There are different types of studies to analyze the resorption of primary molars, although not many are performed when there is agenesis of the successor premolar. In the case of dental agenesis, notable studies include those of Bjerklin and Bennet [9], Rune and Särnas [15], Kurol and Thilander [16], Ith-Hansen and Kjaer [17], Nordquist et al.[18] and Hvaring and Birkeland [19]. Ideally, a longitudinal prospective study should be performed [10, 15,16,17, 19], but this requires periodic radiographs for research purposes, which is not accepted by current radiation protection protocols [20, 21]. Therefore, the present study is cross-sectional and retrospective, a methodology validated by multiple previous studies [18, 22,23,24].
For sample selection, the criteria applied in this study are similar to those of other authors, such as Haselden et al. [23] or Calheiros-Lobo et al. [25]. The minimum age chosen was 6 years, since, according to previous studies, resorption of the 2Pr begins around that age [11, 13, 26, 27]. However, other authors point out that a precise diagnosis of 2Pr agenesis cannot be made with certainty until the age of 9–10 years, as these teeth may calcify late [28].
We aim to provide qualitative and quantitative values for root resorption. Similar to our study, orthopantomography has been the complementary test used by other authors in their studies for making measurements, especially when studying the molar region, where the distortion that can be presented by radiography is minimal [16, 17, 19, 22,23,24,25, 29]. Also, we have used panoramic radiographs, as they are used in pediatric dentistry as diagnostic records.
Regarding premolar agenesis, in the Spanish population, Vaquero-Niño et al. [30] estimated a prevalence of 4.9%, while Hernández Guevara [31] reported 4.1%. More specifically, when we talk about 2Pr, in our study, the prevalence of agenesis drops to 3.4%, with 50% of cases being bilateral. These results coincide with those offered by other authors, who report a prevalence ranging from 2.4 to 4.3%, with 60% of cases being bilateral [9, 10, 32]. However, other studies indicate that unilateral 2Pr agenesis is more common than bilateral [33] Regarding sex, in our study, the number of women with agenesis was almost double that of men (33 men and 61 women), consistent with eight of the studies reviewed [9, 10, 15, 22,23,24,25, 29].
Finally, the present study comprised 174 p2m from 94 patients. Reviewing the literature, we observed great variability in sample sizes. The study presented by Hvaring et al. [24], where they studied 188 p2m from 111 patients, resembles the sample size of this study.
To measure rhizolysis, the graphical method described by Bjerklin–Bennett in 2000 was used [9]. This method has been employed in other studies for analyzing root resorption in cases of agenesis [10, 18, 19, 24, 25]. The results differ from those; of Bjerklin and Bennett [9] and Bjerklin et al. [10]. However, they resemble those of Hvaring et al. [24], because both studies used orthopantomograms and had very similar data for healthy and filled molars.
When analyzing root resorption using the graphical method and its relationship with sex, no significant differences were observed for the mesial root. However, highly significant differences were found for the distal root, with a higher number of unresorbed roots in men. There was a greater difference in women when root resorption was 1/4. Other authors who used graphical methods to analyze resorption found no relationship between sex and resorption of both mesial and distal roots [15, 18, 19, 23]. We also found no differences when analyzing mesial root resorption using the numerical method, but we did find differences for the distal root.
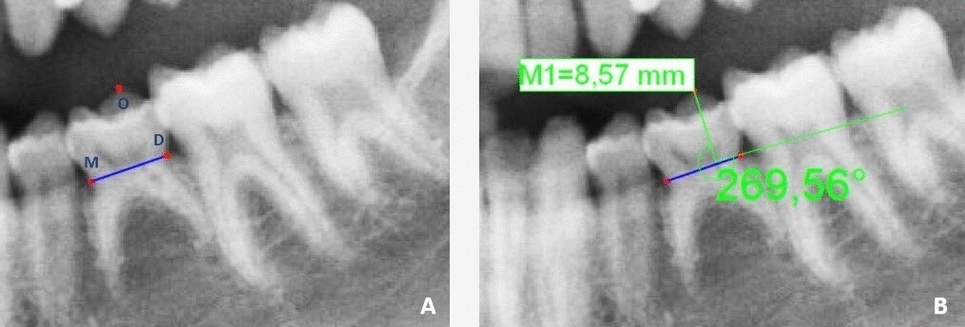
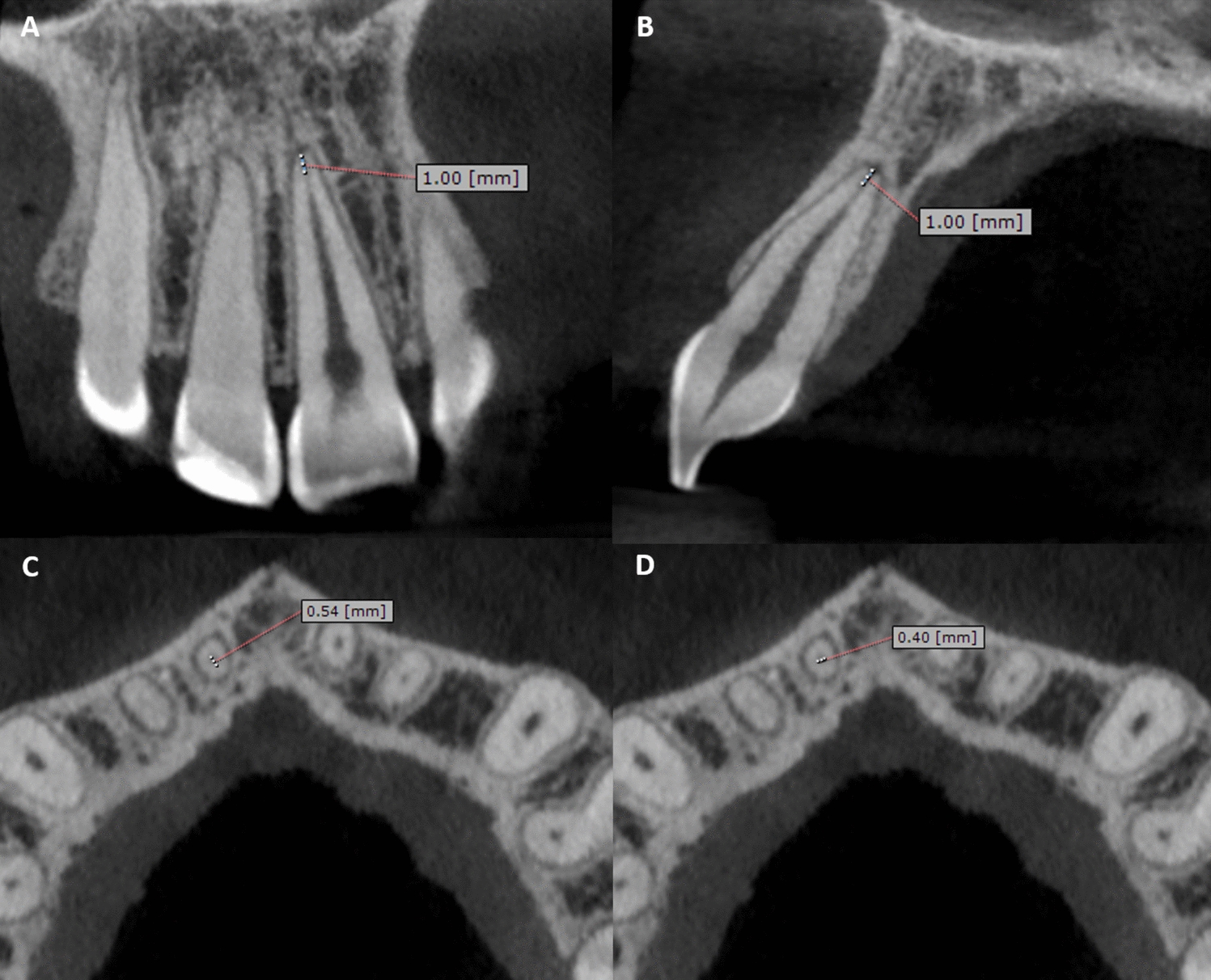
Along with the graphical method, which can sometimes be subjective, we have used a numerical method that allows comparison of linear measurements with non-variable structures (coronal height) and minimizes phenomena, such as magnification, head position, differences between sexes, or racial differences. We use a numerical method based on ratios or proportions which was used to measure root resorption of p2m, but without agenesis [14].
Comparing the results with those of Caleya et al. [14], the mean ratio for the age range of 6–9 years in this study resembles theirs for both roots. This could be interpreted as similar resorption in this age group regardless of the presence or absence of dental germ. For the age group of 9–12 years, the ratio in this study is higher, indicating a delay in root resorption in cases of agenesis compared to resorption in the presence of a germ. The mesial and distal ratios for men are higher than those for women, very similar to the results of Caleya et al. In their study, they also indicated that there were differences in the ratio by sex. However, when we analyzed the distal root by ratios, we did not find statistically significant differences in terms of sex. The fact that the ratio for males is higher than that for females could indicate that the roots of males undergo slower resorption, which would coincide with the results of the graphical method for the distal root.
Since we do not coincide either in the method used or in the classification of infraocclusion, we cannot make direct comparisons with other authors.
Studies that analyze root resorption in cases of agenesis of the permanent successor, with the exception of Haselden et al. [23] examined how infraocclusion influences them. However, not all of them used the same method to assess infraocclusion, nor the same classification as we did in this study, making it difficult to make direct comparisons with our results. Rune and Särnas [15] found no relationship between infraocclusion, sex, caries and resorption, as did Nordquist et al.[18]. Kurol and Thilander stated that the progression of infraocclusion of those molars with agenesis is greater than when the germ is present [16]. Hvaring et al. [24] like Garib et al.[22] found a relationship between infraocclusion and root resorption, with infraocclusion and resorption increasing with age.
Another variable analyzed was whether the resorption of the p2m with agenesis of the successor could be altered when it suffered from any pathology. It has been observed that, with both methods, healthy p2m undergo less resorption than those with fillings or decay. In this aspect, we differ from Rune and Särnas [15] and Nordquist et al.[18] as they stated that there was no relationship between resorption and the presence of cavities or restorations.
Regarding comparing the resorption of p2m with agenesis of the successor with the contralateral without agenesis, as far as we have reviewed, we have not found any publication that analyzes it. There are studies that claim that when there is agenesis of the successor, resorption occurs more slowly or starts later [3, 4, 11, 12, 34, 35]. However, in our study, due to the sample size available to us, although we have compared all cases of unilateral agenesis, we cannot affirm that there are differences in the resorption pattern.
We are aware that our study has a significant limitation in that it is a cross-sectional study. A longitudinal study would be the ideal design to study a process that occurs over time, but multiple sequential radiographs of participants would be required, which is ethically controversial.
One of the greatest strengths of our study is the large sample size achieved to calculate the prevalence of second premolar agenesis. Another strength to highlight is that the previous studies only used graphical methods for analyzing resorption, whereas we used and compared two methods. Another aspect to emphasize is the large number of radiographs analyzed, all performed with the same X-ray machine. With this research, we aim to provide data to predict the survival of a molar with agenesis of permanent successor without the need for multiple sequential radiographs.


Comments (0)