Bytyqi et al. [3] conducted a comprehensive review of oro-facial subcutaneous dirofilariasis, a disease caused by Dirofilaria species (D. repens and D. tenuis), for which domestic dogs and wild canids serve as definitive hosts. During a blood meal taken from an infected canid, infective larvae are ingested by mosquito species (e.g. Aedes spp., Anopheles spp., or Mansonia spp.), which ultimately renders them infectious [8, 9]. During a subsequent blood meal taken from humans, infective dirofilarial larvae are released into the human accidental host, in whom the larvae eventually develop into adults, migrating in the subcutaneous tissue or forming granulomatous nodules. If manifesting in the oro-facial region, subcutaneous dirofilariasis could be etiologically important in explaining oro-dental clinical phenomena, such as swellings, nodules and potentially even (tooth) pain, caused by edematous swelling exerted onto local nerves by a migrating adult worm, or a juxtaposed granulomatous nodule. Local pressure also inhibits blood flow, which in theory could cause dental ischemia and thereby lead to tooth loss. Lastly, it is theoretically possible that systemic or local inflammatory activity caused by filarial infection creates a procarcinogenic environment, potentially contributing to the formation of oral cancer.
Dirofilariasis was most commonly reported from the WHO European Region (53.9%; 55/102), and the WHO South-East Asian Region (37.3%; 38/102) followed by a few reports from the WHO Region of the Americas (4.9%; 5/102), the WHO Eastern Mediterranean Region (2.9%; 3/102) and the WHO Western Pacific Region (1%; 1/102) [3].
The median age of dirofilariasis cases was 39 years (IQR: 28 to 52 years), and females and males were equally often affected (49% [49/101] and 51% [52/101], respectively). Oro-facial dirofilariasis was almost exclusively caused by D. repens (98%; 81/83), with only two cases attributed to D. tenuis (2%). However, it is worth mentioning that definitive Dirofilaria species diagnosis was not performed in 18.6% of cases (19/102). The most commonly affected oro-facial site was the cheek (63.7%; 65/102), followed by the face (17.7%; 18/102), the lip (7.8%; 8/102) and the jaw (6.9%; 7/102); furthermore, there was each a case with involvement of the nasolabial region, the oral cavity, the soft palate and the tongue, respectively. Cases for whom therapy was reported (n = 55) mainly underwent surgical removal (89%; 49/55) or surgical removal including anti-filarial treatment (5%; 3/55). In two cases, the swelling was squeezed, and a worm was recovered, and lastly, in one case, the nodule developed into an abscess, which burst and revealed a white worm. They also stated that oro-facial dirofilariasis caused by D. repens represents the vast majority of oro-facial filariasis, followed by a small non-dirofilarial minority represented by W. bancrofti and O. volvulus [3].
Oro-facial dirofilariasis manifests exclusively as nodules or swellings in different tissue locations. This is in line with the biology of the adult stages of D. repens and D. tenuis, both of which are commonly found in subcutaneous tissue [8]. While swellings (some of which can appear to migrate) are often described as being caused by the active migration of the adult worm, subcutaneous nodules are formed by adult worms whose migration is rendered stationary by the host’s immune system [10]. Characteristically, many case reports reported swellings of subcutaneous tissue for weeks to months, which often spontaneously increased and decreased in size and finally manifested into a single, mobile, soft, or firm nodule. Also, in line with the literature, these nodules and swellings are mostly asymptomatic; however, they can become painful if the immune system of the host attempts to clear the active infection [11]; again, this is congruent with our findings since pain and dysesthesia combined constituted 71% (10/14) of symptoms in symptomatic oro-facial dirofilariasis. Interestingly, most manifestations of oro-facial dirofilariasis occurred on the cheek and face, and to a lesser extent, on the lip, jaw, and other areas. However, it is believed that these are not true predilection sites, but artefacts resulting from categorising the human body into anatomical regions, some of which are naturally larger than others. Furthermore, the recommended treatment of general dirofilariasis caused by D. repens or D. tenuis is surgical removal [11].
The vast majority of dirofilariasis was caused by D. repens (98%), followed by D. tenuis, while D. immitis caused no cases. This phenomenon can be explained via parasite biology since adults of D. immitis are described to inhabit the intravascular space primarily of pulmonary arteries, and not subcutaneous tissue (which is the case for adults of D. repens and D. tenuis) [8].
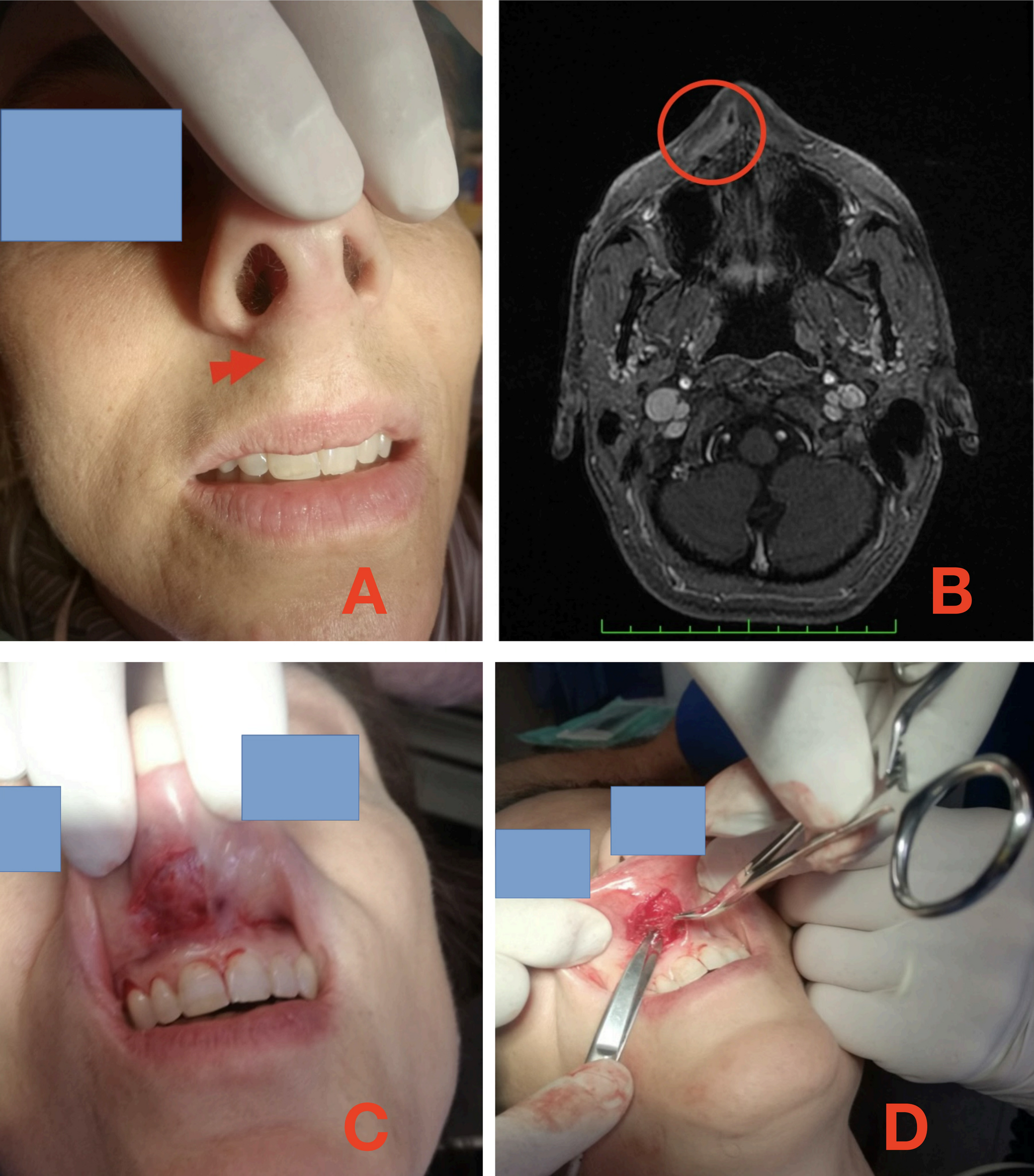
Deducting from the reported extensive review [3], the case we report should be the second in the world to affect the nasolabial region and falls within the 20% of symptomatic cases. Pre-diagnosis course fully replied to the most common evolution: lump migration, sensorial impairment of the face, immune system reaction aimed to eliminate the pathology, months from the beginning of the symptoms/signs to the removal.
Parasites can rarely be identified at histopathological examination, and, most often, only degenerated, dead nematode structures are observed. This finding can sometimes be the only way to diagnose such infections. The patient’s referred history of exposure can also provide supportive information.
In our case, we examined histological sections of adipose and skeletal muscle tissue from the nasolabial area. We observed a prominent inflammatory infiltrate consisting of lymphocytes, plasma cells, histiocytes, eosinophils, and giant cells. Additionally, a central area of suppuration with abundant neutrophils surrounding a degenerating filaria was evident. We were able to identify a thick, laminated chitinous cuticle with longitudinal ridges and large lateral cords, displaying the characteristic arrangement of smooth muscle fibres. The presence of these structures was crucial in suggesting a diagnosis of Dirofilaria sp.
It is crucial to consider that many different worms share morphological features; moreover, other types of foreign bodies should be considered in the differential diagnosis, together with infections, tumors, inflammatory dyseases and cysts. This point highlights the importance of thorough examination and evaluation of all possible factors when diagnosing parasitic infections.
Molecular methods, such as PCR, can detect parasite DNA in blood and may be helpful in occult or suspected cases [12]. However, in this patient, histology alone was sufficient to establish the diagnosis.
Meanwhile, in the absence of adequate clinical and epidemiological research results, oral health providers should consider parasitological etiologies in the manifestations of oro-facial diseases, particularly in patients at high risk of carrying a specific parasitic infection. Unfortunately, oral health providers were often not exposed to the idea in dental medicine curricula that parasites can be an underlying cause of certain oro-facial diseases. This educational gap is even further complicated by the fact that parasite-specific characteristics (e.g. life cycles, risk factors, or disease manifestation) can be vastly different among parasitic diseases.


Comments (0)