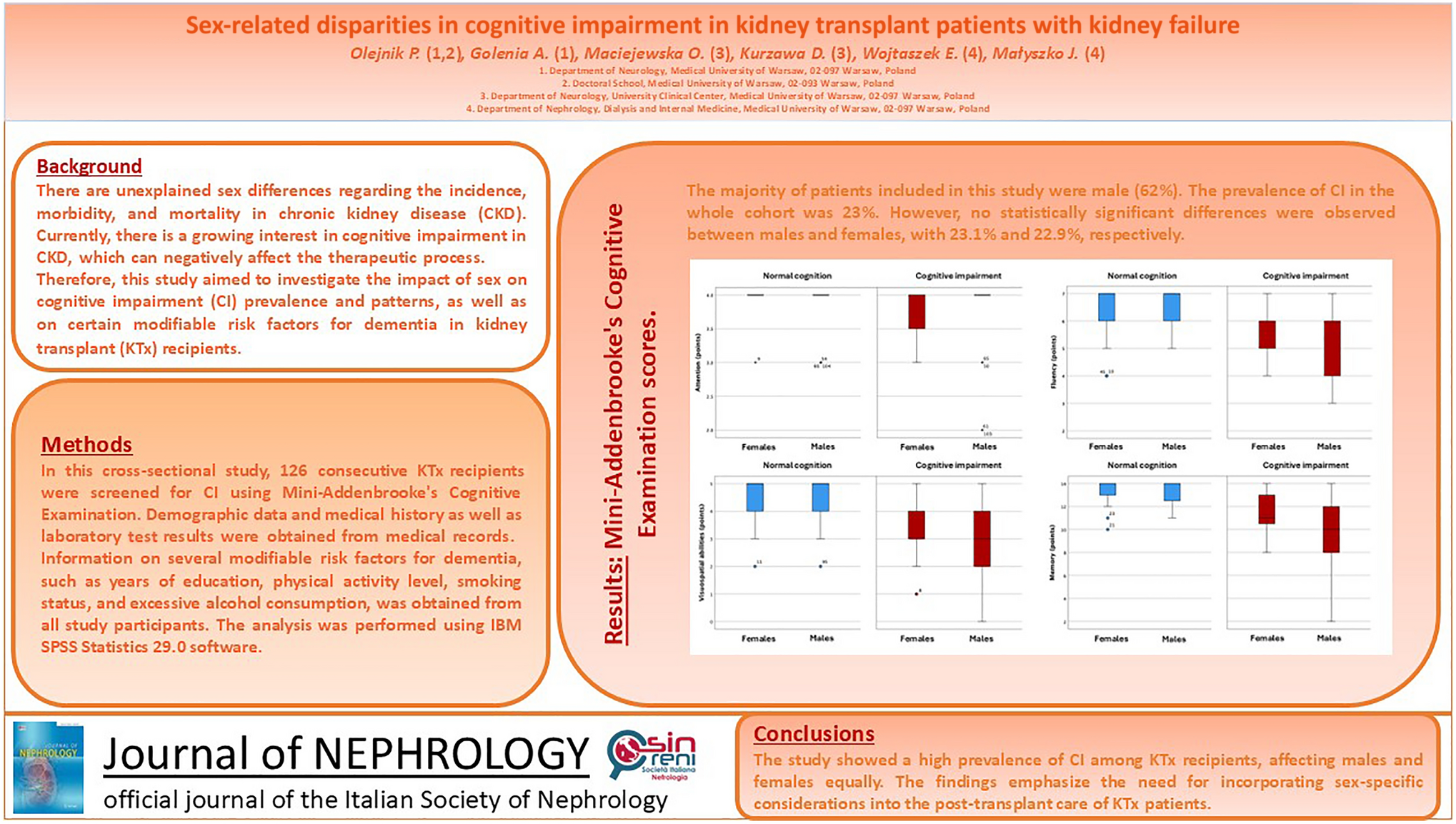
In this study, to the best of our knowledge for the first time in the literature, we investigated sex-based differences in cognitive impairment among transplant recipients. Overall, cognitive impairment affected 23% of the 126 study participants, with no significant sex-related difference in prevalence.
The reported prevalence of cognitive impairment among KTx recipients varies considerably across studies, ranging from 15.6% to 58% [8, 16], and remains higher than in the general population, even among younger recipients [16]. However, direct comparisons across studies are limited by substantial heterogeneity in cognitive screening instruments and methodological approaches, including the absence of established cut-off points and the lack of a healthy control group.
Based on assessments conducted prior to kidney transplantation and at 3 months and one year post-transplant, Gupta et al. demonstrated that kidney failure-related cognitive impairment may be partially reversible [17]. Their findings show that episodic and verbal declarative memory, as measured by Logical Memory I and II, returned to normative levels. However, semantic memory, verbal fluency, and language, as assessed by Category Fluency tasks for animal and vegetable naming, as well as psychomotor speed and visuospatial function, as measured by the Digit Symbol Substitution Test, showed only partial improvement. Although Mini-Mental State Examination scores improved slightly, they did not reach normative values [17]. Similarly, Binari et al. have reported improvements in attention and executive function, measured by the Trail Making Test, despite no significant changes in global cognition assessed with the Repeatable Battery for the Assessment of Neuropsychological Status [18]. Finally, studies evaluating cognitive performance in waitlisted patients with kidney failure have reported a high prevalence of cognitive impairment, affecting up to 30% of this population [19].
Thus, CKD is increasingly recognized as a risk factor for cognitive impairment, with vascular dementia representing the predominant underlying cause. However, the mechanisms involved are complex and poorly understood [6, 20]. Patients with CKD, particularly those with kidney failure, present with numerous cardiovascular risk factors commonly associated with vascular dementia pathogenesis, such as atherosclerosis, hypertension, atrial fibrillation, and diabetes mellitus. They are also exposed to CKD-specific factors, including uremic toxicity and chronic inflammation [20]. Furthermore, kidney transplant recipients who are treated with calcineurin inhibitors, such as tacrolimus or cyclosporine, may develop endothelial dysfunction and vasoconstriction, leading to reduced cerebral blood flow and subsequent cognitive impairment [6].
Assuming that vascular dementia is the main cause of kidney failure-related cognitive impairment, our findings support the concept that its overall prevalence does not differ significantly by sex [21, 22]. For instance, in a pooled analysis of four population-based studies involving individuals aged 65 years and older, Andersen et al. found that females over the age of 85 were at a higher risk of developing Alzheimer’s disease than males. However, no sex-related differences were observed in vascular dementia risk [21]. These results are further supported by an epidemiological study from the United Kingdom conducted by Imfeld et al., which demonstrated that vascular dementia affects males and females at comparable rates [22].
Moreover, our study population has a male predominance, which aligns with the common observation that females are less often referred and waitlisted for KTx, and less likely to receive a kidney transplant compared to males [23]. For instance, a national cohort study by Segev et al., involving 563,197 patients newly diagnosed with kidney failure between 2000 and 2005, found that females with comorbidities had lower access to KTx than males with the same conditions, despite similar survival benefits [24]. One potential explanation is that adult males are 50% more likely to develop kidney failure, despite the fact that CKD prevalence is higher in females [25]. Interestingly, a systematic review by Vilayur et al. revealed that females are more likely to serve as living donors, with female predominance observed in 83% of the studies [26]. Socioeconomic and emotional factors are among the most frequently mentioned explanations for sex disparities in living kidney donation. For instance, concerns about losing a primary source of income may discourage males from donating, while altruism may motivate females [26].
Additionally, although creatinine clearance rates were comparable for both sexes, in our study males had significantly higher creatinine levels than females. This finding is consistent with previous studies that emphasize the advantages of cystatin C as a marker of kidney function, particularly in individuals with greater muscle mass [27]. Furthermore, males in our study had significantly higher serum urea and uric acid levels compared to females, possibly because of the influence of sex hormones [28]. Wang and Charchar reported that circulating uric acid levels in adolescent boys were positively associated with higher testosterone levels and negatively associated with sex hormone-binding globulin concentrations [28]. Moreover, Liu et al. demonstrated blood urea nitrogen levels to be significantly higher in males than in females, regardless of age, which is consistent with our findings [29]. These results may be partially attributed to the lower muscle protein synthesis rates observed in males compared to females, as demonstrated by Henderson et al., this could result in increased protein breakdown and nitrogenous waste production [30].
This study has several limitations that should be acknowledged. First, the cross-sectional design prevents the establishment of causal relationships. Moreover, the small sample size, particularly in the female cohort, might have limited the statistical power to detect subtle differences. Furthermore, cognitive functions were assessed using the MACE rather than a comprehensive neuropsychological battery, which may limit diagnostic accuracy in the case of mild cognitive deficits [31]. Also, since some modifiable risk factors were self-reported by patients, recall bias may have compromised the accuracy of the collected data. Finally, the absence of a pre-transplant cognitive assessment hindered our ability to determine whether cognitive impairment developed de novo post-KTx or existed prior to transplantation. Despite these limitations, the study’s primary strength is in its novel focus on sex-related cognitive outcomes in kidney transplant recipients – an area that, to the best of our knowledge, has not yet been investigated.

Comments (0)