
Remember me
A total of 165 consecutive patients were included in the study. Seventy-one patients received ATLG-15, and 94 Patients received ATLG-30. The median year of transplant was 2020 (2018–2022) in the ATLG-15 group and 2018 (2011–2022) in the ATLG-30 group (p < 0.001). The median age at transplant was 57 years (range, 20–72) and 58 years (range, 20–71) in the ATLG-15 and ATLG-30 (p = 0.88) groups, respectively. ECOG performance status scores were higher in the ATLG-15 group (ECOG0 18%, ECOG1 72%, ECOG2 9%) compared to the ATLG-30 group (ECOG0 36%, ECOG1 64%) (p = 0.001). Sixty eight percent received MAC in the ATLG-15 group compared to 48% in the ATLG-30 group (p = 0.01). All patients, donors, and transplant characteristics are listed in Table 1.
Table 1 Patients Donors and Transplants characteristics.Transplant outcomesAll univariate analysis for transplant outcomes are summarized in Table 2.
Table 2 Univariate analysis.EngraftmentOne patient died prior to engraftment and three patients had primary graft failure in the ATLG-15 group, all remaining patients successfully engrafted. The ATLG-15 cohort showed an earlier leukocyte engraftment (median 11 days, range 8–19, p = 0.004) and earlier platelet engraftment (median 12 days, range 8–107, p = 0.0002) compared to the other group’s medians of 12 days (range 8–16) and 15 days (range 3–249), respectively.
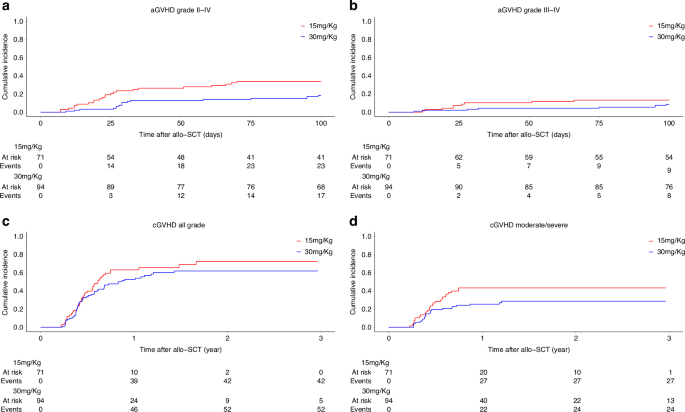
GVHDThe cumulative incidence of aGVHD grade II-IV at day 100 was comparable between the two groups (ATLG-15: 34% vs ATLG-30: 18%, p = 0.2) (Fig. 1a). Only patients’ CMV serology significantly affected aGVHD II-IV, with a cumulative incidence of 12% in patients with negative serology compared to 33% in those with positive serology on univariate analysis (p = 0.007). This difference persisted on MVA (HR: 2.40 [95% CI: 1.30–4.43], p = 0.005). Additionally, there was a trend for increased risk of aGVHD II-IV in patients transplanted from female donors versus male donors (HR: 1.75 [95% CI: 0.96, 3.18], p = 0.068).
Fig. 1: Graft versus host disease.
ATLG 15 mg/Kg vs 30 mg/Kg. a aGVHD grade II-IV. b aGVHD grade III-IV. c cGVHD all grade. d cGVHD moderate/Severe.
The cumulative incidence of aGVHD Grade III-IV at day 100 was comparable between the ATLG-15 (13%) and the ATLG-30 (9%) groups (p = 0.7) (Fig. 1b). Conversely, only conditioning intensity significantly affected aGVHD Grade III-IV, with a cumulative incidence of 4% in patients who received MAC and 19% in those who received RIC (p = 0.0006). This difference persisted on MVA (HR: 5.89 [95% CI: 1.71–20.26], p = 0.0049).
We observed no differences in the cumulative incidence of all grade cGVHD between the two groups, with a cumulative incidence at 2 years of 73% versus 62% in the ATLG-15 and ATLG-30 groups, respectively (p = 0.21) (Fig. 1c). On MVA, none of the factors affected all grade cGVHD.
Patients in the ATLG-15 group had a significantly higher cumulative incidence of moderate/severe cGVHD compared to patients in the ATLG-30 group (ATLG-15: 43% vs ATLG-30: 28%, p = 0.045) (Fig. 1d). No other factor significantly affected cGVHD. This difference persisted on MVA (HR: 0.450 [95% CI: 0.214, 0.946], p = 0.035). MVA for GVHD are summarized in Table 3.
Table 3 Multivariate analysis graft versus host disease, non relapse mortality and cumulative incidence of relapse.OS and PFSThe estimated 2-year OS was 72% for patients in the ATLG-15 group and 77% in the ATLG-30 group (p = 0.2) (Fig. 2a). The estimated 2-year PFS was 60% for patients in the ATLG-15 group and 65% in the ATLG-30 group (p = 0.4) (Fig. 2b). On univariate analysis older patients, TBI, higher DRSS and progressive disease at transplant were associated with lower OS and PFS. There was a trend for lower OS for patients with higher ECOG performance status and lower PFS for patients with negative CMV serology. No other factor affected OS or PFS on univariate analysis. In MVA, older age (HR 1.04 [95%CI: 1.01–1.08], p = 0.02) and Very High DRSS risk vs. Standard (HR 6.70 [95%CI: 1.45–30.98], p = 0.01) were significantly associated with inferior OS. (Fig. 2c) For PFS, older age (HR 1.03 [95%CI: 1.00–1.06], p = 0.03) and Very High DRSS risk vs. Standard (HR 4.27 [95%CI: 1.37–13.31], p = 0.01) were also significantly associated with worse outcomes. (Fig. 2d)
Fig. 2: Overall survival and progression free survival ATLG 15 mg/Kg vs 30 mg/Kg.
a OS. b PFS. cMultivariate analysis OS. d Multivariate analysis PFS.
NRM and CIRThe 2-year cumulative incidence of NRM was comparable between the two groups, with 13% in the ATLG-15 group and 6% in the ATLG-30 group (p = 0.11) (Fig. 3a). Only patients’ age negatively impacted NRM on univariate analysis. On MVA none of the factors impacted NRM (Table 3).
Fig. 3: Non relapse mortality, cumulative incidence of relapse, graft versus host disease relapse free survival ATLG 15 mg/Kg vs 30 mg/Kg.
a Non relapse mortality. b Cumulative incidence of relapse. c GRFS. d Multivariate analysis GRFS.
The CIR at 2 years was similar between the ATLG-15 and ATLG-30 groups, with rates of 25% and 28%, respectively (p = 0.64). (Fig. 3b) However, we observed a higher CIR in patients with negative CMV serology compared to those with positive CMV serology (at 2 years: CMV neg 37% vs CMV pos 21%, p = 0.01). Patients who received total body irradiation (TBI) had a significantly higher CIR at 2 years compared to those who did not receive TBI (64% vs 24%; p = 0.005). Additionally, patients transplanted with progressive disease (PD) exhibited a higher CIR at 2 years (PD: 55%) compared to those in complete remission (CR: 22%), partial remission (PR: 21%), or untreated (17%) (p = 0.004). The cumulative incidence of relapse was highest in the Very High DRSS group at 60 [95%CI: 37–77], compared to 16 [95%CI: 4–36] in Standard, 14 [95%CI: 6–26] in Intermediate 1, 21 [95%CI: 12–32] in Intermediate 2, and 15 [95%CI: 4–34] in the High-risk group (p < 0.001). No other factors significantly impacted CIR in the univariate analysis. In MVA, Very High DRSS risk vs. Standard (HR 3.37 [95%CI: 1.10–10.31], p = 0.03) and TBI vs. no TBI (HR 2.51 [95%CI: 1.04–6.04], p = 0.04) were significantly associated with increased relapse risk.
GRFSThe GRFS at 2 years was comparable between the ATLG-15 and ATLG-30 groups, with rates of 24% and 36%, respectively (p = 0.1) (Fig. 3c). On univariate analysis, patient age (at 2 years: age ≤58 years 36% vs > 58 years 24%, p = 0.02) and RIC (at 2 years: MAC 37% vs RIC 22%, p = 0.02) negatively impacted GRFS. GRFS was markedly lower in the very high DRSS group at 2 yrs 5% [95%CI: 1–33], compared to 39% [95%CI: 21–76] in Standard, 40% [95%CI: 26–61] in Intermediate 1, 30% [95%CI: 19–47] in Intermediate 2, and 43 [95%CI: 26–72] in the High-risk group (p = 0.005).
In MVA, older age (HR 1.02 [95%CI: 1.00–1.04], p = 0.04) was significantly associated with inferior GRFS, while ATLG-30 vs. ATLG-15 was associated with improved GRFS (HR 0.47 [95%CI: 0.25–0.88], p = 0.02). Additionally, there was a trend toward inferior GRFS in patients receiving RIC compared to MAC (HR 1.60 [95%CI: 0.98–2.63], p = 0.06), and in those with Very High DRSS risk vs. Standard (HR 2.08 [95%CI: 0.93–4.68], p = 0.08). (Fig. 3d)
Propensity score matchingPropensity score matching yielded 19 matched cases and 31 matched controls. Covariate balance improved substantially after matching, with standardized mean differences for most variables falling well below 0.2. The variance ratio for the propensity scores was close to 1 (1.16), indicating strong balance between groups. Visual assessment using a Love plot and a density plot confirmed the reduction in imbalance across covariates (Supplementary Fig. 1A, B). In competing risk analysis, the 2-year cumulative incidence of non-relapse mortality was 30% in the ATLG-15 group and 0% in the ATLG-30 group. Due to the absence of NRM events in the ATLG-30 group, the sub distribution hazard could not be reliably estimated using Fine-Gray regression. No significant differences were observed in OS, PFS, CIR GRFS, aGVHD Grade II-IV, aGVHD III-IV, cGVHD all grade and moderate/severe. All results are summarized in Supplementary Table 1
Subgroup analysis of AML/MDS Patients who did not receive TBI by conditioning intensityAmong AML/MDS patients who did not receive TBI (n = 108), 61 received ATLG 15 mg/kg and 47 received ATLG 30 mg/kg. In the MAC subgroup (n = 69), 38 received 15 mg/kg and 31 received 30 mg/kg. In the RIC subgroup (n = 39), 23 received 15 mg/kg and 16 received 30 mg/kg.
In the overall AML/MDS no-TBI population, the incidence of moderate-to-severe cGVHD was significantly higher with ATLG 15 mg/kg compared to 30 mg/kg (38% vs. 19%, p = 0.039). In the MAC subgroup, moderate-to-severe cGVHD occurred more frequently with ATLG 15 mg/kg (39% vs. 19%, p = 0.079). In the RIC subgroup, no statistically significant differences were observed between ATLG 15 mg/kg and 30 mg/kg for any outcomes.
All results are summarized in Supplementary Table 2.
Comments (0)