.F., W.N., A.C., and H.F.) conducted the risk of bias assessment in pairs with a double-blind model. Risk of bias in selected randomized trials was assessed using the second version of the Cochrane Risk of Bias assessment tool (RoB 2) [20], evaluating five domains for each outcome of the selected studies: (I) bias in the randomization process; (II) bias due to deviations from intended interventions; (III) bias due to missing data; (IV) bias in outcome measurement; and (V) bias in the selection of the reported results.
The overall risk of bias assessment for each trial outcome was derived from individual domain judgments. After discussing the reasons for the discrepancy, disagreements were resolved through consensus. We also performed funnel plot analysis to appraise publication bias [21].
Statistical analysis
Statistical analyses were conducted using R (R Foundation for Statistical Computing, Vienna, Austria) version 4.3.2 under the “meta” package [22]. Restricted Estimated Maximum Likelihood (REML) random-effects models were employed for data synthesis. Treatment effects for dichotomous endpoints were compared using Risk ratio (RR) with corresponding 95% confidence intervals (CI), while continuous outcomes were assessed using Standardized Mean Difference (SMD). Time-to-event outcomes, such as recovery and symptom alleviation rates, were calculated using Hazard Ratio (HR) and 95% CIs. Statistical significance was defined as a p-value < 0.05. Heterogeneity was evaluated through I² statistics and Cochran’s Q test, with significance defined as p < 0.10 and I² >40%. Sensitivity analyses were conducted to ensure the robustness and reliability of the findings for outcomes with high heterogeneity.
Trial sequential analysis
We used the TSA 0.9.5.10 Beta software for trial sequential analysis (TSA) [23] to confirm our meta-analysis results. The type of boundary value for the hypothesis test was set to a two-sided test with an alpha value of 5%. Once the cumulative studies in the Z-curve cross the conventional monitoring boundary or the futility area, the results are consistent and should be considered reliable evidence.

Comments (0)