
Remember me
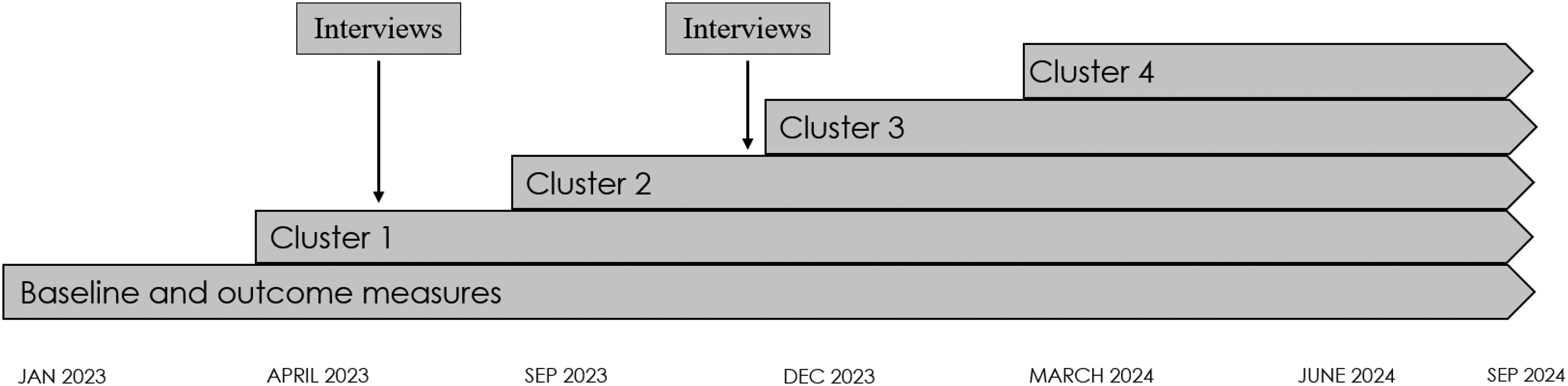






The present study was based on data from individual interviews and group interviews. The interviews were conducted in two rounds during the iTAPP study (Fig. 1), which is a stepped-wedge cluster randomized control trial [26]. In the iTAPP study, four clusters of general practices were enrolled as active practices, i.e. implementing the 15-method, in three-month intervals following a three-month baseline period [15]. The present study adheres to the Standards for Reporting Qualitative Research (SRQR) [27].
Fig. 1
Timeline and interview timepoints for evaluating adaptations and modifications to the 15-metod during implementation in the iTAPP study. Total of 28 healthcare professionals across 12 general practices in The Region of Southern Denmark. Notes: iTAPP, Identification and Treatment of Alcohol Problems in Primary Care (iTAPP) study. Stepped-wedge cluster randomized design. Baseline and outcome measures refer to measures in the iTAPP study. Each cluster includes 4–6 general practices. Interviews (n = 17) consisted of 6 individual and 11 group interviews
SettingThe participating general practices are situated in the Region of Southern Denmark, which comprises 345 practices [28] each with an average of 2.3 general practitioners (GPs). In this region, the typical GP manages 1,541 listed patients, and 99% of the Danish population is registered with a GP [29, 30]. The GP functions as the primary provider and a gatekeeper to the secondary healthcare system and medical treatment and consultations incur no costs for patients [31]. The practices involved in the iTAPP study encompass both urban and rural settings and include solo practitioners as well as larger practices with several GPs, nurses, and other staff groups e.g. medical students and assistants [15, 30].
InterventionThe 15-method is a three-step intervention designed to help HCPs address alcohol-related issues in patients through a structured approach.
Step one (initial screening and brief advice): during routine visits, HCPs conduct opportunistic screening and offer brief advice. HCPs may use screening tools like the Alcohol Use Disorder Identification Test (AUDIT) [32] and biomarkers to screen for alcohol issues if relevant symptoms are present [4, 33]. If alcohol is found to be pertinent to the patient’s condition, the HCPs provide brief advice during this same consultation and suggests scheduling a dedicated follow-up (step two). Between step one and two, patients may complete the AUDIT questionnaire if not already administered to facilitate continuity and ensure comprehensive assessment.
Step two (personalized feedback and check-up): In this second consultation, HCPs provide personalized feedback based on information obtained during step one and between step one and two (e.g., AUDIT results, biomarkers). Tools like the one-week Timeline Follow-Back [34], the Short Alcohol Dependence Data Questionnaire [35], and the International Classification of Diseases 10th revision (ICD-10) criteria for alcohol dependence [36] may be used for further assessment, alongside screening for other substance use if needed, e.g. benzodiazepines and opioids during this step. The HCP then encourage patients to consider the impact of their drinking on health and explore motivation for behavioral change.
Step three (Treatment sessions with planned follow-up): This step comprises up to three treatment sessions, premised on Motivational Interviewing (MI) [37], Cognitive Behavioral Therapy, and Guided Self-Change [38] incorporating strategies like an alcohol diary, goal setting, and self-monitoring exercises. Treatment sessions utilize MI principles, in which Danish GPs receive training during their specialist training. Homework assignments incorporate straightforward CBT-based exercises that require no formal CBT training for HCPs to administer. Collectively, these treatment sessions constitute a guided self-change approach. Treatment intensity and goals are established through shared decision-making [39], with pharmacological treatments options available per national guidelines (Disulfiram, Acamprosate, Nalmefene, or Naltrexone). Step three concludes with collaborative planning between HCP and patient for either a follow-up consultation or referral to specialized treatment, based on the patient’s needs.
HCPs received training in the 15-method and in recognizing and addressing alcohol-related symptoms using an MI approach through academic detailing [40, 41]. Academic detailing, also referred to as educational outreach visits, comprises structured, evidence-based educational interventions delivered through planned visits to healthcare settings to facilitate knowledge translation and clinical practice improvement. Details on the 15-method, its materials, and implementation in the iTAPP study are provided elsewhere [7, 12, 15, 42].
Recruitment and data collectionInterview participants were recruited through their participation in the iTAPP study as part of the 15-method training sessions. HCPs from cluster one and two were included with representation of both GPs and nurses to ensure data from both managers and staff. Interviews were conducted from May to December 2023 in two rounds (Fig. 1) and included 28 HCPs from twelve of the twenty-one general practices participating in the iTAPP. The interviews (n = 17) were 30–60 min and consisted of in-person and video interviews, with 6 individual and 11 group interviews [43, 44]. The first round of interviews held six practices and 12 HCPs, round two was conducted in 11 practices with 25 HCPs including repeat interviews with a subset of participants from round one (Table 1). The participants were interviewed in their practices during working hours and compensated for their time equivalent to their hourly rate. The interviews were semi-structured and guided by the CFIR interview guide available from www.cfirguide.org. We designed the interview guide to have lead questions and follow-up and probe questions within each topic. We used follow-up questions as needed to provide details on a topic, while we omitted questions with information evident prior to the interviews (e.g. role, title). As the FRAME does not provide an explicit interview guide, we compared questions in the FRAME reporting tool to the CFIR interview guide to ensure we covered all relevant aspects related to intervention changes. Supplementary File 1 features the interview guide with a brief description of lead and follow-up questions. For the present study we focused on changes made to the intervention and the CFIR domains Innovation, Inner Setting, and Implementation Process. While this study focuses specifically on these three domains, questions related to the domains “Individual” and “Outer Setting” were included in the interview guide as part of a broader data collection strategy to address multiple research questions across related studies [45]. The first domain, Innovation, includes constructs related to the innovation’s adaptability, trialability, complexity, design, and cost. The Inner Setting domain focuses on the physical infrastructure, work infrastructure, communication, culture, and available resources and materials. The Implementation Process domain focuses on the adaptation process as to the degree to which participants modified and adapted the intervention and/or the inner setting to improve the fit and integration of the intervention into their work [17].
Table 1 Overview of interviewed healthcare professionals (N = 28)Two research assistants transcribed the interviews verbatim.
Data storageData were stored on secure serves hosted by the Region of Southern Denmark at Odense Patient data Explorative Network (OPEN) [46] in compliance with the European General Data Protection Regulations.
AnalysesOur analyses were guided by The Consolidated Framework for Implementation Science (CFIR) [17, 47] and The Framework for Reporting Adaptations and Modifications to Evidence-based interventions (FRAME) [18, 20]. Details on both frameworks are provided below. We analyzed data using directed content analysis [48, 49] using predetermined structure and codes from the CFIR and FRAME. We added codes for each FRAME element to an Nvivo 12 template pre-filled with CFIR determinants (codes) [50]. We then coded data according to the CFIR and FRAME codebooks as provided by the Fidelity, Adaptation, Sustainability, and Training (FAST) Lab at Standford University [51] and by the CFIR research team’s website (www.cfirguide.org) [50]. Additionally, we created a case-memo for each practice with reflections and notes for group discussion.
Data on specific adaptations and modifications were coded to the FRAME and then transferred to a fillable FRAME spreadsheet [51]. Implementation determinants coded to the CFIR were cross-referenced with FRAME codes and the spreadsheet. By combining these two frameworks, we aimed to gain deeper insight into the timing, nature, and reasons behind the identified adaptations and modifications in relations to the ongoing implementation process. While the FRAME focuses on the adaptations and modification to the intervention, and not their derivative effects or the surrounding implementation process [52], the CFIR focuses on implementation determinants both related to the intervention and its deliverers, but also the surrounding implementation process and contexts [17]. The CFIR provides insights into the perceived adaptability of the intervention, contextual factors affecting compatibility, and participants’ reflections on their use of the intervention. Conversely, the FRAME classifies changes according to their nature, level of planning, and their relationship to fidelity in an easily accessible format. By combining the two frameworks, we were able to succinctly classify changes to the 15-method and provide insights into the respondents’ considerations and reasoning behind these changes within their ongoing implementation efforts and work contexts. Notably, we assessed all CFIR constructs from the perspective of the HCPs, including the Implementation Process domain and restricted analysis to CFIR domains “Intervention”, “Inner Setting” and “Implementation Process”, with analysis of data from the Individuals Domain and Outer Setting reported elsewhere [45].
PNS conducted the initial coding and discussed findings with the research team. Re-coded materials were discussed again until consensus. The overall analytic framework and process was overseen by a qualitative research expert unaffiliated with the research group.
Framework for analyzing adaptations and modifications to the intervention: FRAMEThe Framework for Reporting Adaptations and Modifications to Evidence-based interventions (FRAME) [18, 20, 51] encompasses eight elements: (1) when and how the modification was made, e.g. pre-implementation, at scale-up, or during sustainment; (2) whether the modification was planned (proactive) or unplanned (reactive); (3) who decided on the modification, e.g. program leaders, funder, administrator, or recipient; (4) what was modified, such as content, context, training and evaluation, or implementation activities; (5) delivery level of the modification, e.g. individual or group, clinic level, organization, or community; (6) the nature of the context or content modification, such as tweaking, adding elements, loosening the structure, integrating the intervention into other frameworks or protocols, or drifting from the intervention protocol; (7) fidelity-consistency, meaning whether core elements and functions were preserved or changed; (8) the reasons for the modification, such as the goal of the modification, e.g. increase engagement, retention, fit, or to reduce cost, and reason behind the modification, e.g. sociopolitical, organizational, provider-specific, or recipient-specific. The eight elements have been presented in their entirety by Stirman et al. [20].
Framework for analyzing determinants of implementing the intervention: CFIRThe Consolidated Framework for Implementation Science (CFIR) [17, 47] is an implementation determinant framework encompassing 48 distinct constructs across five domains. The five domains focus on the innovation itself, that is the intervention, practice, or protocol being implemented, the Outer Setting, such as the state or system around the inner setting in which the implementation takes place. Further, the Inner Setting in which the implementation takes place, such as a facility or clinic, the individuals’ characteristics and roles, and finally, the Implementation Process, such as the implementation strategies used and the degree to which these are executed. CFIR can be utilized in a variety of ways, including as an implementation planning tool and for post-trial evaluation [47, 53,54,55].
Comments (0)