
Remember me



The ideal antiseptic solution for skin disinfection prior to catheter insertion is considered to have various properties including activity against a broad range of Gram- positive and Gram- negative bacteria, and fungi; fast acting efficacy with a residual effect; not inactivated by organic material such as blood or dirt; and non-irritant and non-toxic [56].
Most studies, reviews and meta-analyses available concern the two main active agents, CHG and PVI, either in aqueous or alcoholic formulations. A recent meta-analysis including 10 RCTs reported a 50% reduction in catheter-related BSI when the antiseptic solution used contained CHG rather than PVI [57]. When only alcoholic formulations of both compounds were considered, CHG use was associated with a five-fold reduction in catheter-related BSIs [21, 46]. The most notable study is probably CLEAN 1, a study involving 5,159 CVCs or ACs inserted in 2,349 patients across 11 ICUs. Compared with 5% PVI-69% EtOH, patients assigned to 2% CHG-70% IPA had lower rates of both major catheter-related infections (0.28 vs. 1.77 per 1,000 catheter-days, hazard ratio [HR] 0.15, 95% CI 0.05–0.41; p = 0.0002) and catheter-related BSI (0.28 vs. 1.32 per 1,000 catheter-days, HR 0.21, 95% CI 0.07–0.59; p = 0.003) [21]. Overall, tolerance of the two antiseptic solutions was excellent. Severe skin reactions were more frequent (3% vs. 1%) with the CHG-IPA solution but required treatment discontinuation in only two patients. Treatment discontinuation allowed full recovery without further treatment, and no systemic adverse reactions to either antiseptic occurred. The large observed reduction in infectious complications far outweighed the few and easily managed side effects.
The superiority of 2% CHG-IPA over 5% PVI-EtOH was also reported with PIVCs. In the CLEAN 3 study involving 989 patients and catheters from one French ED, local infections (0 vs. 6 patients) and catheter colonisation incidence (1% vs. 17%) were lower in patients assigned to CHG [20]. No catheter-related BSI was reported in either study group and no severe skin reaction was reported. Minor skin reactions (9 of 499 of CHG patients [2%] and 7 of 496 PVI patients [1%]) were uncommon and similar in both antiseptic groups.
Based on strong evidence from multiple RCTs, national and international guidelines primarily recommend the use of 2% CHG-70% IPA as first-line antiseptic for disinfecting the skin before inserting a vascular catheter [25, 26, 47, 48].
CHG BathingCHG bathing has been extensively studied as a preventive strategy against HAIs, particularly in critically ill patients. Guidelines strongly recommend daily CHG bathing for ICU patients, especially those with CVCs, as part of bundled care measures aimed at reducing catheter-related BSIs [58, 59]. A recent meta-analysis involving 20,188 ICU patients found that daily bathing with 2% CHG-impregnated wipes reduced the relative risk of CVC-associated BSI by 48% compared with conventional soap-and-water bathing (RR 0.52, 95% CI [0.37–0.73]) [2]. Subsequent to this meta-analysis, post hoc analyses from trials such as CLIP-ID and ABATE provide additional nuance. These analyses reveal a significant reduction in CVC-associated BSIs involving Gram-positive bacteria, particularly coagulase-negative staphylococci (CoNS), but no meaningful impact on infections caused by Gram-negative bacteria [60,61,62]. This limitation may stem from the aqueous formulation of CHG used in the trials, which is less effective against Gram-negative bacteria than alcoholic formulations.
Fig. 1
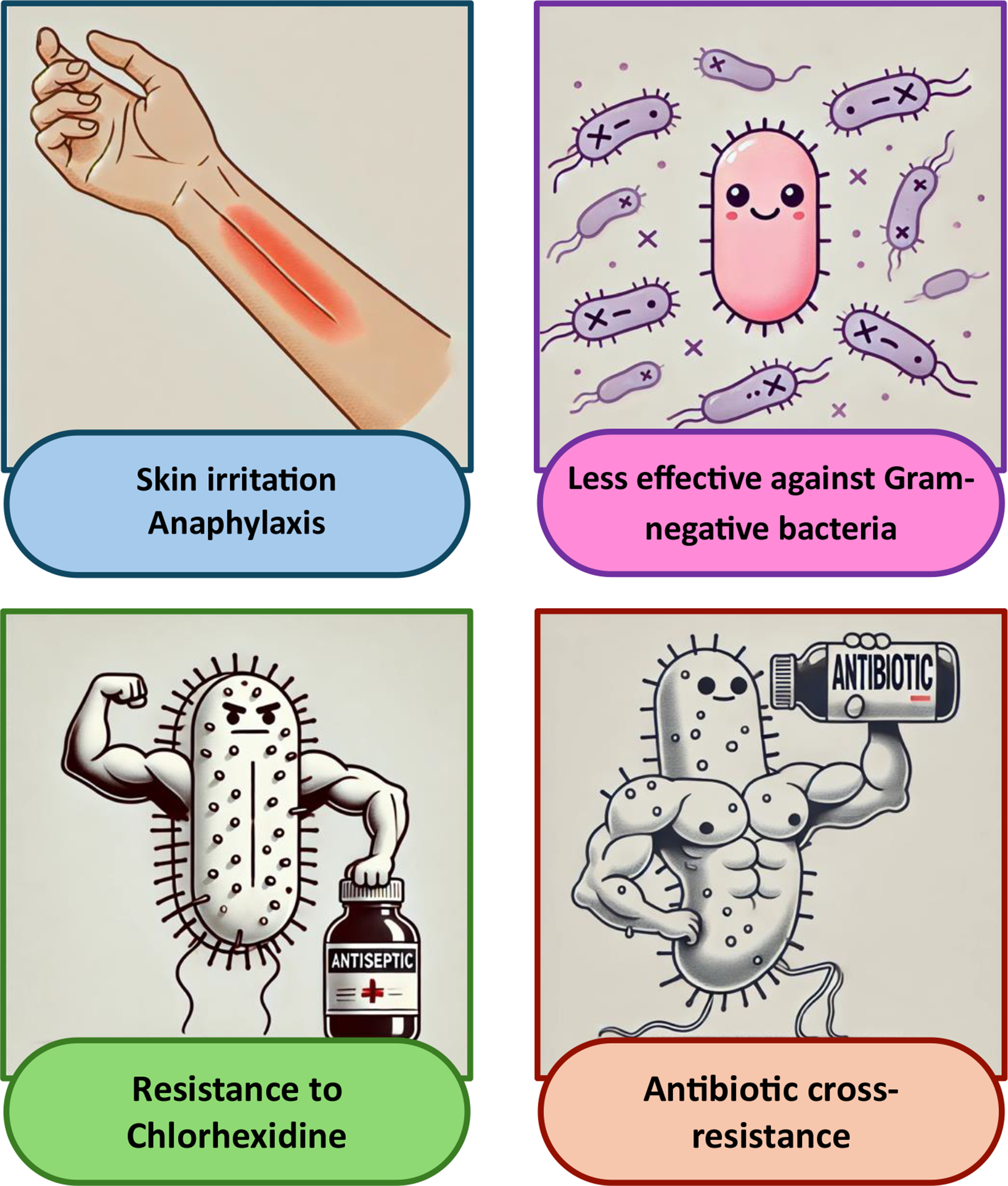
Main concerns linked to the overuse of chlorhexidine
While CHG bathing is generally well-tolerated, concerns about skin reactions, particularly with higher CHG concentrations, have been raised [2]. Reports of mild to moderate reactions, such as dermatitis, exist, but these are typically outweighed by the substantial benefits in infection prevention [63]. Recent advancements in CHG wipe formulations, including improved adhesive properties and enhanced skin moisture evaporation, have further minimised skin irritation [2].
Despite its limitations, CHG bathing remains a valuable intervention for reducing catheter-related infections when integrated into care bundles, including rigorous hand hygiene and maximal barrier precautions during catheter insertion. However, its routine implementation in ICUs faces challenges, including costs, staff training, and patient acceptance. CHG use should be reserved for cases where the benefits clearly outweigh potential risks, such as toxicity and bacterial resistance [64]. Continued research is essential to strengthen the evidence base and explore broader applications, including for patients with CVCs in other high risk clinical settings such as kidney and cancer units, as well as for ICU patients without CVCs.
CHG-impregnated DressingsCHG-impregnated dressings have emerged as a critical intervention for preventing infections associated with CVCs and AC, particularly in ICU patients, and their use is strongly recommended by international guidelines [25, 48, 65, 66]. By contrast, there is no robust evidence supporting their efficacy for PIVCs, emphasising the need for larger-scale studies in this setting.
Three types of CHG-impregnated dressing are available: CHG-impregnated sponges, CHG gel dressings and more recently as CHG impregnated polyurethane dressings. To our knowledge, a direct comparison between sponges and gel dressings has never been performed. The efficacy of CHG dressings is well-documented through multiple high-quality studies. A meta-analysis including 14 randomised controlled trials and 8,920 patients demonstrated that CHG-impregnated dressings halved the risk of catheter colonisation and catheter-related BSI compared with standard dressings [67]. Real-life studies further corroborate these findings. Over an 11-year period, implementation of CHG dressings within a comprehensive catheter care bundle in Swiss hospitals resulted in progressive and sustained reduction in catheter-related BSIs. This decrease was observed similarly with both sponges and gel dressings [68]. However, gel dressings showed fewer dressing disruption, a major risk factor of catheter-related infections [16, 69]. Moreover, sponges do not allow continuous inspection of the catheter insertion site and are more difficult to apply and remove without additional training.
Earlier studies reported more contact dermatitis with the CHG dressing. However, improvements with newer dressings, enhanced adhesive distribution and improved skin moisture evaporation, have since addressed these concerns. A recent analysis reported similar low rates of contact dermatitis for CHG dressings and standard dressings (0.3 episodes per 1,000 device-days in both groups) [68, 70].
Studies evaluating CHG dressings on PIVCs are scarce. A randomised pilot study compared the efficacy of CHG dressings specially designed for the maintenance of PIVC with standard dressings in 300 patients. Colonisation (0.7% versus 2.7%) and local infection (0% versus 0.7%) incidence was lower in patients assigned to the CHG dressing, but the study lacked power to test for statistically significant differences. Skin tolerance to both dressings was similar.
Connector and Hub DisinfectionHub and connector disinfection prior to catheter use is a critical step in preventing catheter-associated BSIs. International guidelines recommend performing active disinfection through a vigorous mechanical scrub using a flat swab pad containing 70% IPA, CHG-IPA suitable for use with medical devices or alcohol caps [48, 59].
Fig. 2
Prioritising preventive measures with chlorhexidine
CHG-IPA is more effective than 70% IPA alone in reducing bacterial load on needleless connectors, leading to reduction in catheter-associated BSIs relative risk by as much as 72% compared with alcohol alone and in a pilot RCT (N = 180) was associated with zero BSIs in cancer patients compared to 2% in patients using alcohol alone in either a flat wipe or an alcohol cap [71,72,73]. By contrast, PVI is less frequently recommended due to its tendency to leave a sticky residue as it dries, complicating the use of needleless connectors [71, 74].
Other cluster-randomised trials evaluated the effectiveness of antimicrobial barrier caps impregnated with CHG in preventing catheter-associated BSIs in haemodialysis patients. These caps significantly reduced catheter-associated BSIs rates compared with standard needleless connectors combined with alcohol-based disinfecting caps [75, 76]. Notably, CHG caps were equally or even more effective against infections caused by gram-negative bacteria than by gram-positive bacteria. No device-related adverse events were reported [75]. However, to our knowledge, the limited number of studies exploring this specific question restricts the robustness of the recommendations and both previous trials were done in conjunction with the manufacturer of the CHG caps.
Although these preliminary data are promising, the number and quality of studies are insufficient to make strong recommendations. Further studies are needed to determine whether CHG impregnation is more effective than alcohol impregnation.
CHG-impregnated CathetersCVCs impregnated with chlorhexidine/silver sulfadiazine are designed to prevent bacterial colonisation and biofilm formation, two key mechanisms in the occurrence for catheter-related infections. The first generation were impregnated externally only. The second generation is impregnated both externally and internally to increase efficacy. The Society for Healthcare Epidemiology of America (SHEA) recommends antiseptic or antimicrobial impregnation of CVCs for reducing the risk of catheter-related BSI, with high-quality evidence in adults and moderate-quality evidence in paediatric patients.
Data from two meta-analyses highlight the efficacy of chlorhexidine/silver sulfadiazine-impregnated catheters in patients. Both reported a 50% reduction in colonisation and catheter-related BSI compared with standard CVCs [77, 78]. Surprisingly, key outcomes such as all-cause mortality were not impacted by the type of CVC used. A recent study, conducted under laboratory conditions simulating clinical scenarios, reported a reduction in Candida auris adherence, particularly with second-generation catheters, suggesting that impregnated catheters may also have a beneficial impact on fungal infections [79]. In contrast, the recent publication of the PICNIC trial, a multicentre, randomised, controlled superiority trial comparing hydrophobic, chlorhexidine-coated, and standard polyurethane PICCs in 1098 adults and children across three Australian hospitals, showed no significant reduction in device failure rates for hydrophobic or chlorhexidine-coated PICCs compared to standard polyurethane PICCs, with complications being highest in the chlorhexidine group [80].
While these results highlight the potential benefits of impregnated catheters, it is important to note that most of the studies were carried out before the widespread adoption of CVC insertion bundles, and in patients with high susceptibility to HAIs. This may therefore have overestimated the impact of these catheters in more contemporary settings. There is no data on the performance of these catheters as part of a comprehensive infection prevention strategy that includes current evidence-based hygiene recommendations.
Thus, the use of CVCs impregnated with chlorhexidine/silver sulfadiazine should be reserved in settings where catheter-related BSI rates exceed institutional targets despite adequate implementation of all recommended prevention measures, in patients with limited venous access and a history of recurrent catheter-related BSIs, and in patients at high risk of severe complications, such as those with recently implanted intravascular devices [59, 81, 82]. Further research is warranted to validate these indications.
Myths and Realities“CHG Is Responsible for a Large Number of Allergy Cases and Should Be Used with Caution!”In 1998, the FDA warned healthcare professionals about the potential for anaphylaxis linked to CHG-containing products, such as impregnated CVCs and dressings. Between 1969 and June 2015, the FDA received 43 reports of CHG-related anaphylaxis worldwide, with over half reported after the 1998 notice. Additional data include eight cases documented in medical literature from 1971 to 2015 and one case identified through the NEISS-CADES database between 2004 and 2013. Among the reported cases, serious allergic reactions often required emergency treatment or hospitalisation, with two fatalities attributed to anaphylaxis. These numbers, however, likely underestimate the true incidence due to underreporting [83].
Beyond systemic reactions, CHG has also been associated with a range of skin reactions, from mild contact dermatitis and erythema to rare but severe hypersensitivity reactions requiring careful monitoring [13]. For instance, a case series involving six patients with complex skin disorders (e.g., Stevens-Johnson syndrome, toxic epidermal necrolysis syndrome, burns, anasarca and graft-versus-host disease) revealed necrotic lesions linked to CHG disks. This highlights the risks for patients with compromised skin barriers, exudative wounds, or prolonged exposure to CHG products [84].
While valid, concerns about CHG-induced allergic reactions must be contextualised within its widespread use and critical role in preventing HAIs. Reports of CHG allergies include immediate hypersensitivity reactions, such as anaphylaxis, and delayed-type reactions, such as contact dermatitis [85, 86]. However, robust evidence indicates that such reactions are exceedingly rare, especially when compared to the millions of patients exposed to CHG annually in healthcare settings. Further, it is thought that many cases of local ‘reaction’ to CHG actually reflect irritation from the dressing being applied to wet skin and therefore clinical education about allowing the skin to dry prior to dressing placement is important.
Large-scale studies consistently demonstrate the low prevalence of CHG-related allergic reactions. For example, a Danish dermatology clinic reported only 1% among 8,497 patients patch-tested positive for CHG allergy, with most cases presenting as mild contact dermatitis [87]. Similarly, a systematic review analysing 14 worldwide reports of CHG-induced anaphylaxis found that the estimated incidence in perioperative settings was less than 1 per 100,000 exposures. Importantly, the majority of severe reactions were linked to high-risk applications, such as mucosal application or impregnated line intravascular use, where CHG is directly introduced into sensitive tissues [86].
The safety of CHG is further supported by its long history of use and significant improvements in formulation. Modern CHG products, such as 2% CHG-alcohol for skin antisepsis, are designed to minimise irritation while maintaining efficacy. In the CLEAN study, involving 2,349 patients, no systemic allergic reactions to CHG-alcohol were reported, while the intervention reduced catheter-related BSIs relative risk by 77% compared to PVI-alcohol [21]. By contrast, minor skin reactions were observed, without any impact on patient outcome. Similarly, a meta-analysis involving 34,408 blood cultures where different antiseptic solutions were used for skin disinfection reported no case of severe allergic reactions [88]. Though rare, immunological investigation of serious suspected cases and reporting of identified cases to the health authorities should be the rule.
“CHG Is Less Effective against Gram-negative Bacteria!”The perception that CHG is less effective against Gram-negative bacteria is based on theoretical data and experimental observations. However, clinical evidence presents a more nuanced picture.
Large-scale trials and meta-analyses have shown that CHG is equally effective in reducing HAIs caused by both Gram-positive and Gram-negative bacteria. This is the case with studies comparing CHG-impregnated dressings with standard dressings [67], as well as trials evaluating CHG versus PVI for skin antisepsis before catheter insertion [20, 21, 45].
Regarding CHG bathing, several studies reported its ability in reducing colonisation and infection by multidrug-resistant organisms (MDROs), including Gram-negative pathogens such as Acinetobacter baumannii [89]. A large meta-analysis in ICU settings evaluating CHG bathing reported similar reduction in BSIs caused by both Gram-positive and Gram-negative pathogens compared with standard soap-and-water bathing [2]. However, other recent ICU study showed no significant impact on CVC-associated BSI caused by gram-negative bacteria, although these findings may be limited by sample [61]. Overall, CHG’s efficacy against Gram-negative bacteria appears to be context-dependent. While in vitro studies and ICU-based trials have demonstrated activity against some Gram-negative species, results from non-ICU settings are more variable. For example, the ABATE trial, which assessed daily CHG bathing in non-ICU patients, reported no statistically significant reduction in BSIs due to multidrug-resistant Gram-negative organisms (HR 0.91, 95% CI 0.82–1.00; p = 0.16). This limited effect may reflect lower skin colonisation densities, the protective nature of biofilms, or reduced antiseptic penetration in the presence of organic matter. These findings suggest that CHG bathing efficacy is influenced by both the type of pathogen and the clinical context in which it is applied.
In summary, although some variability exists—particularly in lower-risk settings—CHG retains broad-spectrum clinical efficacy, and theoretical concerns regarding reduced activity against Gram-negative bacteria are not consistently supported by clinical outcome data.
“CHG Use Induces Bacterial Resistance to Antiseptics!”CHG has been the focus of resistance concerns due to its extensive use and potential implications for patient health. While antiseptic resistance is generally defined as a change in susceptibility that renders it ineffective against a previously susceptible microorganism, this definition which mirrors that of antibiotic resistance, is not entirely correct, for several reasons [35]. Indeed, antibiotic resistance is typically determined using minimal inhibitory concentration (MIC) values, a straightforward approach due to the standardised serum and tissue concentrations achieved through oral or parenteral administration. In contrast, antiseptics are applied topically, usually at concentrations far exceeding bacterial MIC values [90]. Moreover, CHG efficacy is influenced by various environmental factors, such as pH, temperature, presence of organic matter, biofilm formation and contact time. Finally, CHG is often combined with alcohol, another antiseptic with quick and intense bactericidal activity, providing a dual mechanism of action that enhances the efficacy of disinfection and helps protect against selection of resistant strains. As a result, this phenotypic method often yield misleading conclusions when applied to antiseptics [6]. The lack of standardised laboratory protocols to determine MIC values complicates the comparison across studies, highlighting a critical gap in antiseptic resistance research. Studies conducted at the laboratory to select strains with reduced susceptibility to CHG were not conclusive. For example, successive exposure of a Pseudomonas aeruginosa strain to subinhibitory concentrations of CHG increases its MIC from 1.56 to 25,000 ug/mL [90]. These values remain below the concentrations of CHG used in clinical practice, which generally range from 0.25 to 4% (2,500 to 40,000 µg/mL) [32]. In addition, these experiments do not take into account the contribution of alcohol.
Bacterial adaptive resistance may arise through different mechanisms [34]. Efflux pumps, such as QacA/B or QacC in Staphylococcus aureus, enable bacteria to become less susceptible to CHG by actively expelling CHG molecules, thereby reducing intracellular concentrations. Genes encoding for efflux pumps, carried on mobile genetic elements like plasmids or transposons, facilitate the spread of resistance within and across bacterial populations. These transfers are facilitated by the proximity of bacteria to each other, for example within a biofilm [6, 34].
A study investigating the prevalence of CHG adaptive resistance genes coding for efflux pumps (qacA/B and smr) on skin of hospitalised patients exposed to CHG-impregnated dressings found 79% of positive specimens. This prevalence was not different from those observed in samples taken from contralateral arms not exposed to CHG. By contrast, non-CHG-treated patients showed lower prevalence of resistant genes. The prevalence of resistant genes increased with CHG dressing exposure, suggesting that patients were contaminated with bacteria or DNA containing resistant genes during their hospital stay. Presence of these genes were not associated with the presence of viable bacteria. The study underscores the widespread presence of adaptive resistant genes in hospital environments and the potential impact of prolonged CHG exposure, highlighting the importance of resistance monitoring [91].
Furthermore, biofilm formation represents a significant resistance mechanism, as it creates a structured bacterial community embedded in a self-produced extracellular matrix. This barrier hinders CHG penetration into deeper layers, preventing the biocide from reaching lethal concentrations. Subinhibitory levels of CHG within biofilms can promote adaptive resistance mechanisms, raising concerns about their impact on infection control efforts in clinical settings [40].
Additionally, CHG can influence the skin microbiota, although studies suggest that its effects are transient. For instance, one pilot study found minor shifts in microbial composition over 72 h following CHG application, with some species (e.g., Finegoldia magna) becoming more abundant but without significant long-term reduction in diversity. Another study comparing CHG-IPA and PVI-EtOH before PIVC insertion noted transient changes in microbiota composition, such as alterations in the Firmicutes/Bacteroidetes ratio, without lasting impact on diversity. These findings highlight the resilience of the skin microbiome while suggesting that transient modulations could influence outcomes such as catheter colonisation or BSIs [92, 93].
While mechanisms of reduced susceptibility to CHG, such as efflux pump expression or biofilm-mediated tolerance, have been demonstrated under laboratory conditions, these findings have not translated into decreased clinical efficacy. Observed increases in MICs remain well below the CHG concentrations typically used in clinical practice, particularly when combined with alcohol, which provides rapid and potent bactericidal action. Moreover, studies have not identified any treatment failure or higher infection rate attributable to CHG resistance. The presence of resistance genes in skin microbiota, though frequent in hospital environments, is not consistently associated with viable bacterial carriage or clinical outcomes. This supports the conclusion that current antiseptic protocols using CHG-alcohol remain highly effective. In addition, CHG exposure induces only minor, transient shifts in the skin microbiome, without significant long-term alteration of microbial diversity, further supporting its safety in routine use.
“CHG Induces cross-resistance with Antibiotics!”The selection of antibiotic-resistant bacteria following the use of antiseptics is a growing concern, as it could limit the efficacy of last-resort antibiotics. One key mechanism involves the over-expression of efflux pumps, which enable bacteria to expel various antibiotics and biocidal agents, including CHG. A study of 114 Staphylococcus aureus isolates found that 96% of the strains expelled chlorhexidine (CHG) via efflux pumps, with 57% also exhibiting efflux of norfloxacin, highlighting the central role of efflux mechanisms in resistance [94, 95]. Another study reported that, after 14 days of prolonged exposure to s
Comments (0)