
Remember me
Journal of Anesthesia, Analgesia and Critical Care 2025,5(1):A86
Background
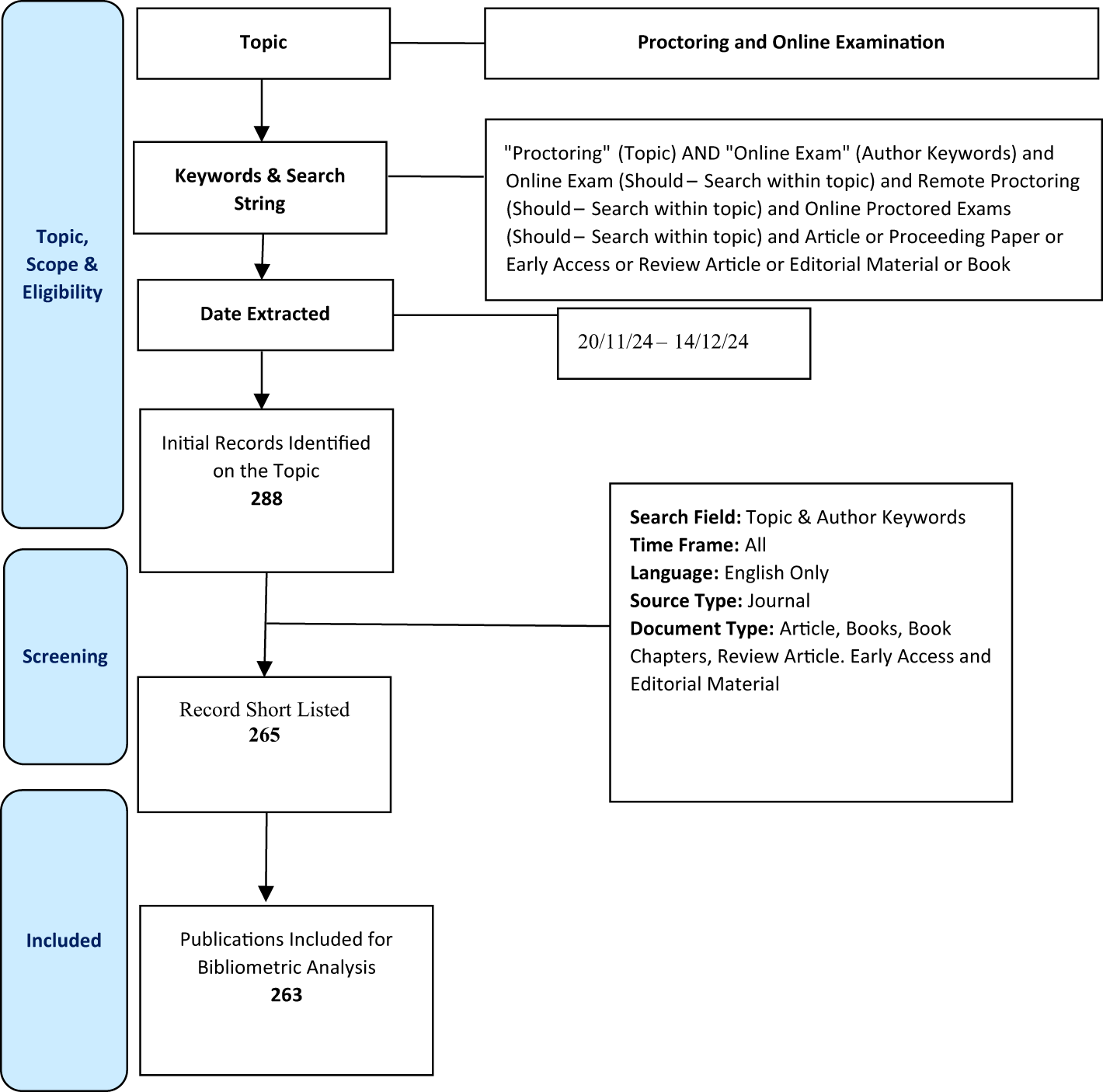
Timely identification of pathogens and appropriate antimicrobial therapy are critical in the management of bloodstream infections (BSIs), particularly in intensive care settings. In 2024, a multidisciplinary team at Fondazione IRCCS Ca’ Granda Policlinico Hospital (Milan) designed and introduced diagnostic pathways tailored for BSIs (fig.1 e fig.2), based on the review of local epidemiology (hospital cumulative antibiograms) and availability of fast-microbiology diagnostic strategies.
Methods
BSI episodes managed before (2023) and after (2024) algorithms implementation were retrospectively compared.
Outcomes included microbiological turnaround time - from sample collection to first microbiological data (pathogen identification and/or resistance pattern) and the proportion of patients receiving antibiotic optimization within 72 hours from blood culture collection (i.e., how often and how rapidly treatments were de-escalated or changed once microbiological data became available). All patients signed BSI-STUDY consent.
Results
A total of 73 BSI episodes were analyzed, 32 from the pre-implementation period and 41 post-implementation period (Tab.1).
Most cases originated in the emergency department 38 (52%) or the ICU 19 (26%), with sepsis or septic shock present in 78% of cases at onset. The most frequently isolated pathogens included Escherichia coli 13/73 (17.8%), Klebsiella pneumoniae 10/73 (13.6%), and Staphylococcus aureus 9/73 (10.9%). Multidrug-resistant organisms accounted for 28/73 (38.3%) of isolates, with similar proportions across Gram-positive and Gram-negative infections. (Tab. 2).
The use of BCID2 rose from 12% in the pre-intervention group to 60% post-intervention (p<0.0001). Following implementation, median microbiological turnaround time decreased significantly (30 [IQR 22–70] vs 77 [IQR 42–129] hours; p=0.003), and early antibiotic therapy optimization became more frequent (43.9% vs 16%; p=0.008). No significant difference was observed in the overall duration of antibiotic treatment between groups.
Conclusions
The adoption of structured, pathogen-specific diagnostic algorithms - supported by fast molecular microbiology - was associated with faster microbiological reporting and a significant improvement in early antibiotic adjustments. Ongoing evaluation will assess their long-term influence on antimicrobial consumpion and resistance patterns over time.
Consent
Informed consent was obtained for the publication of this scientific article.
References
Peri A, Ling W et al. Performance of BioFire Blood Culture Identifcation 2 Panel (BCID2) for the detection of bloodstream pathogens and their associated resistance markers: a systematic review and meta-analysis of diagnostic test accuracy studies. BMC Infectious Diseases (2022).
Timsit JF, Ruppé E, Barbier F, Tabah A, Bassetti M. Bloodstream infections in critically ill patients: an expert statement. Intensive Care Med. 2020 Feb;46(2):266-284.
Chang CM, Hsieh MS, Yang CJ, How CK, Chen PC, Meng YH. Effects of empiric antibiotic treatment based on hospital cumulative antibiograms in patients with bacteraemic sepsis: a retrospective cohort study. Clin Microbiol Infect. 2023 Jun;29(6):765-771.
Fig. 1 (abstract A86).
Empiric therapy algorithm for BSI caused by Gram +
Fig. 2 (abstract A86).
Empiric therapy algorithm for BSI caused by Gram -
Table 1 (abstract A86). Epidemiological data. Continuous variables are expressed as median (Q1-Q3), categorical are expressed as n (%) Table 2 (abstract A86). Clinical and microbiological data. Continuous variables are expressed as median (Q1-Q3), categorical are expressed as n (%). *Genitourinary, intestinal traslocation, CNS; **S. epidermidis; ***Enterobacter hormaechei, Klebsiella spp; ****Neisseria meningitidis, Salmonella spp, Bacteroides spp, Citrobacter sppA87 Use of pentaglobin in a patient affected by neisseria meningitidis serogroup BM. Toma, D. Puscio, G. Paiano, D. Mastria, L. Giaccari, R. De Maglio, R. Barbieri, F. Madaro, G. Pulito, L. MasciaUOC Anestesia E Rianimazione - P.O. Vito Fazzi, Lecce, Italy Correspondence: M. TomaJournal of Anesthesia, Analgesia and Critical Care 2025,5(1):A87
Meningitis caused by Neisseria Meningitidis, a serious infectious disease caused by Gram-negative diplococcus, despite having an incidence in Italy of 0.14 cases per 100,000 inhabitants (ISS 2024 data), continues to have a high rate of hospitalization in intensive care, permanent sequelae and mortality despite timely treatment. Adjuvant therapy with IgM seems to be a promising solution for the control of severe infection by N. meningitidis because it neutralizes bacteriotoxins, exotoxins and improves opsonization and phagocytosis of pathogens. The only available polyclonal drug preparation enriched with IgM immunoglobulins is Pentaglobin (Biotest-AG, Dreieich, Germany); This contains 76% IgG, 12% IgA and 12% IgM and has shown greater efficacy in vitro against gram-negative bacteria through the improvement of the phagocytosis process. In a study conducted in Tuscany in 2017, it was seen how the group treated with Pentaglobin had a lower mortality rate than the control group.
Case report (Informed consent to the processing of personal data required): 35-year-old male patient went to the emergency room for hyperpyrexia (for about 2 days), vomiting and appearance of diffuse blood extravasations all over the body and confusion (Fig. 1). He arrived disoriented and uncooperative with initial signs of nuchal rigidity. Given the neurological picture and the presence of a septic picture (Lat: 3.8; PCT 58.8) the patient was transferred to intensive care. He performed a negative total body CT scan and a lumbar puncture which was positive for Neisseria Meningitidis. During hospitalization in intensive care the patient maintained spontaneous breathing, neurologically intact with stable hemodynamics. Upon admission the patient was treated with Ceftriaxone 2 g x 2/day, replaced with Meropenem 2 g x 3/day and Linezolid 600 mg x 2/day. Pentaglobin 50mg/ml at 36 ml/h was then started. The clinical picture began to improve the day after admission with progressive improvement of laboratory tests and reduction of hemorrhagic petechiae (Fig 2). After a week of hospitalization, the patient was discharged.
The case report we described highlights the efficacy of IgM immunoglobulins in Neisseria-mediated meningitis and shows a rapid improvement of the patient's clinical and laboratory picture, confirming Pentaglobin as a key player in fighting meningeal infections.
Consent
Informed consent was obtained for the publication of this scientific article.
Fig. 1 (abstract A87).
DIFFUSE BLOOD EXTRAVASATIONS ALL OVER THE BODY
Fig. 2 (abstract A87).
WHITE BLOOD CELL COUNT AND PCT TREND DURING THE DAYS OF HOSPITALISATION
A88 Point-of-care evaluation of fibrinolysis in Sepsis: the pocefis studyI. Silvestri1,3, C. Bonetti1, A. Caccioppola2, A. Meli2, G. Corica1, E. Bellavia1, A.G. Motta1, A. Rosati1, G. Zimei1, F. Cappelli1, G. Grasselli1,2, M. Panigada2 1Department of pathophysiology and transplantation, University of Mila, Milano, Italy; 2Intensive care unit, IRCCS Ca'Granda Fondazione, Milano, Italy; 3Policlinico di Milano Ospedale Maggiore | Fondazione IRCCS Ca'Granda, Milano, Italy Correspondence: I. SilvestriJournal of Anesthesia, Analgesia and Critical Care 2025,5(1):A88
Background
Fibrinolytic shutdown is a recognized phenomenon observed in septic patients and is associated with worsened prognosis. However, a standardized, bedside diagnostic approach still lacks. The ClotPro® viscoelastic assay, specifically its TPA-test, offers a point-of-care method to quantify fibrinolysis impairment by measuring lysis time (LT) and maximum lysis (ML). The POCEFIS study aims to assess the prevalence and clinical relevance of impaired fibrinolysis in sepsis.
Methods
This single-center, prospective cohort study enrolled adult ICU patients with a diagnosis of sepsis or septic shock, admitted to the adult ICU of Policinico Hospital of Milan, Italy.. Exclusion criteria included ECMO, history of known coagulopathies and oral anticoagulation therapy.. Patients were enrolled within 12 hours from the diagnosis of sepsis or septic shock. The primary endpoint was the prevalence of fibrinolysis impairment based on prolonged LT on the ClotPro® TPA-test. Secondary outcomes included associations with standard coagulation tests, inflammatory biomarkers, organ dysfunction (SOFA score), ICU mortality, and ICU length of stay.
Standard laboratory tests, ClotPro® (including TPA, EX, IN, FIB, and AP-tests), and VCM were performed at enrollment, and on day 1, 2, 3, and 7 after enrollment. Biomarkers such as PAI-1, plasminogen, IL-6, and TNF were measured at enrollment and on day 2 and 7.
Results
From January 2024 to April 2025, 57 patients were enrolled in the study.. Fibrinolysis response was categorized based on TPA lysis time, with a cut-off of 411 seconds. 23 patients (40.4%) had normal response, and 34 (59.6%) showed altered fibrinolysis. No significant differences in age, sex, BMI, comorbidities, or site of infection were observed between groups. ICU mortality was similar in the two groups (13.0% vs. 14.7%, p=1.00).
While SOFA scores at enrollment did not differ significantly, patients with altered fibrinolysis showed higher SOFA scores on day 2 (11.1 ± 2.3 vs. 8.9 ± 3.0, p=0.029), suggesting a transient association with organ dysfunction. Trends over the first 72 hours revealed that persistent fibrinolysis impairment was associated with higher inflammatory markers (e.g., IL-6, TNF), elevated fibrinogen and PAI-1, and reduced plasminogen levels. A subgroup of 13 patients (22.8%) exhibited severe fibrinolysis resistance persisting across all time points, with biochemical markers suggestive of consumptive coagulopathy.VCM analysis confirmed lower maximum lysis (ML%) in the resistant group, particularly on days 1 and 2, supporting the ClotPro® findings.
Conclusions
The ClotPro® TPA-test effectively identifies fibrinolysis impairment in septic ICU patients. Nearly 60% of cases exhibited altered fibrinolysis at enrollment, with variable recovery trajectories. Persistent resistance was associated with elevated inflammatory and antifibrinolytic markers, but not conclusively with worse clinical outcomes in this preliminary analysis. VCM Results paralleled ClotPro® findings, further validating the presence of a hypofibrinolytic phenotype. These insights support the use of bedside viscoelastic testing for early phenotyping of septic patients and potential guidance of individualized therapeutic strategies in sepsis induced coagulopathy.
Consent
Informed consent was obtained for the publication of this scientific article.
References
1.Iba T, Umemura Wada Levy JH. Roles of Coagulation Abnormalities and Microthrombosis in Sepsis: Pathophysiology, Diagnosis, and Treatment. Arch Med 2021;52(8):788-797.https://doi.org/10.1016/j.arcmed.2021.07.003
2.M. Panigada et al., ‘Assessment of Fibrinolysis in Sepsis Patients with Urokinase Modified Thromboelastography’,2015,https://doi.org/10.1371/journal.pone.0136463.
A89 Two cases of acinetobacter baumannii-related ventriculitis following external ventricular drain placementD. Scarano, C. Bussemi, A. Piedepalumbo, A. Lucarelli, F. Scarpato, D. CarbonePresidio Ospedaliero Umberto I, Nocera Inferiore, Italy Correspondence: A. PiedepalumboJournal of Anesthesia, Analgesia and Critical Care 2025,5(1):A89
Background
Ventriculitis is an infection of cerebral ventricles that may result from meningitis, open head trauma, neurosurgical procedures, or the placement of devices such as an external ventricular drain (EVD). The clinical presentation includes fever, altered level of consciousness, and, in advanced cases, nuchal rigidity and signs of intracranial hypertension. Diagnosis is based on cerebrospinal fluid (CSF) analysis—typically showing leukocytosis, hypoglycorrhachia, and elevated protein levels—CSF cultures for pathogen identification, and neuroimaging (CT or MRI) that may reveal ependymal enhancement and thickening, periventricular edema, and hydrocephalus. Certain conditions, such as EVD placement, prolonged ICU stay, and immunosuppression, are risk factors for ventriculitis due to multidrug resistant bacteria such as Acinetobacter baumannii. Treatment includes removal or replacement of the infected catheter and targeted antibiotic therapy, either intravenous and/or intrathecal, according to antimicrobial susceptibility testing.
Case Report
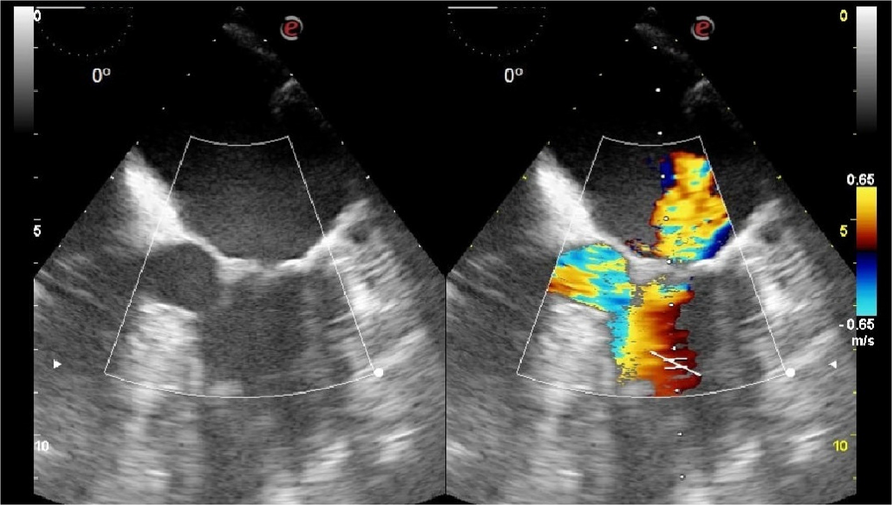
We report two cases of ventriculitis caused by extensively drug-resistant (XDR) Acinetobacter baumannii, arising after EVD placement in patients admitted to the intensive care unit for acute cerebral hemorrhagic events. The first patient, a 62-year-old man, was admitted for hypertensive intracerebral hemorrhage. The second case involved a 77-year-old woman with subarachnoid hemorrhage caused by the rupture of an aneurysm of the right middle cerebral artery. Both patients developed complications from their condition which required placement of an EVD. After 7 days from placement in the first case and after 5 days in the second, both patients showed rapid neurological deterioration with sudden decrease in the GCS score, fever and elevated inflammatory markers. Blood cultures were negative in both cases. MRI was suggestive of ventriculitis (Figure 1,2,3), which was subsequently confirmed by CSF analysis and culture isolation of XDR A. baumannii. Treatment included a combined antimicrobial approach with 0.125 MU/day of intrathecal colistin and intravenous cefiderocol (6 g/day), fosfomycin (16g/day) and colistin (4.5 MU/bid). The EVDs were removed and replaced with new ventricular catheters dedicated to intrathecal colistin administration. In both cases, microbiological sterilization of the CSF was achieved within approximately 10 days, along with clinical and radiological improvement. Antibiotic therapy continued for 14 days. No adverse events related to intrathecal colistin administration were observed. The ventricular catheters were later removed without complications, and both patients were discharged from the ICU with preserved cognitive and motor functions.
Conclusion
This case series highlights the effectiveness and safety of intravenous cefiderocol, fosfomycin and colistin in combination with intrathecal colistin. The combined approach, in addition to demonstrating a good safety profile, led to resolution of the infection, suggesting a potential benefit in case of MDR pathogens. These preliminary results are promising; however, further confirmation is needed through prospective, randomized studies to establish the role of this antibiotic regime and to develop shared therapeutic guidelines, particularly given the limited number of Acinetobacter-related ventriculitis cases reported in the scientific literature.
Written informed consent was obtained from the patients for publication of this case report and any accompanying images or clinical data.
Consent
Informed consent was obtained for the publication of this scientific article.
References
1.Ulloque-Caamaño L, Mo-Carrascal J, Maraby J, Narvaez-Rojas A, Quintana-Pajaro L, Ramos-Villegas Y, Moscote-Salazar LR. Ventriculitis associated with extraventricular drainage: etiology, diagnosis and treatment focused on neurocritic care units. Cir Cir. 2019;87(2):230-240. English. https://doi.org/10.24875/CIRU.18000052. PMID: 30768063.
2.Hasbun R. Healthcare-associated ventriculitis: current and emerging diagnostic and treatment strategies. Expert Rev Anti Infect Ther. 2021 Aug;19(8):993-999. https://doi.org/10.1080/14787210.2021.1866544. Epub 2020 Dec 24. PMID: 33334204.
3.Karaiskos I, Galani L, Baziaka F, Giamarellou H. Colistina intraventricolare e intratecale come ultima risorsa terapeutica per il trattamento della ventricolite e meningite da Acinetobacter baumannii multifarmaco-resistente ed estesamente farmaco-resistente: una revisione della letteratura. Int J Antimicrob Agents. Giugno 2013;41(6):499-508. https://doi.org/10.1016/j.ijantimicag.2013.02.006. Epub 16 marzo 2013. PMID: 23507414.
4.Karaiskos I, Galani L, Baziaka F, Giamarellou H. Colistina intraventricolare e intratecale come ultima risorsa terapeutica per il trattamento della ventricolite e meningite da Acinetobacter baumannii multifarmaco-resistente ed estesamente farmaco-resistente: una revisione della letteratura. Int J Antimicrob Agents. Giugno 2013;41(6):499-508. https://doi.org/10.1016/j.ijantimicag.2013.02.006. Epub 16 marzo 2013. PMID: 23507414.
Fig. 1 (abstract A89). Fig. 2 (abstract A89).
Fig. 2 (abstract A89). Fig. 3 (abstract A89).
Fig. 3 (abstract A89). A90 Impact of extracorporeal membrane oxygenation on incidence rates of bacterial bloodstream infections and ventilator-associated pneumoniaM. Petrone1, V. Vago1, T. Mara2, A. Chiara3, B. Alessandra4,5, G. Amedeo3, M. Davide4, M. Andrea3, P. Mauro3, G. Giacomo3,5, S. Vittorio3,6
1School of Specialization in Anesthesia Intensive Care, and Pain Management, University of Milan, Italy; 2School of Specialization in Infectious Diseases, University of Milan, Italy; 3Department of Anesthesia, Critical Care and Emergency, Intensive Care and Emergency, Foundation IRCCS Ca'Granda Hospital, Milan, Italy; 4Infectious Diseases Unit, Foundation IRCCS Ca'Granda Ospedale Maggiore Policlinico, Milan, Italy; 5Department of Pathophysiology and Transplantation, University of Milan, Italy; 6Department of Biomedical, Surgical and Dental Sciences, University of Milan, Italy
Correspondence: M. Petrone
A90 Impact of extracorporeal membrane oxygenation on incidence rates of bacterial bloodstream infections and ventilator-associated pneumoniaM. Petrone1, V. Vago1, T. Mara2, A. Chiara3, B. Alessandra4,5, G. Amedeo3, M. Davide4, M. Andrea3, P. Mauro3, G. Giacomo3,5, S. Vittorio3,6
1School of Specialization in Anesthesia Intensive Care, and Pain Management, University of Milan, Italy; 2School of Specialization in Infectious Diseases, University of Milan, Italy; 3Department of Anesthesia, Critical Care and Emergency, Intensive Care and Emergency, Foundation IRCCS Ca'Granda Hospital, Milan, Italy; 4Infectious Diseases Unit, Foundation IRCCS Ca'Granda Ospedale Maggiore Policlinico, Milan, Italy; 5Department of Pathophysiology and Transplantation, University of Milan, Italy; 6Department of Biomedical, Surgical and Dental Sciences, University of Milan, Italy
Correspondence: M. PetroneJournal of Anesthesia, Analgesia and Critical Care 2025,5(1):A90
Background
Extracorporeal membrane oxygenation (ECMO) is a life-saving support for patients with refractory cardiac or respiratory failure. Its potential role in promoting nosocomial infections, such as ventilator-associated pneumonia (VAP) and bloodstream infections (BSI), remains unclear. This study investigates the association between ECMO and BSI/VAP.
Methods
This retrospective observational study includes all consecutive adult patients admitted to the ICU of Ospedale Policlinico in Milan for >48h. Patients mechanically ventilated for <48h were not considered for VAPs.
Only the first microbiologically-confirmed bacterial infection leading to the initiation/modification of an antimicrobial therapy was considered.
We defined infection time at risk: a) for BSI from 48 hours after ICU admission until discharge, infection, or death; b) for VAP from 48 hours after intubation until extubation, infection, or death.
Crude incidence and incidence rate (IR) were calculated for BSI/VAP in ECMO and non-ECMO patients. A univariate Fine and Gray competing risk analysis was performed, considering death as a competing event. ECMO was considered a time-varying variable, with an ECMO-related infection timeframe starting and ending 48 hours after ECMO initiation and decannulation.
Results
From January 1, 2023, to December 31, 2024, 404 patients were admitted to ICU. 204 stayed in the ICU for >2 days and were included in the analysis. Median age was 60 [IQR 49–68], 144 (71%) were male; 133 (66%) patients were intubated for 7 [3–17] days.
Forty-two (21%) patients received extracorporeal support, mainly for respiratory failure (34 VV-ECMO, 6 ECCO2R, 2 VA-ECMO) for 6.5 [4–10] days. Six were not intubated during ECMO, one was intubated for <2 days.
BSI occurred in 18 (9%) patients (12 (7%) non-ECMO vs. 6 (14%) ECMO patients, p=0.098). VAP occurred in 16 (12%) intubated patients (13 (13%) non-ECMO vs. 3 (9%) ECMO patients, p=0.464). Two (11%) BSIs and 9 (56%) VAPs were polymicrobial. 17/48 (35%) isolates were multidrug-resistant (10/28 (36%) of Gram-negative vs. 7/20 (35%) of Gram-positive bacteria). Table 1 shows details of the microbiological isolates.
BSI and VAP IRs were 8.6 (5.4–13.6) and 16.2 (9.9–26.5) infections/1000 days-at-risk, respectively. Figures 1 and 2 show the cumulative incidence of BSI and VAP.
The risk factors analysis detected no difference in BSI hazard (IR (95%CI) 8.1 (4.8–13.7) vs. 10.7 (4.0–28.5) infections/1000 days-at-risk, sHR (95%CI) 1.02 (0.94–1.10), p=0.654) and VAP hazard (IR 18.5 (10.7–31.8) vs. 10.6 (3.4–32.8) infections/1000 days-at-risk, sHR 0.62 (0.18–2.08), p=0.435) between non-ECMO and ECMO patients, respectively.
Conclusions
In our population, ECMO did not seem to increase the risk of bacterial BSI and VAP.
Consent
Informed consent was obtained for the publication of this scientific article.
References
1.Grasselli G, Scaravilli V, Di Bella S, Biffi S, Bombino M, Patroniti N, et al. Nosocomial infections during extracorporeal membrane oxygenation: Incidence, etiology, and impact on patients’outcome. Crit Care Med.2017;45(10).
2.Abrams D, Grasselli G, Schmidt M, Mueller T, Brodie D. ECLS-associated infections in adults: what we know and what we don’t yet know. Intensive Care Med.2020;46(2).
3.Peña-López Y, Machado MC, Rello J. Infection in ECMO patients: Changes in epidemiology, diagnosis and prevention. Anaesth Crit Care Pain Med.2024;43(1).
Fig. 1 (abstract A90). Table 1 (abstract A90). Microbiological isolatesA91 Cerebrospinal fluid (CSF) lactate measurement as a diagnostic and prognostic tool in suspected cns infections in emergency departmentE. Petrillo1, M.A. Zingaropoli2, G. Imbimbo3, R. Renna1, P. Pasculli2, A. Falcou4, M.R. Ciardi2, G. Galardo1
1Dipartimento Emergenza Accettazione, Area Critica e Trauma Policlinico Umberto 1, Roma, Italy; 2Dipartimento di Malattie Infettive, Sapienza Università di Roma, Roma, Italy; 3Dipartimento di Medicina Traslazionale e di Precisione, Sapienza Università di Roma, Roma, Italy; 4Dipartimento Emergenza Accettazione, Area Critica e Trauma- UTN, Policlinico Umberto 1, Roma, Italy
Correspondence: E. Petrillo
Table 1 (abstract A90). Microbiological isolatesA91 Cerebrospinal fluid (CSF) lactate measurement as a diagnostic and prognostic tool in suspected cns infections in emergency departmentE. Petrillo1, M.A. Zingaropoli2, G. Imbimbo3, R. Renna1, P. Pasculli2, A. Falcou4, M.R. Ciardi2, G. Galardo1
1Dipartimento Emergenza Accettazione, Area Critica e Trauma Policlinico Umberto 1, Roma, Italy; 2Dipartimento di Malattie Infettive, Sapienza Università di Roma, Roma, Italy; 3Dipartimento di Medicina Traslazionale e di Precisione, Sapienza Università di Roma, Roma, Italy; 4Dipartimento Emergenza Accettazione, Area Critica e Trauma- UTN, Policlinico Umberto 1, Roma, Italy
Correspondence: E. PetrilloJournal of Anesthesia, Analgesia and Critical Care 2025,5(1):A91
Background
Infectious meningitis and encephalitis are major causes of morbidity and mortality worldwide, posing a severe threat to life if not promptly diagnosed and treated. Early diagnosis and appropriate management, facilitated by accurate etiological identification, significantly improve patient outcomes. However, achieving a precise diagnosis can be challenging due to the non-specific initial clinical presentations of many Central Nervous System (CNS) infections. Moreover, distinguishing between meningitis and encephalitis can be difficult, as their clinical presentations often overlap. Lactate levels in cerebrospinal fluid (CSF) are increase, due to the oxidative stress of neuroinflammation and CSF levels are independent from blood lactate levels. In previous studies, blood gas analyser was used as a rapid assay to assess CSF lactate levels at the patient’s bedside.
By this study we aimed at investigating the association between CSF lactate levels with i) the presence of meningitis and encephalitis and ii) its association with clinical outcomes.
Materials and Methods
This is a observational single center study conducted at the Emergency Department (ED) of Sapienza University of Rome, Policlinico Umberto I University Hospital in collaboration with the Department of Public Health and Infectious Diseases, Sapienza University of Rome. We enrolled patients with suspected meningitis or encephalitis, requiring lumbar puncture for diagnosis. The CSF lactate levels were measured immediately on a point-of-care analyser (Abbott i-STAT analyser, Abbott Park, IL, USA) available in the ED. The study was approved by the Local Ethical Committee and performed in accordance the Declaration of Helsinki. All the patients signed the informed consent. Receiver operating characteristic (ROC) analysis and multivariate logistic regression were employed to evaluate the diagnostic performance of CSF lactate levels and identify factors associated with ICU admission, respectively.
Results
We enrolled 100 patients (50% male) with a mean age of 57.2 ± 21.8 years. Among them, 18 were diagnosed with meningitis, 21 with encephalitis, and 61 with non-CNS infectious diseases. CSF lactate levels were available for 80 participants. Patients with meningitis showed significantly higher mean CSF lactate levels (9.8 ± 6.4 mg/dL) compared to those with non-CNS infections (2.0 ± 0.7 mg/dL, p < 0.001), and a non-significant trend toward higher levels compared to patients with encephalitis (2.4 ± 0.9 mg/dL, p = 0.054). ROC analysis demonstrated good diagnostic performance of CSF lactate in identifying meningitis, with an AUC of 0.820 (p < 0.001). No significant differences were observed between the AUCs of CSF lactate, glucose (0.760), and protein (0.851). In a multivariate logistic regression analysis including age, sex, CRP, CSF glucose, CSF protein, and diagnosis (meningitis or encephalitis), only CSF lactate levels were significantly associated with increased risk of ICU admission (OR = 1.567, 95% CI: 1.045–2.350, p = 0.030).
Conclusion
CSF lactate levels measured at the bedside in the Emergency Department demonstrated strong diagnostic performance for identifying meningitis and were independently associated with ICU admission. These findings support the potential utility of CSF lactate as a rapid, reliable biomarker to guide early clinical decision-making in suspected CNS infections.
Consent
Informed consent was obtained for the publication of this scientific article.
A92 The control of bacterial infections of the oral cavity in intensive care patientsC.M. Petrangeli1, A.K. Vergou2, M. Ciotti3, F.M. Petrangeli4, F. Semenzato5, C. Sicignano3, F. Claro1, M. Martucci1, V. De Angelis1, F. Frisardi1, S. Verrengia1, I. Brandolini1, D.J. Brunetti1, D. Cipollone1, M. Silvi1, T. Galli1, C. Manni1, S. Di Florio1, F. Leonardis1 1UOSD Terapia Intensiva Policlinico Tor Vergata, Roma, Italy; 2UOSD Microbiologia e Virologia Policlinico Tor Vergata, Roma, Italy; 3UOSD Odontoiatria Policlinico Tor Vergata, Roma, Italy; 4Dipartimento di Matematica Università Sapienza, Roma, Italy; 5Facoltà di Medicina e Chirurgia Università Tor Vergata, Roma, Italy Correspondence: C.M. PetrangeliJournal of Anesthesia, Analgesia and Critical Care 2025,5(1):A92
Background
Daily hygiene of the oral cavity of patients admitted to intensive care, reducing the presence of bacteria in the oral cavity, is a practice that increases the chances of improving the clinical status of patients with bacterial pneumonia.
Materials and Methods
We carried out our study to search for the presence of pathogenic microorganisms of the oral cavity in patients admitted to intensive care and verify a percentage difference in their presence in discharged patients compared to that in deceased patients. We enrolled 40 patients admitted to the ICU suffering from bacterial pneumonia, all on mechanical ventilation via orotracheal tube or tracheostomy cannula. Of the 40 patients (22 males and 18 females), 25 were discharged (13 males and 12 females) while 15 died (9 males and 6 females). The micro-IDent plus 11 kit we used allowed us to search for the following microorganisms: Aggregatibacter actinomicetemcomitans, Porphyromonas gingivalis, Prevotella intermedia, Tannerella forsythia, Troponema denticola, Parvimonas micra, Fusobacter nucleatum, Campylobacter rectus, Eubacterium nodatum, Eikenella nodatum, Capnocytophaga spp. Each patient underwent oral hygiene two hours before the sampling carried out by the dentist specialist in the periodontal sac of four different teeth, two of the upper arch and two of the lower arch. Oral hygiene was performed according to ward protocol with a cleaning brush and aspirator using 0.12% chlorhexidine associated with dental gel for 5 minutes. The samples taken were analyzed to our microbiology laboratory using the technique of bacterial DNA extraction and amplification according to the GenoLyse protocol (Bruker, Germany).
Results
The results obtained showed that in patients who arrived at discharge, the overall percentage of the 11 bacterial species sought was 45% while in deceased patients the percentage rose to 64%. The data collected therefore confirm that the presence of these bacterial species in the oral cavity in ventilated patients with bacterial pneumonia is significantly higher in deceased patients than in discharged patients.
Consent
Informed consent was obtained for the publication of this scientific article.
References
1.Rabello F, A. V. Effectiveness of oral chlorhexidine for the prevention of nosocomial pneumonia and ventilator-associated pneumonia in intensive care units: Overview of systematic reviews. Int. J. Dent Hyg. 2018 Nov; 16(4): 441-449.
2.Vidal CF, Vidal AK, Monteiro JG Jr Cavalcanti A, and others. Impact of oral hygiene involving toothbrushing versus chlorhexidine in the prevention of ventilator-associated pneumonia: a randomized study. BMC Infect Dis. 2017 Jan; 17(1): 112.
A93 Healthcare-associated infections in ecmo patients: a retrospective single-center study on incidence and outcomesM. Orlandi, A. De Felice, A. Cardoni, G. Cianchi, M. BonizzoliAOU Careggi, Firenze, Italy Correspondence: M. OrlandiJournal of Anesthesia, Analgesia and Critical Care 2025,5(1):A93
In recent years, the use of Extracorporeal Membrane Oxygenation (ECMO) therapy has seen significant growth, especially following the COVID-19 pandemic, which highlighted its usefulness in managing the most severe cases of respiratory failure. However, patients undergoing ECMO are extremely vulnerable to healthcare-associated infections (HAIs), complications that negatively impact clinical outcomes and significantly increase mortality. This abstract, based on the retrospective single-center observational study'ECMOin'conducted at the Careggi University Hospital in Florence, analyzed data from 67 patients treated with veno-venous ECMO between 2021 and 2024. The study aimed to describe the clinical, microbiological, and epidemiological characteristics of ECMO-related infections, identify associated risk factors, and assess their prognostic impact. Informed consent was obtained from the patient and/or family members.
The analysis revealed an overall HAI incidence of 35.9 episodes per 1,000 ECMO days. The most frequent infections were ventilator-associated pneumonia (HAP/VAP), followed by primary bloodstream infections and central line-associated bloodstream infections (CR-BSI). A clear correlation emerged between prolonged ECMO support (>21 days) and increased infection risk, confirming the need for early weaning strategies. Moreover, there was a high prevalence of multidrug-resistant (MDR) pathogens, particularly Klebsiella pneumoniae KPC and vancomycin-resistant Enterococcus (VRE), with increased colonization observed during intensive care stays.
Overall mortality was 44.8%, with 66.7% of deaths partially attributed to nosocomial infections. Mortality was especially high among patients with respiratory infections and bloodstream infections. Further analysis showed significantly higher mortality among patients over 50 years of age. A comparison between COVID-19 and non-COVID-19 patients revealed a higher incidence of infections and greater absolute mortality in the SARS-CoV-2 group, likely due to complications from viral pneumonia (Table 1).
In terms of management, empirical antibiotic therapy was initiated in most cases, followed by targeted therapy based on microbiological results. In the most complex MDR infection cases (28.9%), infectious disease consultations were requested, fostering a multidisciplinary approach. The implementation of antimicrobial stewardship programs and the use of biomarkers such as procalcitonin proved potentially useful tools to optimize diagnosis and therapy.
The study confirmed the impact of HAIs on the outcomes of ECMO patients and emphasized the importance of preventive strategies, such as the adoption of strict management protocols and early identification of infections. Among the limitations were the retrospective design and the small sample size. Future prospective multicenter studies will be essential to further validate the findings and improve the management of these critically ill patients.
Consent
Informed consent was obtained for the publication of this scientific article.
Table 1 (abstract A93). ECMO outcomesA94 Providencia stuartii infection in a critically ill patient: a case reportI. Maruzzella, P.F. Marsilia, F. Cirillo, G. Liguori, F. Imparato, M. Grazia, F. Di Biase, F. ImperatoreUOC Rianimazione DEA - AORN Cardarelli, Napoli, Italy Correspondence: I. MaruzzellaJournal of Anesthesia, Analgesia and Critical Care 2025,5(1):A94
Background
Providencia stuartii is a Gram-negative bacillus of the Enterobacterales order, often associated with healthcare-related infections, particularly in immunocompromised or critically ill patients [1]. It shows intrinsic resistance to several <beta>-lactam antibiotics and frequently acquires extended-spectrum <beta>-lactamases (ESBL) or carbapenemases, significantly narrowing therapeutic options. Strains resistant to all commonly used antibiotics, including carbapenems, have been reported, posing a serious clinical challenge [1]. In this context, the combination of aztreonam and ceftazidime/avibactam has shown promising
Results against MDR Gram-negative bacteria [2,3].
Case Report
A 32-year-old woman was admitted to the ICU with suspected autoimmune encephalitis, later confirmed by the presence of anti-NMDAR antibodies and linked to an ovarian dermoid cyst, which required surgical removal due to its unresponsivenesss to immunotherapy. During her ICU stay, the patient developed several infectious complications, including ventilator-associated pneumonia (VAP) from MDR Pseudomonas aeruginosa and C. Parapsilosis candidemia. The clinical course was further complicated by pulmonary embolism and right-sided infarction, followed by the development of empyema in the middle and lower right lobes, requiring bilobectomy. Due to a post-surgical bronchopleural fistula and recurrent empyema, she underwent open window thoracostomy with resection of the sixth and seventh ribs and later required a complete pneumonectomy.
Given the onset of septic shock, rapid and coordinated intervention was critical. Targeted antibiotic therapy and source control were implemented to stabilize her condition.
Serial microbiological cultures of the pleural cavity revealed persistent P. stuartii resistant to all tested antibiotics, including carbapenems, aminoglycosides, and fluoroquinolones. A 14-day course of cefiderocol had previously failed to achieve microbiological eradication and was discontinued in accordance with national regulatory guidelines (AIFA).
With no remaining active options, combination therapy with aztreonam and ceftazidime/avibactam was initiated [2,3]. Clinical status progressively improved, with resolution of septic shock, reduction in inflammatory markers, and progressive healing of the surgical site. Serial cultures confirmed complete sterilization of the pleural cavity within 20 days of starting combination therapy. No relapse or recurrence was observed. (Fig. 1)
Conclusions
This case highlights the life-saving potential of the aztreonam-ceftazidime/avibactam combination therapy for the treatment of pan-resistant P. stuartii infections. In an era of growing antimicrobial resistance, this combination may represent a key option against MDR Gram-negative pathogens [2,3]. Early identification and antimicrobial susceptibility testing remain essential for guiding therapy. Furthermore, the timely initiation of appropriate antibiotic therapy, alongside adequate surgical source control, played a pivotal role in stabilizing the patient's condition, optimizing the timing and conditions for surgical intervention, and ultimately overcoming septic shock.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report.
References
1.Emeraud C et al. Providencia stuartii infection in critically ill patients: case series and literature review. Infect Dis Now. 2021;51(1):37–42. https://doi.org/10.1016/j.idnow.2020.08.006
2.Rossolini GM et al. In vitro activity of aztreonam-avibactam vs MBL-producing Enterobacterales: ATLAS 2016–2020. J Glob Antimicrob Resist. 2024;36:123–31. https://doi.org/10.1016/j.jgar.2023.12.027
3.Castanheira M et al. Aztreonam-avibactam vs resistant Enterobacterales from Europe, Latin America, Asia- Pacific (2020–2022). Int J Antimicrob Agents. 2024;63(1):106803. https://doi.org/10.1016/j.ijantimicag.2023.106803
Fig. 1 (abstract A94).
Antimicrobial susceptibility profile of the isolated pan-resistant Providencia stuartii
A95 Extracorporeal blood purification therapies in pediatric septic shock: a case report on sequential therapies with ha60 and toraymyxin 05r in combination with CRRT and ECMOM.M. Paoletti1, M. Luciani2, M. Marano3, F. Stoppa3, M. Di Nardo3, S. Perdichizzi3, G. Bottari3, C. Cecchetti3 1Università di Pisa, Italy; 2Università di Bologna, Italy; 3Ospedale pediatrico Bambino Gesù, Roma, Italy Correspondence: M.M. PaolettiJournal of Anesthesia, Analgesia and Critical Care 2025,5(1):A95
Septic shock and multiple organ failure remain a leading cause of pediatric mortality worldwide. Pediatric patients affected by severe septic shock, in particular those who received extracorporeal therapies such as extracorporeal membrane oxygenation (ECMO) and renal replacement therapy (RRT), still present a high mortality rate.
Extracorporeal Blood Purification (EBP) strategies may be considered in sequence or as separate entities according to the pathophysiological status. Haemoadsorption systems can be added for the treatment of patients with early-stage sepsis and can be coupled with organ support provided by haemofiltration, ECMO, CRRT or other techniques. At present the availability of blood purification devices customized for newborn and small children is limited.
Among devices adapted for pediatric use, the HA60 Jafron cartridge incorporates a highly adsorptive resin composed of double cross-linked styrene-divinylbenzene copolymers, with a priming volume of 65±20 ml. Its relatively low volume renders it advantageous for integration into pediatric extracorporeal circuits.
Another device utilized in children is Toraymyxin cartridge, which employs polystyrene fibers covalently immobilized with polymyxin B. It is specifically designed for the selective removal of circulating endotoxins in the context of gram-negative sepsis and septic shock.
We describe for the first time to the best of our knowledge a clinical experience in using HA60 and Toraymyxin 05R in combination with CRRT and ECMO in a Gram negative fulminant septic shock.
Materials and Methods
The patient was a 3-month-old male infant with a diagnosis of posterior urethral valves and anorectal malformation. He had two previous hospitalizations for urosepsis episodes after birth. Following endoscopic laser ablation of the urethral valves, he was transferred to our center overnight in septic shock due to Gram-negative infection, presenting with refractory hypotension, hyperlactatemia, and anuria. The patient was treated with a combination of ceftazidime-avibactam and cefiderocol, along with intravenous immunoglobulin therapy and hydrocortisone. Despite aggressive management—including high-dose vasopressor support, continuous renal replacement therapy (CRRT), and extracorporeal membrane oxygenation (ECMO)—the patient exhibited a clinical deterioration marked by an increase in serum lactate, worsening metabolic acidosis, persistence of elevated inflammatory markers, and progressive increase of hepatic enzyme levels. Sequential Hemoadsorption therapy was performed using HA60 cartridges and two cycles of Toraymyxin (Fig 1).
Baseline concentrations of Presepsin, C-Reactive Protein, and Procalcitonin were 2299 pg/ml, 17.46 mg/ml, and 116 ng/ml, respectively. Following EBP treatment, these levels changed to 2944 pg/ml, 12.82 mg/ml, and 12.4 ng/ml, respectively.
Over the course of three days, the patient’s condition continued to decline, and despite maximal supportive care, the patient died.
Discussion and Conclusions:
Even though the outcome was fatal, this case report aims to demonstrate the feasibility of using multiple hemoadsorbent cartridges in combination with CRRT and ECMO. While the patient ultimately succumbed to multiorgan failure, the therapeutic approach—featuring sequential hemoperfusion with HA60 cartridges and Toraymyxin highlights the potential role of advanced extracorporeal therapies in the management of severe septic shock.
Importantly, this case also emphasizes the critical role of timing, particularly in the initiation of hemoadsorption therapy. Early intervention may be a key factor in maximizing the potential benefits.
Consent
Informed consent was obtained for the publication of this scientific article.
Fig. 1 (abstract A95). A96 Antimicrobial resistance and the challenges of antibiotic prescription: an antimicrobial stewardship-based approachA. Usai1, F. Utzeri2, F. Vacca2, S. Paba1, E. Lai1, A. Orrù1, A. Busia1, F.M. Loddo1
1Dipartimento Attività Cliniche - Ospedale NS della Mercede - SC Anestesia e Rianimazione - ASL Ogliastra, Lanusei, Italy; 2Dipartimento Area Servizi - Ospedale NS della Mercede - SSD Farmacia Ospedaliera - ASL Ogliastra, Lanusei, Italy
Correspondence: A. Usai
A96 Antimicrobial resistance and the challenges of antibiotic prescription: an antimicrobial stewardship-based approachA. Usai1, F. Utzeri2, F. Vacca2, S. Paba1, E. Lai1, A. Orrù1, A. Busia1, F.M. Loddo1
1Dipartimento Attività Cliniche - Ospedale NS della Mercede - SC Anestesia e Rianimazione - ASL Ogliastra, Lanusei, Italy; 2Dipartimento Area Servizi - Ospedale NS della Mercede - SSD Farmacia Ospedaliera - ASL Ogliastra, Lanusei, Italy
Correspondence: A. UsaiJournal of Anesthesia, Analgesia and Critical Care 2025,5(1):A96
Background
In the European Union, healthcare-associated infections (HAIs) account for approximately 71% of infections caused by antibiotic-resistant bacteria, including carbapenem-resistant Enterobacterales. The implementation of robust infection prevention and control (IPC) measures is essential, particularly in intensive care units (ICUs), where patients are at increased risk of acquiring multidrug-resistant infections [1]. Antimicrobial stewardship (AMS) encompasses coordinated strategies aimed at optimizing antimicrobial use to mitigate the development and spread of antimicrobial resistance (AMR) [2]. Effective AMS programs are founded on continuous surveillance of antimicrobial consumption and resistance patterns, supported by interdisciplinary collaboration among clinicians, microbiologists, pharmacists, and infection control specialists [3].
Materials and Methods
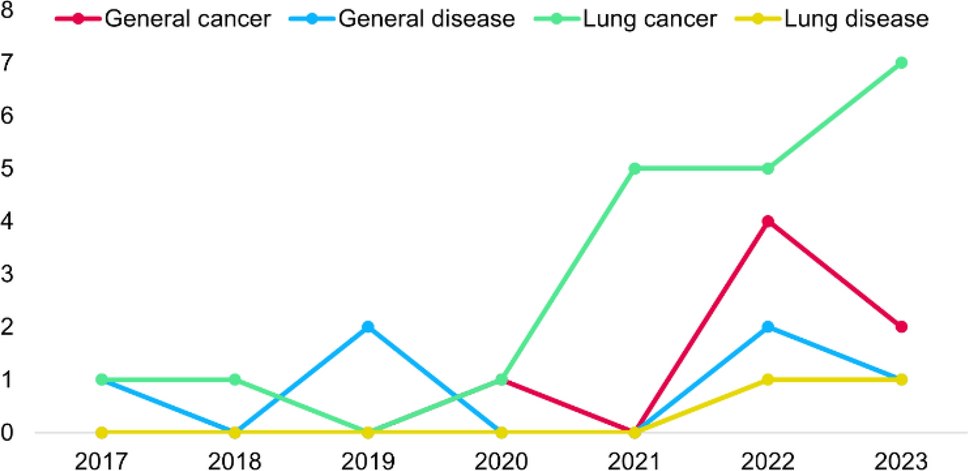
A retrospective analysis was conducted on AMR patterns and antimicrobial consumption in an ICU from January 2018 to December 2023. Data was retrieved from dedicated surveillance software. The analysis focused on infections including lower respiratory tract infections (LRTIs), catheter-related bloodstream infections (CR-BSIs), and catheter-associated urinary tract infections (CA-UTIs). Antimicrobial usage over the same period was also assessed.
Results
During the study period, susceptibility trends in LRTIs demonstrated a notable decline in response to cefepime, piperacillin-tazobactam, fluoroquinolones, and meropenem. Conversely, the susceptibility to linezolid and vancomycin remained stable at 75% and 80%, respectively. CR-BSI data revealed a significant reduction in vancomycin susceptibility (33%). In CA-UTIs, susceptibility rates were consistently low for piperacillin-tazobactam, meropenem, linezolid, and vancomycin, whereas ciprofloxacin susceptibility significantly improved, reaching 60%. Antimicrobial consumption analysis indicated a reduction in ceftriaxone and ciprofloxacin use, paralleled by an increase in the administration of levofloxacin, meropenem, vancomycin, and
Comments (0)