This study provided epidemiologic and clinicopathologic characterization of conventional ameloblastoma over a 22-year period from a single academic surgical oral pathology laboratory in the Midwestern United States (U.S.). To our knowledge, it represents the first institutional analysis from this region. A previous investigation from the Southeastern U.S. focused primarily on racial and ethnic factors [7]. In contrast, our study incorporated detailed treatment information and recurrence-free survival data, providing insight into prognostic patterns and management strategies for ameloblastoma within a U.S. population.
WHO Classification of Head and Neck Tumors (5th edition) classifies conventional ameloblastoma as a distinct entity separate from unicystic and peripheral ameloblastoma [1], supporting the clinical relevance of analyzing this tumor independently. Accordingly, we focused exclusively on conventional ameloblastoma, which demonstrates aggressive local behavior and a substantially greater recurrence risk than unicystic and peripheral ameloblastoma. This approach allowed clearer definition of the clinical and histologic spectrum of the biologically aggressive form of the disease.
Although all specimens were processed at a single reference laboratory, the cohort included submissions from multiple geographical location within the U.S., with nearly half originating outside the state of Iowa. This broad referral base enhances the external validity of our findings, suggesting that the observed patterns are not limited to a single regional population in the U.S. However, this diversity also introduced variability in clinical documentation, radiographic imaging, and treatment approaches, reflecting differences in practice across referring providers and institutions.
The mean patient age in our cohort was 51 years, which aligns with the commonly reported fourth to fifth decade age range for conventional ameloblastoma [1]. This mean age is slightly higher than that reported in a previous U.S.-based study, which documented a mean age of approximately 42 years [7]. A recent global epidemiologic analysis demonstrated that ameloblastoma most commonly occurs in the third decade overall but presents later in Europe and North America, typically in the fifth and sixth decades [5], supporting our findings. A slight male predominance (56.3%) was observed in our study, consistent with reports from global and North American populations, which describe male involvement ranging from 52 to 59% [1, 5].
The mandible was the predominant site of involvement in our cohort (91.9%), consistent with previous U.S. data reporting 93% mandibular involvement [7] and global estimates of 87% [5]. Although a North American systematic review and meta-analysis reported a lower proportion of mandibular cases (71%) [5], the mandible remains the most common site of occurrence across all studies. With respect to specific tumor location, involvement of the posterior mandible is most commonly reported [1]. An exception is the desmoplastic subtype, which has been reported to equally occur in both the mandible and maxilla and shows a greater predilection for the anterior jaws [8]. In our dataset, anatomic subsite information was inconsistently recorded in pathology submission forms, which limited more detailed evaluation of jaw-region involvement.
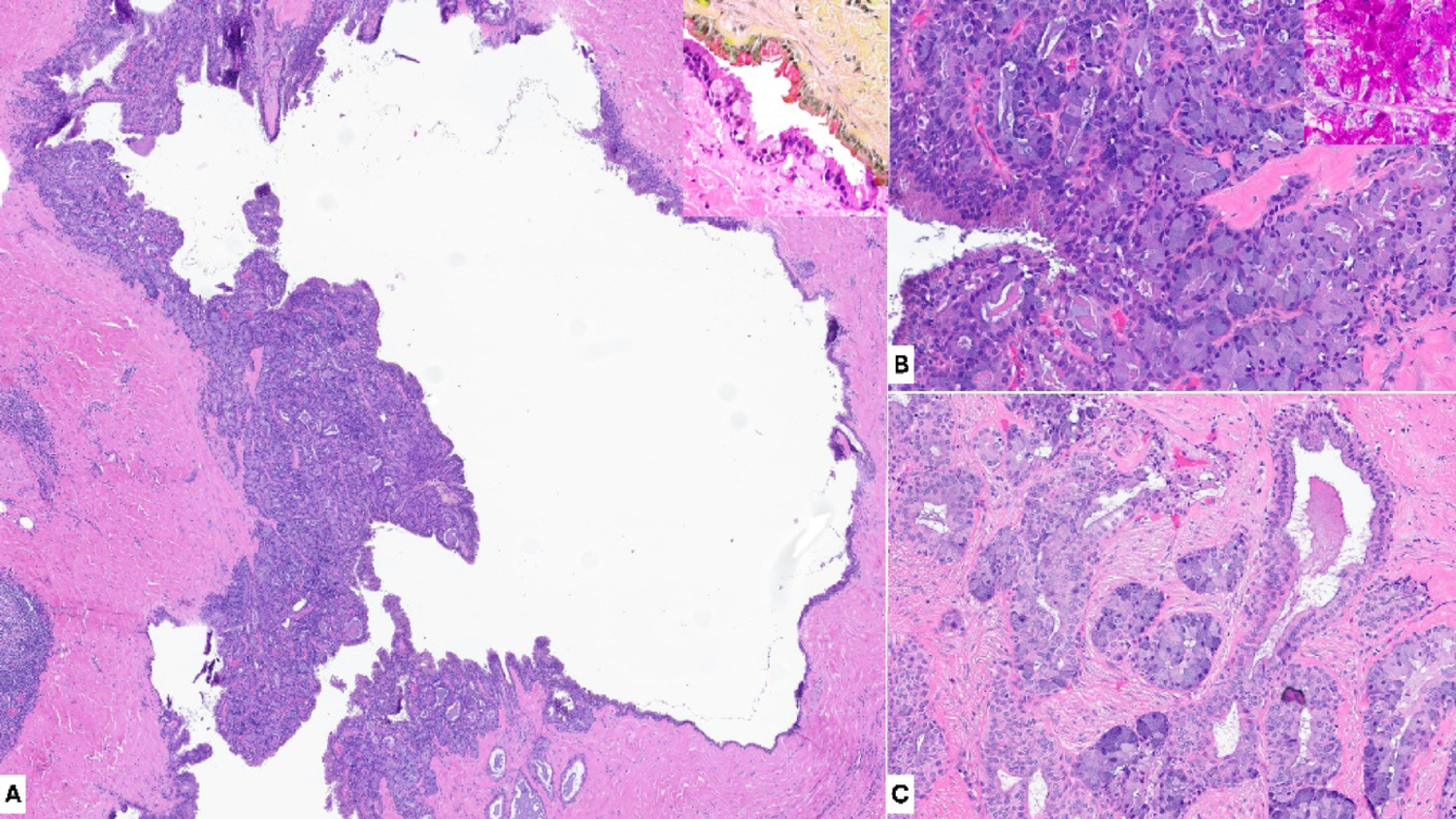
Radiographically, unilocular radiolucency was the most common presentation in our cohort (54.4%). Although multilocularity has been reported as the predominant pattern in some studies, accounting for up to 74% of cases [1, 9], a multicenter cohort study documented relatively equal frequencies of unilocular and multilocular lesions [4], reflecting variability across studies. Multilocularity was identified as a potential predictor of increased recurrence risk and more aggressive clinical behavior in some studies [10]. In contrast, Bi et al. reported no significant association between radiographic pattern and recurrence risk [11], which is consistent with our findings. Mixed radiolucent-radiopaque radiographic appearance has been described in desmoplastic subtype of conventional ameloblastoma, attributed to reactive bone formation and sclerosis of trabeculae associated with stromal desmoplasia, rather than intrinsic tumor mineralization [1, 8]. A systematic review reported that up to 54% (152 of 279 cases) of conventional ameloblastoma with pure desmoplastic morphology or in combination with other subtypes exhibited mixed radiolucent-radiopaque features [8]. In our cohort, 6 of 24 cases (25%) with desmoplastic component and available radiographic information demonstrated a mixed radiolucent-radiopaque appearance. The predominance of incisional biopsy specimens in our study limited assessment of reactive bone formation in cases demonstrating mixed radiolucent-radiopaque radiographic appearance and may account for the absence of a desmoplastic component in one such case on histologic evaluation. Importantly for radiographic results of our study, radiographic information in our study was derived solely from clinician-provided descriptions on pathology submission forms. As a result, variability in interpretive criteria, imaging modality, and completeness of reporting could not be standardized, and original imaging studies were not available for re-review. Differences between two-dimensional imaging (e.g., panoramic radiograph) and three-dimensional techniques (e.g., cone-beam computed tomograph) may also influence the perception of radiodensity and locularity. In addition, other radiographic features that have been reported to be associated with greater tumor aggressiveness and recurrence risk (e.g., association with impacted teeth, cortical perforation, and root resorption) [10, 11] were not consistently documented in our cohort, limiting further analysis.
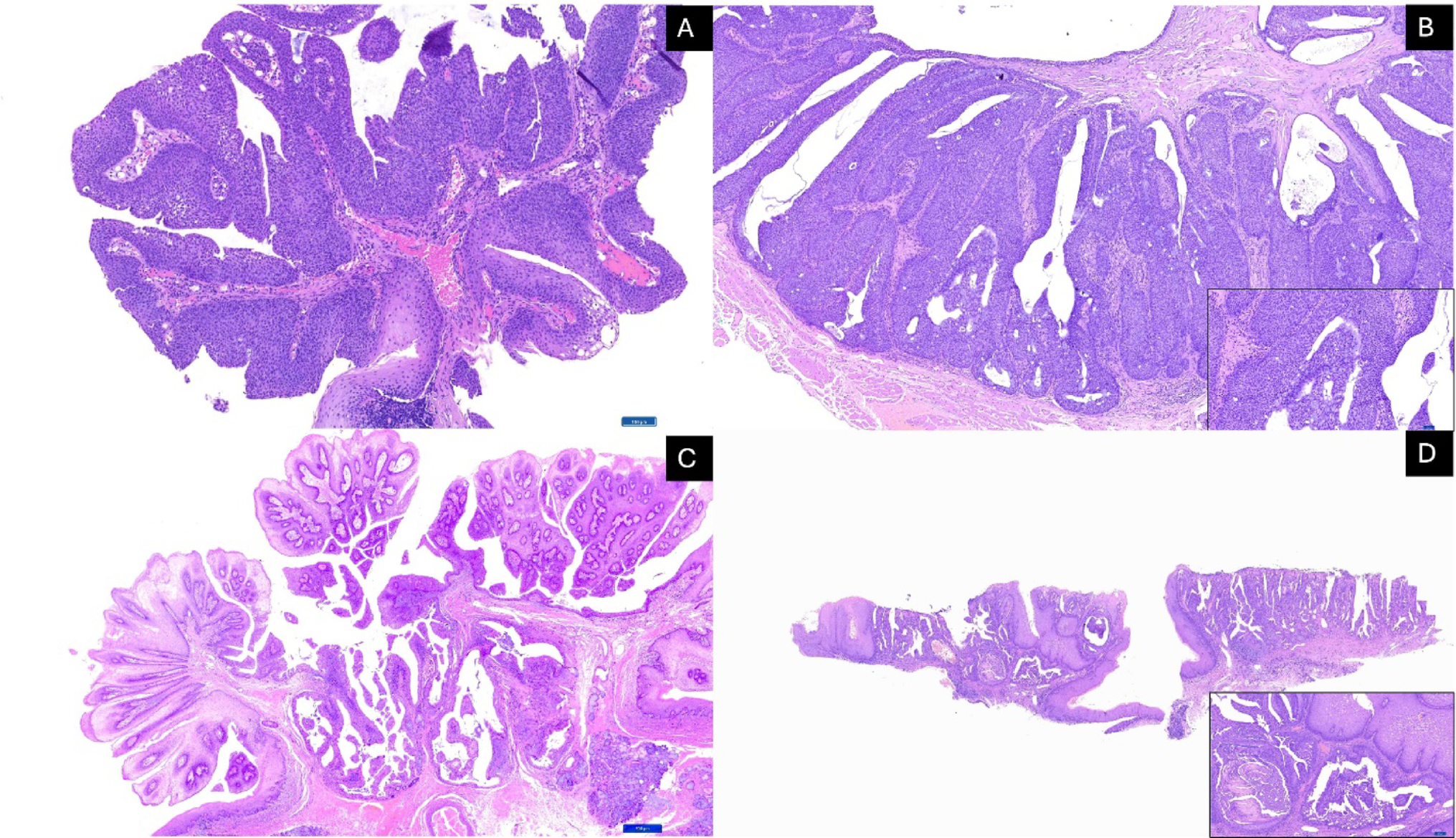
Mixed histologic patterns were frequently observed in our cohort, with a predominance of the follicular component combined with other subtypes, consistent with previous studies of ameloblastoma [1, 7]. A recent study from the Southeastern U.S. likewise demonstrated that many ameloblastoma cases exhibited more than one histologic subtype within the same lesion [7], reinforcing the marked histologic heterogeneity of conventional ameloblastoma. These findings underscore the limited prognostic value of subclassifying tumors based solely on histologic subtype. In our analysis, histopathologic subtype did not show a significant difference in recurrence-free survival. A recent scoping review evaluating factors associated with ameloblastoma recurrence exhibited substantial inconsistency across studies regarding the prognostic relevance of histologic subtypes [10]. Much of this variability likely reflects differences in how subtypes were defined across investigations and some studies did not account for tumors exhibiting multiple histologic subtypes within the same lesion [12,13,14] which is common in our cohort and in previous studies [1, 7, 15]. Furthermore, most specimens in our study were incisional biopsies, which further restrict accurate subtype characterization, as sampling may not capture the full architectural diversity of the lesion. Taken together, the overall evidence supports that histologic subtype alone is not a reliable prognostic indicator in conventional ameloblastoma.
Treatment modality was the significant predictor of recurrence outcome in our analysis. Resection demonstrated substantially improved recurrence-free survival compared with conservative procedures, consistent with previous reports showing lower recurrence rates after radical resection and markedly higher recurrence following conservative treatment [10, 11]. Recurrence occurred as late as 24 and 30 years after initial treatment in patients who were 26 and 33 years old, respectively, at the time of initial diagnosis. Such delayed recurrence likely reflects indolent regrowth of residual tumor following conservative treatment, which is more frequently selected in younger patients to preserve function and quality of life. Notably, two patients experienced recurrence after resection, and one of these developed a second recurrence approximately 23 years after repeat resection. Follow-up periods of 5 to 10 years are commonly reported in the literature [2, 16, 17]; however, our findings in these four cases suggest that long-term postoperative follow-up beyond a decade may be warranted. Recurrence following resection suggests that intrinsic biological factors may contribute to tumor persistence. Molecular alterations involving the MAPK and Hedgehog signaling pathways (particularly BRAF p.V600E and SMO variants) are commonly detected in ameloblastoma and may influence recurrence potential [18,19,20,21]. A previous study demonstrated that tumors harboring multiple mutations exhibited a higher recurrence risk compared with those containing a single alteration [22]. Such molecular heterogeneity may help explain why some tumors recur despite aggressive management.
Although younger age appeared to be associated with recurrence in the direct comparison between the two groups (Student’s t-test), this association did not persist in Cox regression analysis, indicating that age was not an independent predictor of recurrence. The significant age difference observed in the t-test likely reflects confounding by treatment modality rather than a biologic effect. Among patients who experienced recurrence, 66.7% underwent enucleation and curettage, whereas 95% of non-recurrent cases were treated with resection. Overall, this marked imbalance suggests that the apparent association between younger age and recurrence is driven by differences in surgical treatment, which is the primary determinant of recurrence in conventional ameloblastoma.
The limitations of this study included variability of follow-up durations. Several patients monitored for shorter periods than typically recommended to detect late recurrence, potentially leading to underestimation of the true recurrence rate. Additional limitations included variability in the completeness of clinical and radiographic data, lack of standardized reporting of prognostic features such as tumor size, association with impacted teeth, and cortical perforation [10], as well as reliance on clinician-provided follow-up for externally managed patients. Original radiographic images were not available for review, and radiographic characterization relied on clinician-provided descriptions, which may be subject to variability. Moreover, the predominance of incisional biopsy specimens in this study limited the ability to fully evaluate histopathologic diversity within individual tumors. The limited number of cases with available follow-up data may affect the interpretation and generalizability of recurrence-related analyses.
Future multi-institutional studies incorporating standardized radiographic, histopathologic, and surgical documentation are needed to validate these findings. Molecular investigations may further elucidate tumor biology and refine recurrence risk prediction. Integrating clinical, surgical, and molecular data has the potential to guide more personalized treatment strategies for ameloblastoma.
In conclusion, this 22-year retrospective analysis of conventional ameloblastoma in a U.S. population aligned with global demographic, anatomic trends, and histopathologic features. This study reinforced that treatment approach remained the key factor influencing recurrence-free survival, emphasizing the critical role of comprehensive surgical management in minimizing recurrence. In addition, this tumor frequently exhibited mixed histopathologic subtypes, limiting the prognostic value of histologic subclassification.







Comments (0)