Patients on VV-ECMO as a bridge to lung transplantation have equivalent one-year survival outcomes compared to other transplant candidates, despite starting at a significantly higher level of illness, a logical conclusion based on the necessary indications for ECMO. Without VV-ECMO, these patients would most likely die while waiting for a transplant [27, 28]. Notably, only 4 of 116 interstitial lung disease (ILD) patients (4%) in our cohort received pre-transplant VV-ECMO. This low utilization reflects our institutional policy of reserving ECMO support for ILD candidates with acute, potentially reversible decompensation—often associated with shorter wait-list times—while avoiding VV-ECMO in stable, end-stage fibrotic ILD without new insults. In addition, the VV‑ECMO cohort skewed younger in part because ARDS predominated among VV‑ECMO bridges (28/37, 75.7%), and during the study period most ARDS transplants were COVID‑19–related (41/44, 93.2%), reflecting a pandemic‑era case‑mix rather than any age‑based exclusion policy. This study supports the continued use of VV-ECMO to bridge critically ill patients to transplantation, despite concerns about increased infection rates. Our data indicate that infections, while initially more frequent, do not significantly impact survival, emphasizing the life-saving potential of VV-ECMO. By definition, the patients requiring VV-ECMO were relatively sicker than the control group and needed additional care beyond standard ICU practice, thus justifying the use of circulatory mechanical support [2, 4].
Patients on VV-ECMO have higher infection rates, but infections are manageable and do not significantly impact survival. While persistent immune dysregulation and prolonged central-line dependence after ECMO decannulation contribute to late-onset bloodstream infections and infections are a known risk of ECMO, occurring in approximately 20.5% of adults [29], interventions like infection prevention protocols and timely management reduce their severity. Additionally, most of the infections acquired by both groups were common among solid organ transplant recipients, where prophylaxis is not necessarily available or appropriate [30, 31]. There were no infectious agents particularly endemic to the VV-ECMO population, nor were there trends in infection incidence over time that deviated significantly from the norm [32, 33]. A notable trend was the relative stability or even decrease in infections over time in the VV-ECMO group. Typically, transplant recipients with surgical or technical complications develop infections within the first 30 days, yet the VV-ECMO bridge group experienced only about a 10% relative increase in infection incidence compared to the control group, despite undergoing considerable procedural strain [34].
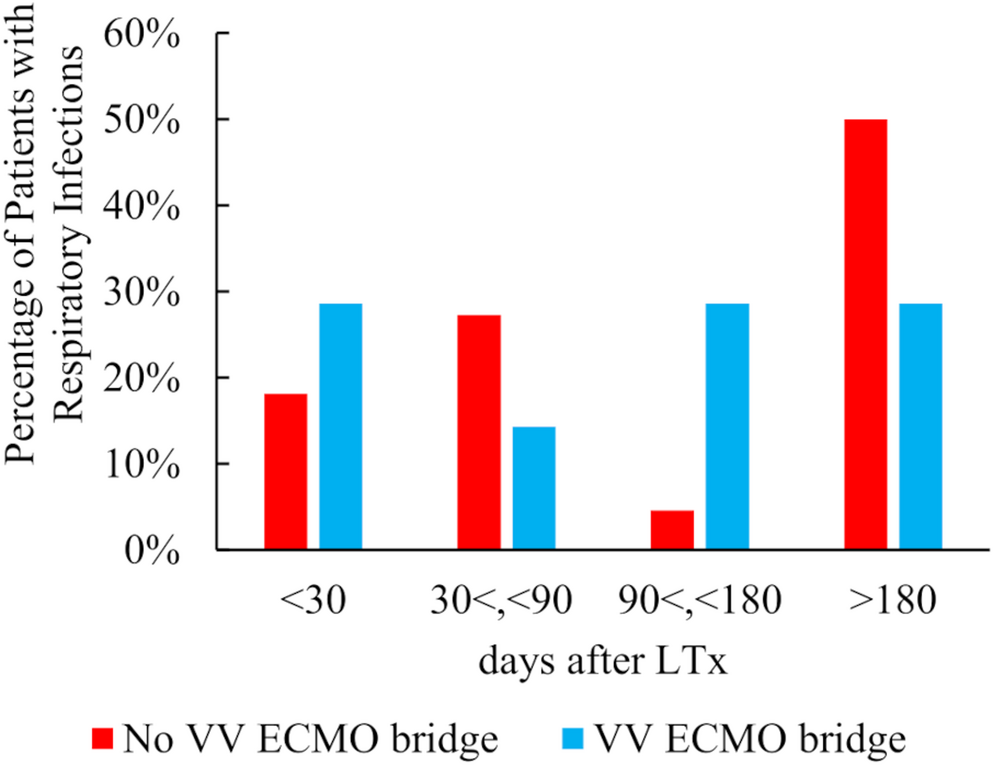
Infections were more frequent early after transplantation among patients bridged with VV‑ECMO, a temporal pattern we consider largely related to bridge‑specific exposures—large‑bore cannulation with prolonged central venous access, transfusion requirements, and transient immune perturbation—that diminish after decannulation and device removal. At our center, standardized practices likely contributed to this attenuation and could be broadly adoptable by other programs: (i) daily device‑necessity assessments with early‑decannulation pathways and prompt removal of non‑essential lines [26]; (ii) protocolized central line exchange during VV ECMO support; (iv) early mobilization, nutrition, and glycemic control; and (v) careful titration of maintenance immunosuppression. Consistent with Table 3, the pathogen spectrum mirrored that of solid‑organ transplant recipients, and no ECMO‑specific endemic organisms were observed. These observations suggest that the early excess reflects modifiable care processes rather than a persistent, ECMO‑specific susceptibility, helping explain the convergence of infection burden over time.
From a device standpoint, several artificial‑lung practices may further mitigate risk and are broadly adoptable: choosing low‑prime, heparin‑bonded circuits to reduce hemodilution and transfusions; maintaining sufficiently high flows to limit stasis; protocolized surveillance of the oxygenator with predefined thresholds for exchange; cautious, escalation‑only anticoagulation in the peri‑transplant period; and ready availability of a primed backup circuit with a standardized rapid‑exchange checklist. These artificial‑lung considerations, combined with early decannulation and line‑care bundles, likely explain the reason early infection risk attenuates rather than persists in patients bridged with VV‑ECMO.
Because patients bridged with VV‑ECMO were more likely to undergo bilateral transplantation, their operative time, ischemic time, and transfusion requirements were longer than those of controls (Table 2). To disentangle the effect of this greater surgical invasiveness from that of VV‑ECMO itself, we constructed a uni and multi variate Cox model for both respiratory and bloodstream infections that included pre‑transplant VV‑ECMO, operative time, total ischemic time, and intra‑operative transfusion volume (Tables 4 and 5). Operative and ischemic times were not significant risk factors in multivariable analyses for respiratory infection and not significant in univariate analysis for bloodstream infection. In contrast, pre‑transplant VV‑ECMO remained an independent predictor of bloodstream infection (HR 2.28, 95% CI 1.03–5.03, p = 0.047), whereas it was not associated with respiratory infection. These findings indicate that the excess risk of bloodstream infection is more strongly related to the VV‑ECMO bridge itself than to surgical complexity per se.
When considering infection risk, it is also important to account for pre-transplant risk factors that contribute to post-transplant infections more than VV-ECMO itself. Factors such as donor age, need for mechanical ventilation, smoking, alcohol use, history of infection, and aspiration all impact the likelihood of PGD, making it inaccurate to attribute infections solely to VV-ECMO [33,34,35,36,37]. Our data also reflects similar trends in which risk factors negatively predicted outcomes. Although the risks identified in univariate and multivariate analyses of VV-ECMO should not be trivialized, it is important to note that patients requiring this therapy would likely not have survived to transplant without it. Therefore, reducing these global risk factors could help mitigate infections while preserving the benefits of VV-ECMO.
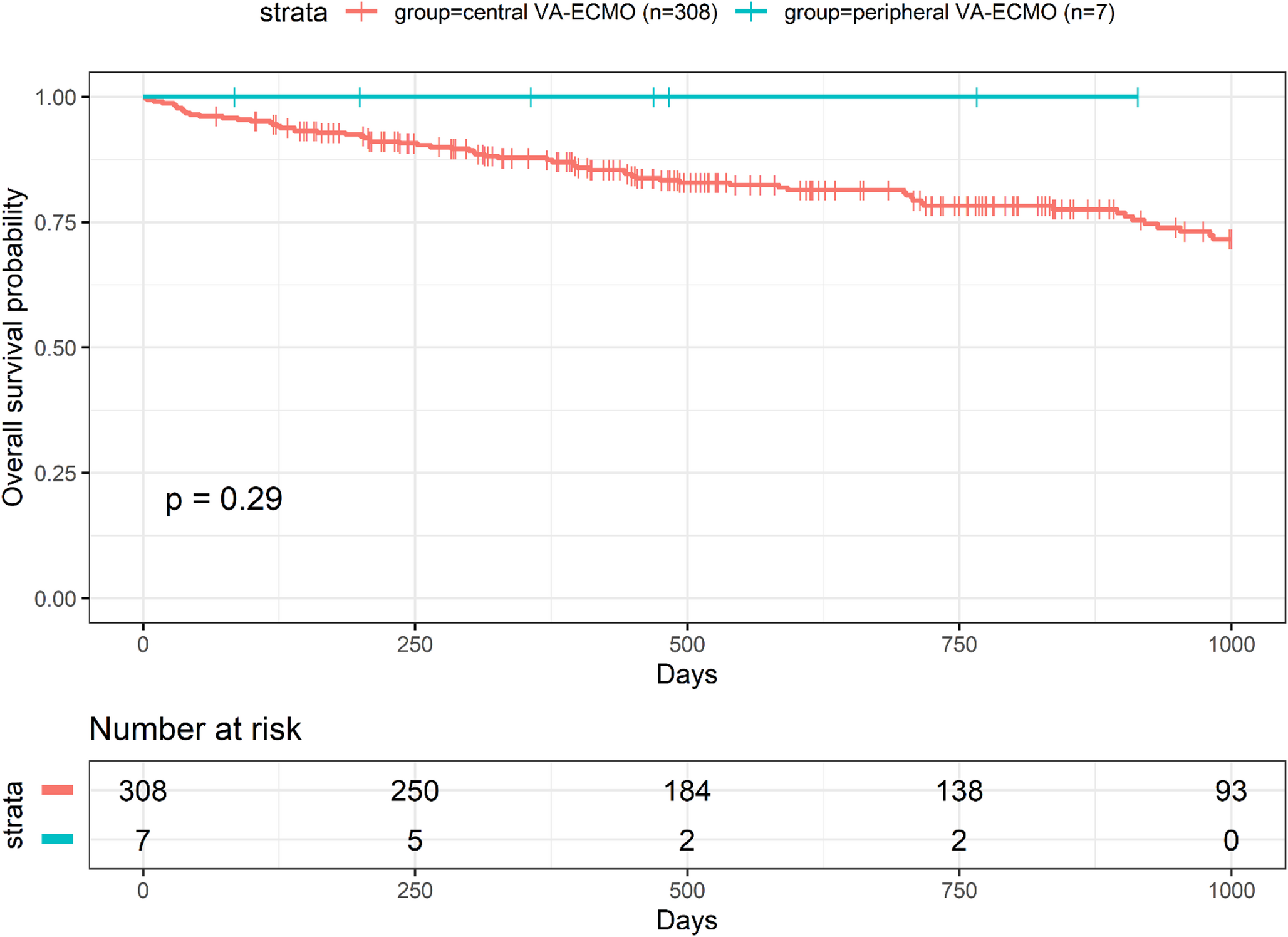
Despite higher initial illness severity, VV-ECMO patients achieve comparable one-year survival rates to non-ECMO patients. Beyond the first year, the survival curve flattens, indicating no recurring infections or ongoing complications. Additionally, there is no statistically significant difference (89.8% vs. 81.1%, p = 0.16) in one-year survival between groups. Although most ECMO-infection risk literature focuses on managing infections during ECMO use, these insights can reasonably be applied to post-VV-ECMO management as well [38].
VV-ECMO allows critically ill patients to remain stable long enough to receive a transplant, ensuring equitable outcomes despite their critical condition. Short of irreversible lung disease, the need for intubation alone should not preclude a patient from transplant eligibility [39]. While VV-ECMO patients experience infections earlier, their survival trajectories align with other candidates over time. Infections decline after the first year, suggesting they are largely acute and manageable. Furthermore, for clinicians concerned about infection risks, ECMO technology and infection-risk mitigation protocols are continuously evolving and being implemented with great success [36, 40].
ECMO has been steadily increasing in use over the last couple of decades across thoracic surgery and while there are certainly opportunities to optimize the technology, many consequential applications have arisen for patients requiring more intensive care than the standard delivered in ICUs [41, 42].
Limitations
This study has a few limitations. Firstly, it is a retrospective single-center cohort, which may limit generalizability to other centers or countries. However, given the life-saving circumstances in which VV-ECMO is used, conducting a randomized controlled trial would be ethically challenging [43]. Additionally, prospective studies are difficult for this study due to the relatively small sample sizes, population heterogeneity, and unpredictable clinical course.
Regarding the increased incidence of infection in VV-ECMO patients, the study’s small sample size, an inherent limitation due to the severity of the condition and treatment and preoperative medical ventilation, may overemphasize infection rates. However, total survival data indicate that infections do not significantly shorten the lifespan of VV-ECMO patients, despite their higher baseline illness severity. These patients are carefully selected based on strict criteria for VV-ECMO therapy while waiting for a transplant, reinforcing the overall benefit of this life-sustaining intervention. To address potential confounding by age and the temporal impact of COVID-19, we performed a prespecified OS analysis restricted to recipients ≥ 55 years and re-fitted multivariable models including age; neither analysis identified an independent excess risk associated with VV-ECMO bridging. Nevertheless, residual confounding and the limited sample size of the VV-ECMO cohort remain important limitations.

Comments (0)