
Remember me

A core multidisciplinary team of Surgeons, Anaesthetists, and Nurses participated in the ‘Enable Quality Improve Patient Care (EQuIP)’, a Stanford-India Collaborative Quality Improvement (QI) training project from 2023 to 2024. Other team members included the Quality Training Program mentors (two institutional). This study was undertaken as a QI initiative at Tata Memorial Centre, Mumbai, rather than human participant research. The study was conducted according to the Declaration of Helsinki, as revised in 2013. Institutional Ethics Committee approval has been obtained for this study.
The problem statement for the project was the lack of identification of NAPS as a problem by the stakeholders (Surgeons, Anaesthetists and Nurses). We also did not have the actual incidence of NAPS at our institute before initiating this study and, subsequently, the lack of understanding of probable predisposing factors. We started with setting two SMART (Specific, Measurable, Achievable, Relevant, and Time-Bound) goals: firstly, to understand the incidence of NAPS, sensitise the existence of this problem to stakeholders, And consider this as a measure of the quality of care delivered to our patients. Secondly, we wanted to identify predisposing factors for the development of NAPS And reduce the overall incidence of NAPS to less than 10% of its current incidence (once identified) in 3 months. The team met fortnightly during the project and attended online lectures on various steps of QI.
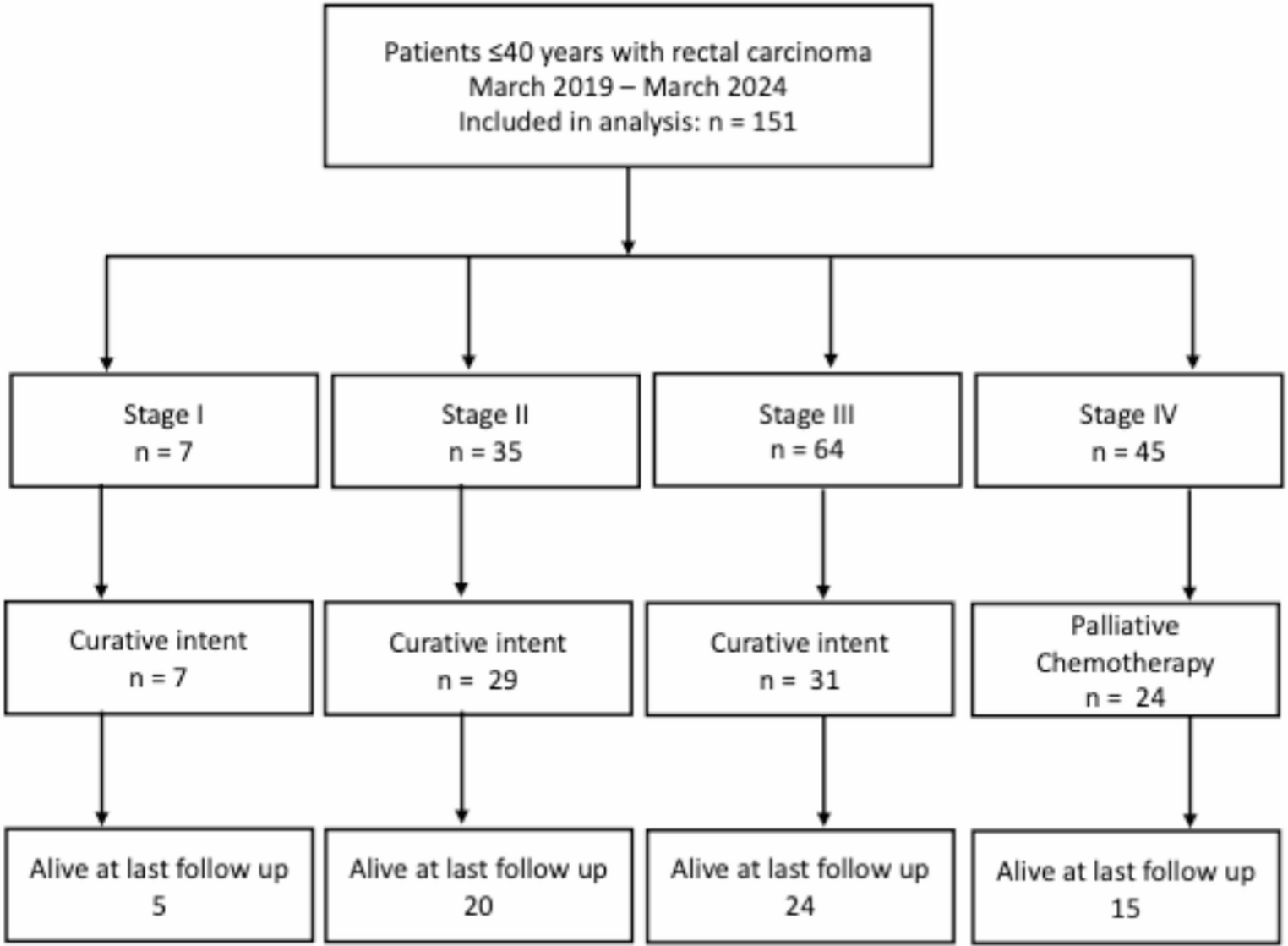
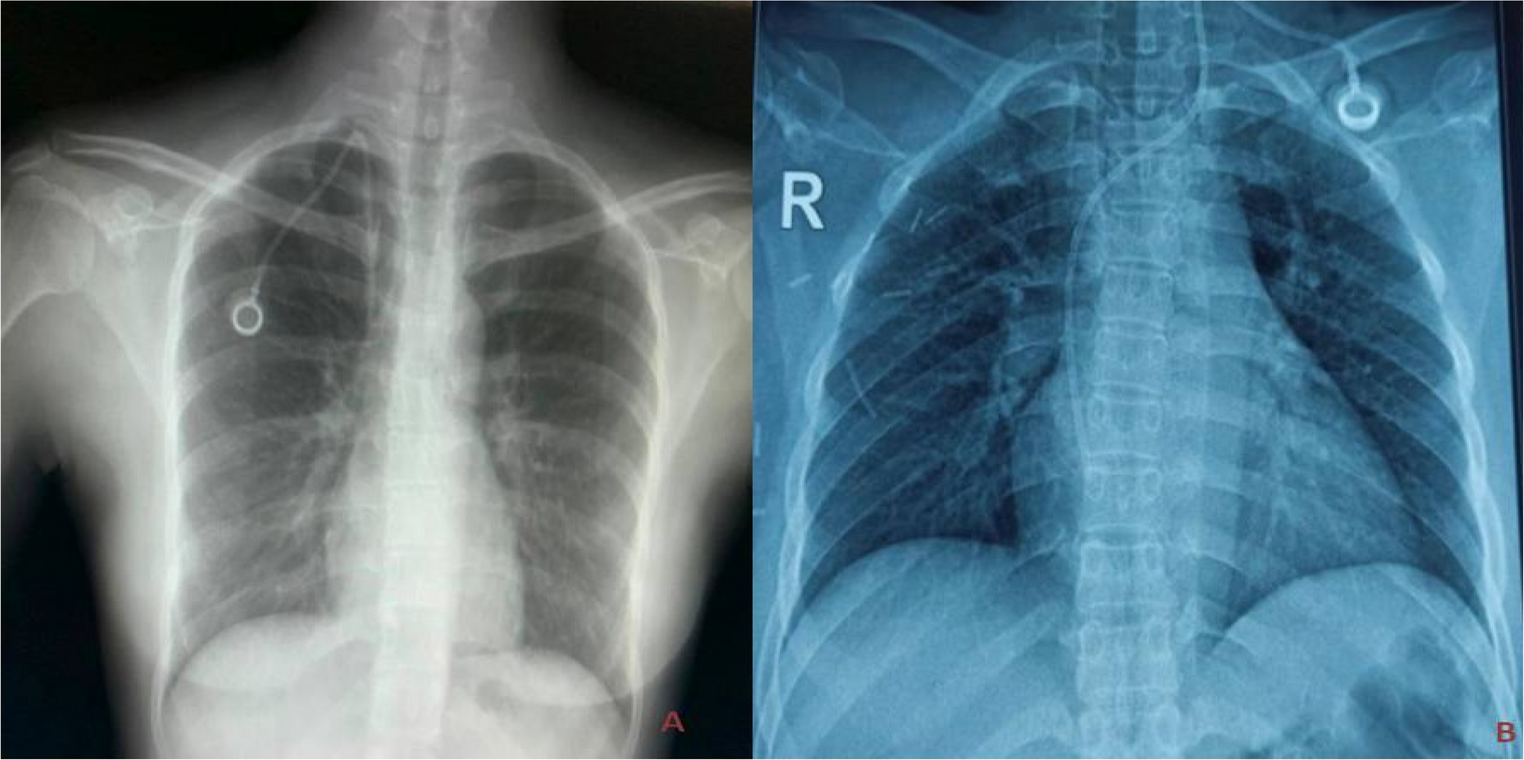
Part 1 (Cohort 1)To achieve the first SMART goal (to achieve baseline data), all patients aged > 18 years undergoing surgery for oral cancer with nasotracheal intubation from October 1, 2023, to May 15, 2024, were included. Patients undergoing surgery with oral intubation/tracheostomy for oral cancer or other head and neck cancer were excluded. The relevant demographic and clinical details such as age, gender, comorbidities, ECOG status, and history of prior treatment (including head and neck irradiation), family history, clinical T-stage, N-stage, details of the surgery, duration of surgery, need for overnight intubation, duration of intubation, and location of postoperative ward were collected from the electronic medical records. The patient was assessed on the first postoperative day by the surgeon (Consultant & Resident) for the presence or absence of NAPS. Any sore or ulcer on the nasal ala was documented as the presence of NAPS (Fig. 1B). Baseline demographics And relevant clinical information are documented for periodic clinical audit. Patients with NAPS were treated with topical Antibiotic ointment for local application for 7 to 10 days.
Statistical AnalysisStatistical Analysis was done using SPSS version 29 (IBM Corp, Armonk, New York). The univariate analysis was done to test the association for variables based on clinical relevance using the chi-square test and/or Fisher’s exact test. The multivariate analysis was done using binomial logistic regression (forward stepwise selection). A p-value of < 0.05 was considered significant.
Part 2 (Cohort 2)Information regarding the incidence and predisposing factors was shared with all stakeholders. Several meetings were held with various disciplines involved in the clinical care pathway to generate and review the process map and fishbone diagram. A process map (Fig. 2A) was made to understand the sequence of events starting with patients entering the operating room and until shifted to the postoperative recovery bay. Next, a fishbone analysis was done to identify potential contributory factors for the development of NAPS (Fig. 2B). As a team, the stakeholders were asked to prioritise the most frequent causes for NAPS; this was used to generate a Pareto chart (Fig. 3A). Interventions were designed to address these areas that were easiest to implement and provided maximum benefit to patients and the care provider team (Action-Priority-Matrix).
Fig. 2
(A) Process map, (B) Fish Bone Analysis
Fig. 3
(A) Pareto chart, (B) Key drivers and interventions
Plan-Do-Study-Act Cycle (PDSAC): It was perceived that there was a lack of understanding/awareness of the entity NAPS as a complication following nasotracheal intubation for oral cancer surgery. Also, there were no preventive measures/methods to monitor NAPS. Hence, a set of interventions was conceived and implemented (Fig. 3B). These interventions were implemented in January 2024. The incidence of NAPS was monitored fortnightly during the implementation process of various interventions (Fig. 4, red arrows) and subsequently thereafter as well.
Fig. 4
Run Chart showing the incidence of NAPS across the study point along with the time point where interventions were implemented (Arrows) and the subsequent reduction in its incidence
Comments (0)