
Remember me

We identified 179 patients with SFT registered at our center for the said duration, of which 111 patients (62%) were extra-thoracic SFTs. Out of this 22 patients (19.8%) who had underwent surgical resection formed the cohort of patients for the study. The median age at presentation was 54 years (range 25 to 75 years). There were 14 male (63.6%) and 8 female (36.4%) patients which included 15 patients with abdominopelvic SFTs, 5 patients with extremity SFTs, and 2 patients with extra-meningeal head and neck SFTs. Patients were initially evaluated with a contrast-enhanced computed tomography (CECT) scan. SFTs are characterized as well-circumscribed soft tissue masses that enhance avidly indicating their vascular nature with smaller lesions being more homogenously enhancing and larger lesions having a central low attenuation area due to necrotic changes (Fig. 1). In extremities, pelvic and orbital SFTs, magnetic resonance imaging (MRI) was done and all cases had demonstrated the characteristic black-and-white-mixed pattern in T2-weighted sequences (Fig. 1). Radiological features although not diagnostic often helped to point towards the diagnosis (11). Preoperative biopsy was done in 16 patients. Surgical morbidity with the Clavien-Dindo Grade 3 or more complications were encountered in 2 patients (9.1%) with both these patients requiring re-exploration due to bowel related complications. Microscopically margin negative resection was achieved in 18 of patients (81.8%) and node positive disease was reported in 1 patient. The median size of tumor in the largest dimension was 12 cm (range: 3 to 30 cm). All cases were diagnosed by their characteristic appearance and CD34 and/or STAT6 expression (5). Immunohistochemical (IHC) markers for STAT6 were positive in all 8 out of 8 patients that were tested. IHC for CD34 was positive in 19 out of 22 in which it was done; BCL2 was positive in 7 out of 9 patients and S100 in 3 out of 17 patients in which they were done. NAB2-STAT6 fusion testing though gold standard was not performed in any patients due to logistic constraints (Fig. 2).
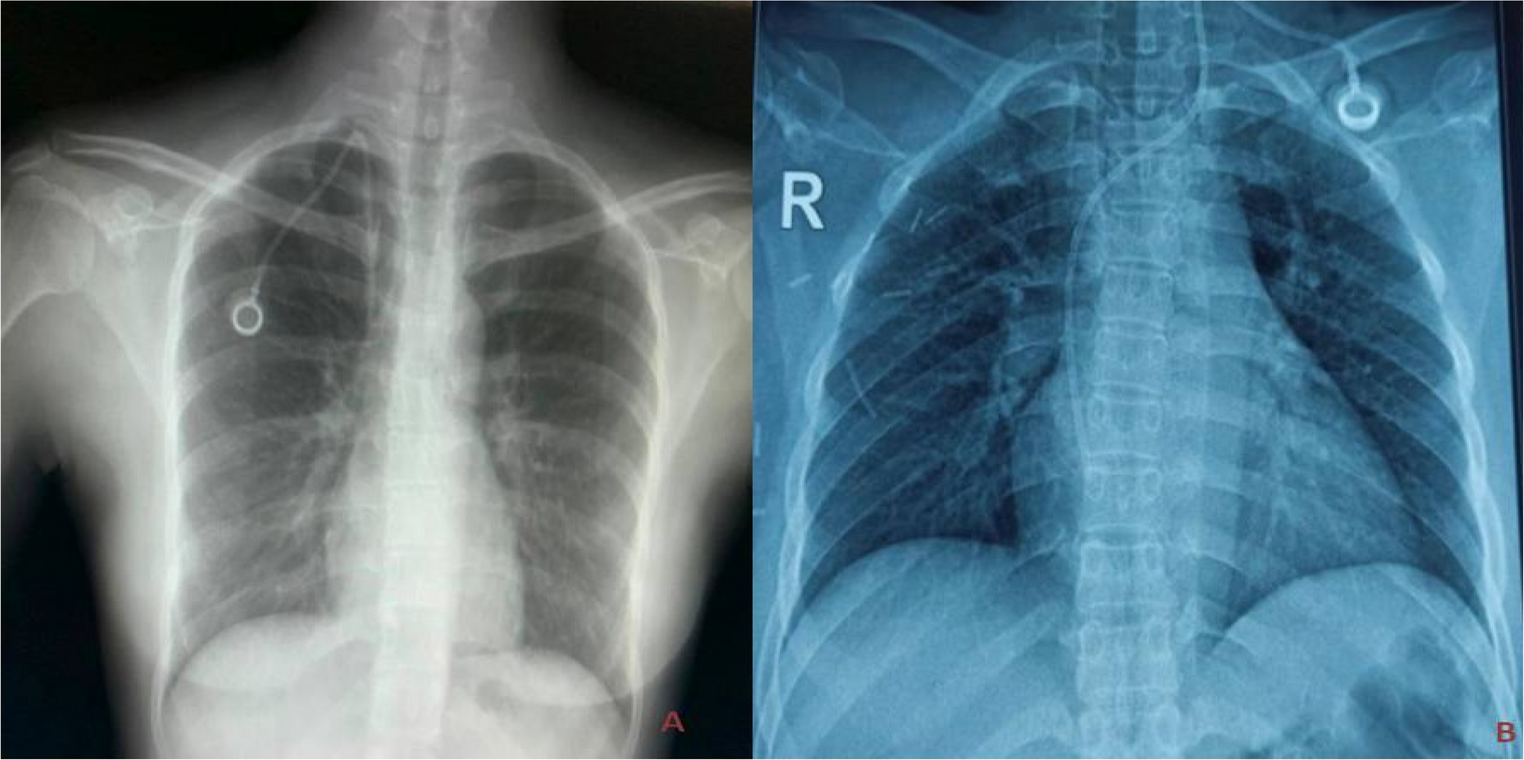
Fig. 1
A, B Axial view of contrast enhanced CT scan of abdomen of right retroperitoneal SFTs. Both cases required right nephrectomy. C Axial view of contrast enhanced CT scan of abdomen of left sided SFT. This case required a Distal pancreatico-splenectomy. D Axial view of contrast CT scan of abdomen scan of mesenteric SFT. The superior mesenteric vessels are posterior and pancreas superior to the mass. E T2-weighed sagittal MRI images of a male patient with pelvic SFT. This case required Abdominoperineal resection as the tumor though well delineated was involving pelvic diaphragm. F T2-weighed sagittal MRI image of a female patient with pelvic SFT. This case was managed without multiorgan resection
Fig. 2
A Cellular tumor composed of spindle-shaped cells with intervening stromal collagen. Hematoxylin and Eosin slides, × 200. B Higher magnification showing relatively monomorphic oval to spindle-shaped cells with intervening thick collagen. C Tumor cells showing diffuse CD34 positivity, including intervening blood vessels. D Same case showing diffuse intranuclear STAT6 positivity
Abdomino-pelvic SFT(Fig. 1)This included 15 patients of which 8 were pelvic site primaries, 5 were retroperitoneal, 1 was mesenteric, and 1 was primary from the liver. Further, the pelvic site SFT also included 1 case of urinary bladder SFT and 1 prostatic SFT. The median age was 55 years ranging from 25 to 75 years, and 11 out of 15 cases were males. All patients were symptomatic on presentation with the most common symptom being abdominal pain. SFTs are known to be associated with paraneoplastic events including reactive hypoglycemia. In our cohort, only one patient had the same in the form of hypoglycemic episodes at initial presentation which resolved after resection (12). The median tumor size was 15 cm (range 4 to 33 cm). Intraoperatively, these tumors were usually found to have well-defined margins, with adjacent organs being pushed rather than invaded. Despite being circumscribed, multivisceral resections were required in 4 patients. Two patients with epicenter in the right retroperitoneum required nephrectomy due to involvement of the renal vasculature. Similarly, one patient required a distal-pancreatic-splenectomy from the invasion of the splenic hilum and tail of the pancreas (Fig. 1C). Another patient required an abdominoperineal resection as the disease involved pelvic diaphragm and anal canal (Fig. 1E). Rarer sites of abdominal primary which included the liver, prostate, and urinary bladder required appropriate organ-specific resections. A patient with prostate SFT who underwent radical prostatectomy had microscopic positive margin and thus was given adjuvant External Beam Radiotherapy (EBRT) to prostate bed and pelvis. Similarly, another patient with pelvic floor SFT who had margin positive tumor excision received postoperative EBRT. Neither of these two patients who had received postoperative radiotherapy for positive margins developed local or systemic relapses. There were no local recurrences and three patients had systemic relapse with a median Disease-Free Interval (DFI) of 54 months.
Extremity SFTThere were five patients with a median age of presentation of 43 years (range 28 to 65 years) with a median size of 12 cm (range 8 to 18 cm) and of these four cases had epicenter in proximal thigh. Preoperative biopsy was done in all patients, and none of the patients received any neoadjuvant treatment. All underwent curative intent margin negative resections. One patient with planned close margins along bone required adjuvant radiation. There were no local recurrences, and one patient had systemic relapse in lung after a DFI of 27 months.
Other Rarer Sites of SFTFor rare sites like orbit and neck, the focus remained on gross tumor excision and was achieved with acceptable morbidity. In the one patient with right sided orbital SFT, gross tumor resection was achievable but the same was removed piecemeal due to difficult access. In this patient, preservation of eye-ball was feasible without need for orbital reconstruction, as the orbital framework was left intact. EBRT was given to prevent local recurrence due to possible intraoperative tumor seeding. The second patient with upper paravertebral mass received postoperative radiotherapy due to planned close margins and ultimately microscopic positive margins at lamina. Neither of these two patients reported any local and systemic at a median DFI of 122 months.
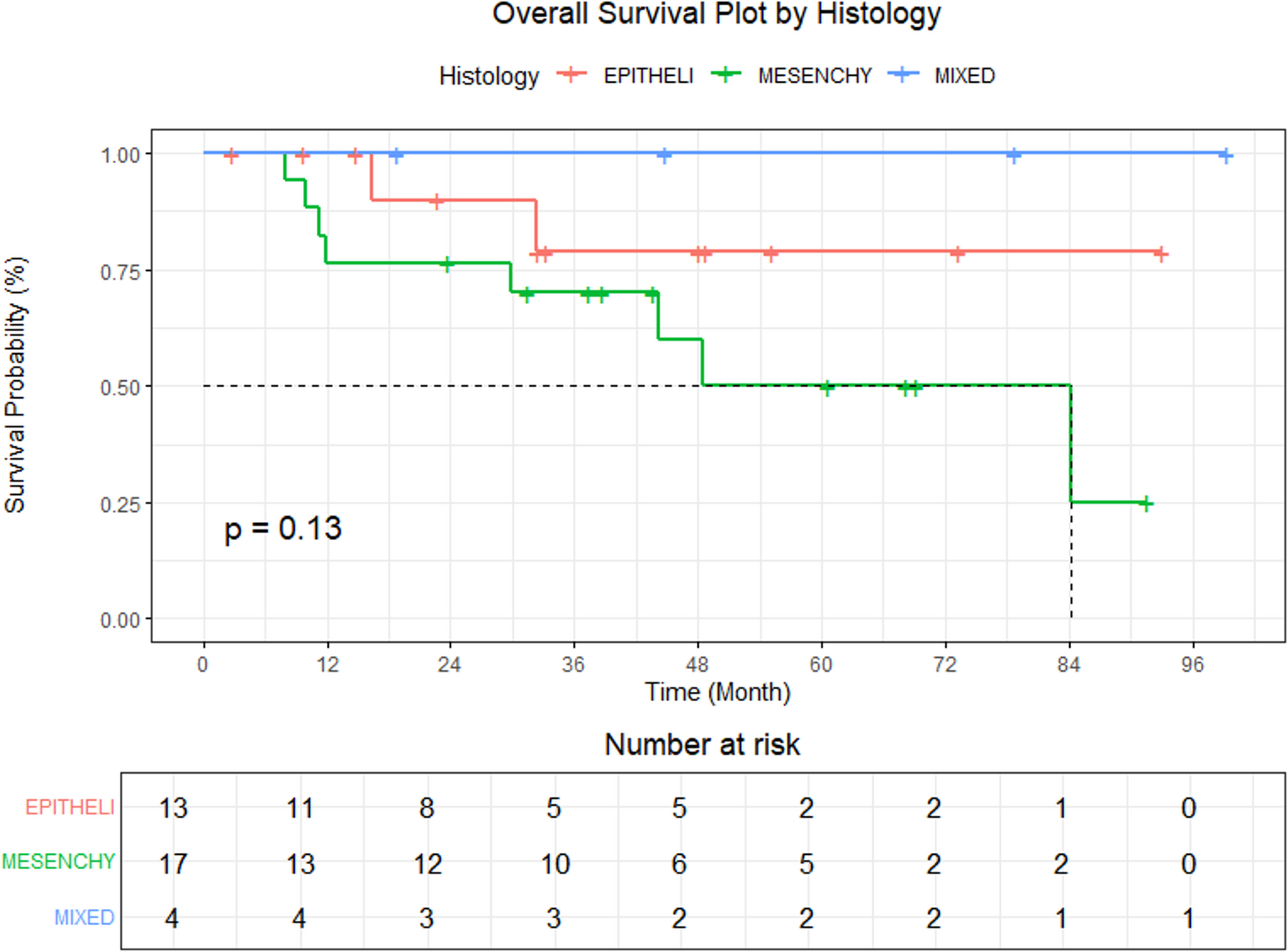
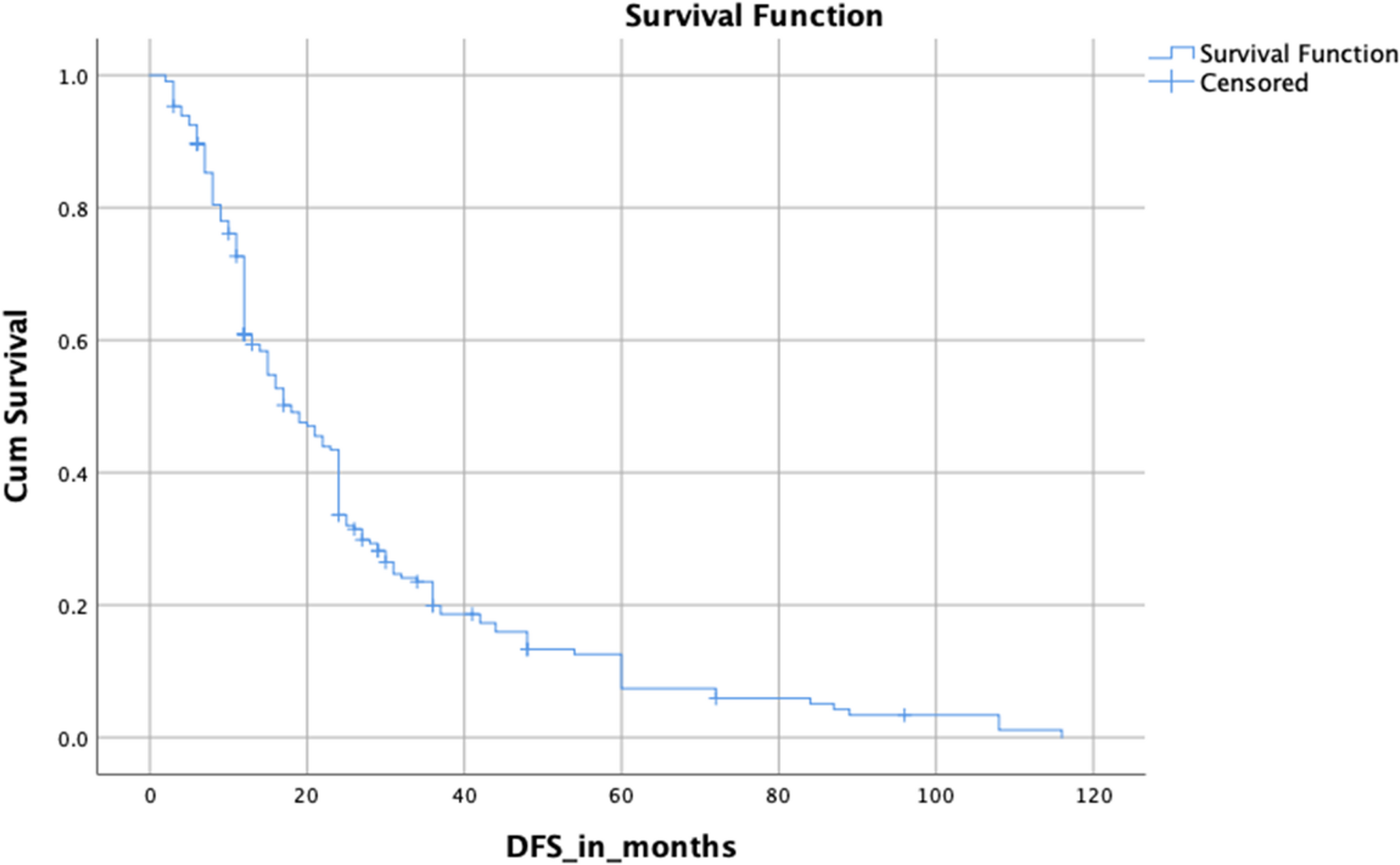
Survival Trends and Recurrence Patterns (Fig. 3, Table 2)Fig. 3
Kaplan–Meir survival curves of DFS and OS for the entire cohort and Demicco model risk groups
The median follow-up duration was 54 months (4 to 162 months). Four patients developed recurrences with three of them occurring after 50 months. Salvage treatment was attempted in all patients at the time of recurrence as they had good performance status, DFI more than 24 months and were single site recurrences. Salvage with systemic chemotherapy was attempted for three patients with lung metastasis with ifosfamide-adriamycin used as first line. Salvage radiation was offered to one patient with bone relapse. Median survival after recurrence was 10.5 months, and all patients who recurred died due to disease progression. The median DFS and OS were not reached for the cohort. The five-year DFS and OS were 80% and 80%, respectively.
Table 2 Factors determining disease-free survival and overall survival*Recurrences happened after 5 years; hence, 5-year DFS was 100%
Out of 22 patients, 11 were low risk, 7 were intermediate risk, and 4 were high risk as per the Demicco model. The 5-year DFS and OS in the low-risk group were 100% and 100%, respectively; intermediate risk group 80% and 85%, respectively; and high-risk group 67% and 60% respectively (Fig. 3). Two patients each in intermediate risk and high risk Demicco groups developed recurrences. None of the low-risk Demicco patients developed recurrences.
Comments (0)