
Remember me
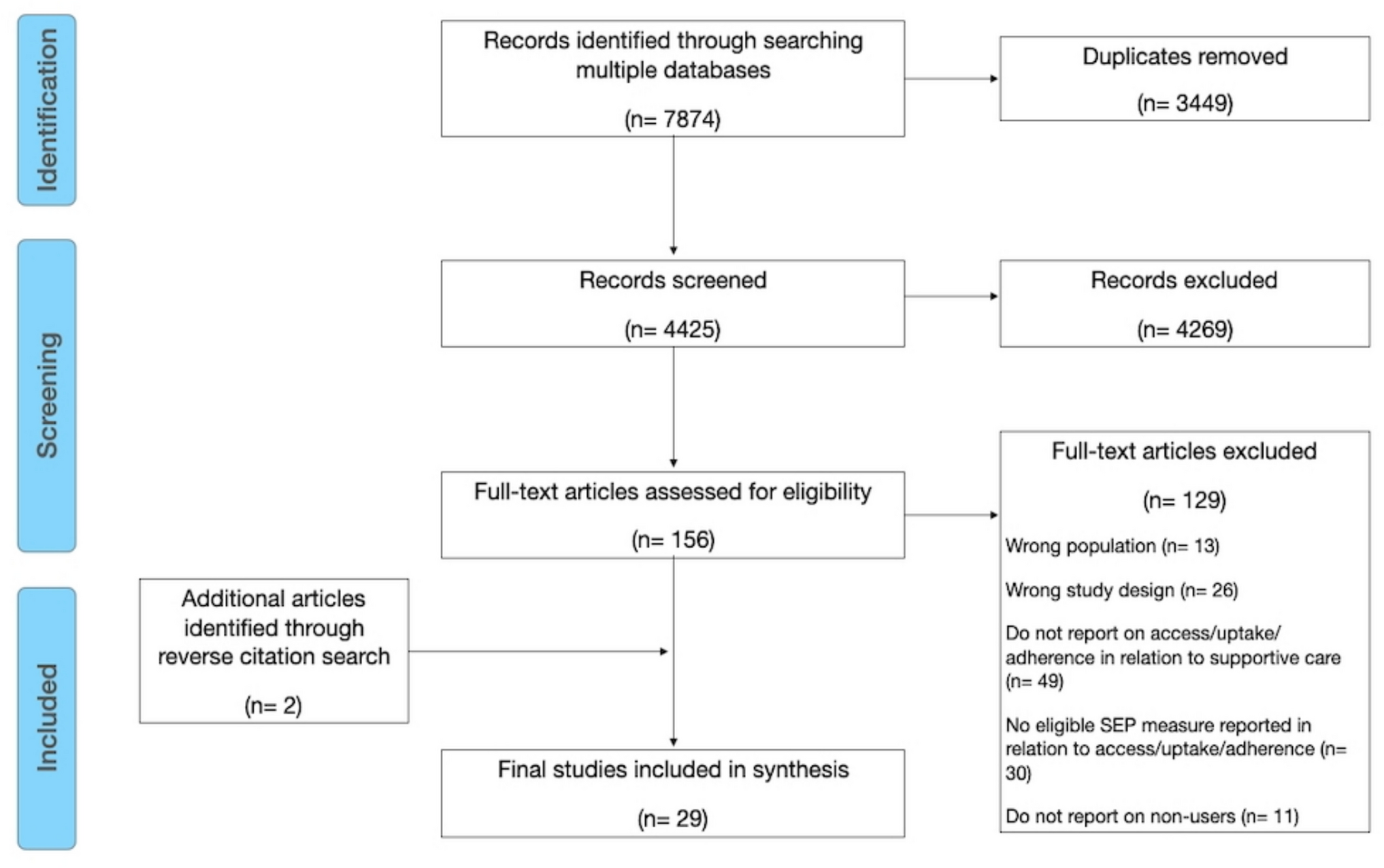

The flow of full reports, protocol papers, and trial registry entries is shown in Fig. 1. The database searches yielded 1795 records. After removing duplicates, 1687 records were screened and 96 were assessed for eligibility. Seventy-one records were excluded, leaving 25 reports for inclusion. After reviewing records known to the authors and completing backwards and forwards citation searching, an additional 3 reports were included. In total, 28 reports were included, including 13 full reports [40,41,42,43,44,45,46,47,48,49,50,51,52], 4 protocol papers [53,54,55,56], and 11 trial registry entries [57,58,59,60,61,62,63,64,65,66,67] (Table 1).
Fig. 1 Table 1 Summary of characteristics in full reports, protocols, and trial registriesFull reportsQuality assessment
Table 1 Summary of characteristics in full reports, protocols, and trial registriesFull reportsQuality assessmentTable 2 summarises the methodological quality of full reports. True randomisation was used in all except two studies, from the same authors, which lacked detail about the randomisation procedure [45, 46]. Those allocating participants to groups were concealed from allocation in eight studies [40, 44, 47,48,49,50,51,52], but it was unclear in the remaining five [41,42,43, 45, 46]. As expected for behavioural interventions, no study blinded participants or intervention deliverers to treatment allocation. Outcome assessors were not blinded to treatment allocation in two studies [50, 51], and this was unclear in another six [41, 43, 45,46,47, 49].
Table 2 Summary of quality assessments using the Joanna Briggs Institute Critical Appraisal Checklist for Randomized Controlled TrialsBaseline differences existed between groups in three studies [41, 44, 45]; including differences in education level [41, 44], marital [41], and employment statuses [45]. The intervention and control groups were treated differently in six studies [40, 43,44,45, 48, 49]. For example, offering the control group support unavailable to the intervention group, such as enhanced usual care [43] or additional communication [48].
Differences between groups regarding follow-up (e.g. descriptions of loss to follow-up (LTF), reasons for LTF, impact of incomplete follow-up) were inadequately described in six studies [43,44,45,46, 48, 49]. All studies had reliable outcomes that were measured identically across groups, used appropriate designs and analysed participants in the groups they were randomised. One study was considered to not have used appropriate statistical analysis [45], which involved a complex crossover design but conducted separate comparisons for the immediate and delayed receipt of the intervention with the control.
Characteristics of studiesMost (61.5%) full reports originated in the USA [40,41,42, 44,45,46,47,48, 52], with representation also from Australia [43, 50], India [49], and various European countries [51]. Three were full reports of phase III trials [42, 49, 51], with the remainder being phase II [42] or pilot/feasibility studies (69.2%) [41, 41, 44,45,46,47,48, 50, 52]. Nearly all used a parallel group RCT design, with a minority using an RCT with full or partial crossover [45, 46, 48]. One trial reportedly used a quasi-experimental design, but it was unclear how the allocation method was not random [41]. Sample sizes ranged from 21 [46] to 357 [51] (median = 49).
Participant characteristics were not consistently reported, with 9/13 reporting on ethnicity [40,41,42,43,44,45,46, 48,
Comments (0)