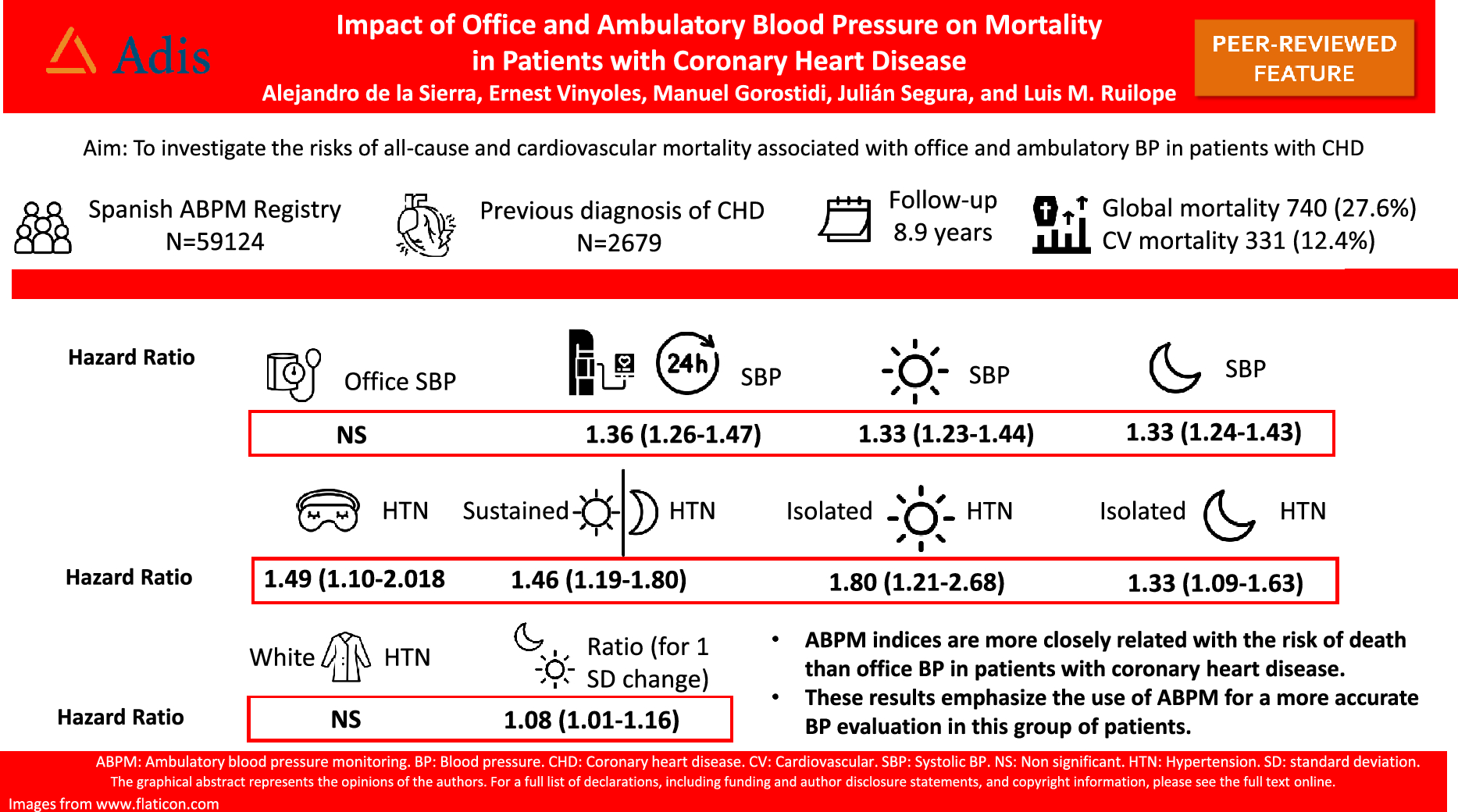
The present study demonstrate that ABPM-derived indices are superior to office BP in predicting all-cause and cardiovascular mortality in patients with documented coronary heart disease. Twenty-four-hour, daytime and nighttime SBP were all significantly associated with all-cause and cardiovascular mortality in models adjusted for clinical confounders and office SBP. The superior impact of ABPM on mortality was also observed by the analysis of BP phenotypes, with increased rates of mortality in subgroups with masked and sustained hypertension, while white-coat hypertension was not significantly associated with an increased risk. In relation to BP variability, NDR was significantly associated with mortality as it was the presence of a riser pattern (nocturnal BP higher than daytime BP). These results are in accordance with previous reports in the general population of patients with hypertension and emphasize the use of ABPM in patients with CHD, in order to better assess the BP-related risk in this population.
Although ABPM is considered the best accurate method for BP measurement [23], and its role in hypertension diagnosis and management has been extensively investigated [3,4,5,6,7,8,9,10,11,12,13], studies evaluating its role in patients with CHD are scarce, mostly cross-sectional, or with a limited sample size [14]. First prospective studies [15, 24] use Holter identified transient ischemic episodes as outcome while later reports examined the risk of new myocardial infarction [17], restenosis [25], or a composite endpoint of fatal and non-fatal events [16, 26]. In most cases, sample sizes have been small (< 100 patients) and results included a positive relationship with 24-h, daytime, and nighttime BP elevation, as well as with a non-dipping pattern.
Our results demonstrate the superiority of ABPM-derived BP indices over office BP in the prognosis of patients with CHD. Although both systolic office and ABPM were associated with the risk of death in unadjusted models, after clinical confounders adjustments, office BP was no longer predictive, whilst 24-h, daytime and nighttime SBP significantly associated with all-cause and cardiovascular mortality, and this association was not modified by office SBP adjustment. These results are similar as other previously reported in the general population of patients with hypertension [5], or in patients with hypertension and diabetes [27] or with a previous stroke [28]. It is noteworthy that hazard ratios for both daytime and nighttime SBP were similar and after simultaneous adjustment both indices maintained their association with all-cause and cardiovascular death. Although it has been clearly demonstrated that nighttime BP has a superior prognostic accuracy in relation to both cardiovascular events development and mortality in the general population of patients with hypertension [4, 5], as well as in patients with hypertension and a previous stroke [28], the present results suggest that in patients with CHD both ABPM-derived indices have similar importance in their association with the risk of death.
In the same direction, when patients were separated in groups of isolated daytime or nighttime hypertension, or combined daytime and nighttime hypertension, all the obtained phenotypes have a significant association with all-cause mortality, when compared to patients with normal daytime and nighttime BP (the reference group), also indicating that both daytime and nighttime BP are important in their association with mortality. For cardiovascular mortality, hazard ratios had similar values than for all-cause mortality. However, confidence intervals were wider, lacking statistical significance, possibly due to the low number of cardiovascular deaths in each of these groups. These observations have possible implications indicating that both daytime and nighttime BP should be equally targeted with antihypertensive treatment in patients with CHD.
The analysis of BP phenotypes of white-coat, masked, and sustained hypertension revealed that only sustained and masked hypertension were associated with mortality, while white-coat hypertension was not. These results are aligned with those we have previously reported in the general population of patients with hypertension, also showing a lack of association between white-coat hypertension and risk of mortality [5]. Although this has been controversial in other reports, this is possibly related to the way white-coat hypertension is defined, regarding normal 24-h or normal daytime BP [8]. In the case of masked hypertension, the association was statistically significant with all-cause mortality, but not with cardiovascular mortality. As also commented before, we interpret that the lack of statistical significance is also influenced by the low number of deaths (masked hypertension is the phenotype with the lowest number of patients) and the resulting wide confidence interval.
We have examined the association between BP variability and mortality in this group of patients. Night-to-day ratio, both systolic and diastolic was associated with all cause mortality in models adjusted for clinical confounders and additionally for 24-h BP. Regarding nocturnal phenotypes, only the riser pattern based on diastolic BP was associated with the risk of death. In the case of cardiovascular mortality neither NDR nor any phenotype was associated with an increased risk. Previous observational studies have focused on these nocturnal phenotypes and the risk of cardiovascular events in patients with CHD, with some inconsistent results. While some found increased risk of Holter-identified transient ischemic episodes [15, 24] in non-dippers (combining non dippers and risers in the same group), a more recent report [26] concluded that the impact of a riser pattern was lost when adjusted for absolute values of nocturnal BP. In the general population of patients with hypertension, we have reported that non-dipping was associated with all-cause and cardiovascular death, even in the absence of nocturnal BP elevation. However, nocturnal BP was a more powerful estimate than non-dipping [11]. It is acknowledged that these nocturnal BP phenotypes have a limited reproducibility, and are significantly influenced by the interference of the ABPM procedure with the quality of sleep [3].
The association of other short-term variability parameters, such as SD or ARV with the risk of death was mild and, in most cases became non-significant after adjustment for absolute BP values. Only nighttime systolic BP-SD remained significant but with only a moderate association (9% increase in total mortality for 1 SD change). Whereas we and others have previously reported an association between short-term BP variability and prognosis in patients with hypertension, in all cases such associations were mild compared with the risk driven by absolute BP elevation [13, 29]. In the present report in patients with CHD, short-term BP variability did not seem to provide a significant prognostic effect added to that of absolute BP elevation.
The present study has important limitations. First, the history of CHD was based on the clinical record, limited to a previous diagnosis of an acute coronary event or stable angina. We do not have more information regarding clinical characteristics of the event, type of coronary lesions or revascularization treatments. Second, patients included in the Registry were those with an indication for ABPM, based on guidelines, and it does not necessarily represent the general population of people with CHD. Third, data regarding antihypertensive treatment was available only at baseline, whilst changes done during follow-up were not collected, and fourth, the observational nature of the study precludes any direct inference on the possible benefit of basing treatment on ambulatory BP measurements. Nevertheless, the present study has several strengths, as represents the largest cohort of patients with CHD and ABPM, as well as the long duration of follow-up.



Comments (0)