
Remember me
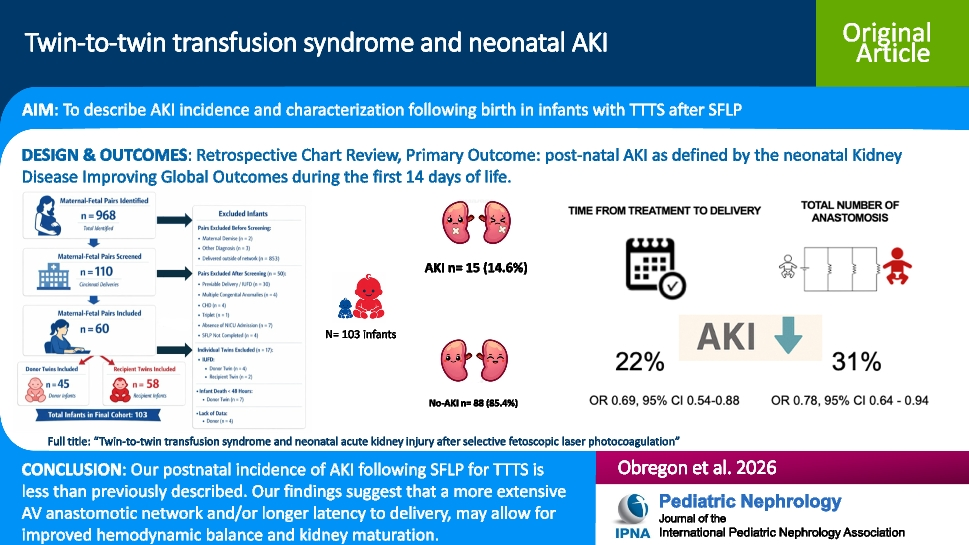
During the study period, 60/968 (6%) of maternal–fetal pairs met inclusion criteria, resulting in a final cohort of 103 infants (45 donors, 58 recipients). Some individual twins were excluded due to in utero fetal demise, infant death within 48 h, or lack of NICU admission (Fig. 1).
Fig. 1
STROBE flow diagram. *Maternal demise not related to the procedure
There were no statistically significant differences in maternal demographics, comorbidities, obstetric complications, or corticosteroid administration between pregnancies in which at least one twin experienced AKI, compared to those in which neither twin was affected. However, AKI was more common following pregnancies in which indomethacin was used for tocolysis (53.8% vs. 23.4%, p = 0.04), but no significant differences were observed with other nephrotoxic agents [14] (Table 1).
Table 1 Maternal characteristicsIn pregnancies where at least one twin was diagnosed with AKI, the mean gestational age (GA) at SFLP was 22 (SD ± 2.82) weeks with the majority classified as Quintero Stage III (69.2% vs. 56.4%, p = 0.95) (Table 2). These pregnancies had a lower total number of placental vascular anastomoses compared to those without AKI (12 vs. 22, p < 0.01) (Table 2). Both donor-to-recipient (D-R) anastomoses (5 vs. 9, p = 0.03) and recipient-to-donor (R-D) anastomoses (6 vs. 12, p = 0.02) were fewer. Additionally, latency to delivery (i.e., interval between SFLP and birth) was significantly shorter in pregnancies affected by AKI (4 weeks vs. 9 weeks, p < 0.01) (Table 2). Placental share among both groups was comparable for donors and recipients.
Table 2 SFLP characteristicsAmong 103 infants, 15 (14.6%) were diagnosed with neonatal AKI in the first 2 weeks of life. Twins with AKI were born at earlier GA (26 weeks vs. 30 weeks, p < 0.01) and had lower birth weights (923 vs. 1320 g, p = 0.02) compared to those without AKI. Infants with AKI had a higher need for vasopressor use in their first week of life (26.7% vs. 10.2%, p = 0.09), increased incidence of respiratory distress (100% vs. 65.9%, p < 0.01), and required more days of mechanical ventilation (15 days vs. 9 days, p = 0.03). Twin status (i.e., donor vs. recipient) was not different between twins with and without AKI (Table 3). Other comorbidities, including grade 3 or 4 intraventricular hemorrhage, cardiovascular dysfunction, pulmonary hypertension, persistent ductus arteriosus, necrotizing enterocolitis, and exposure to nephrotoxic medications [14] were similar between both groups.
Table 3 Prenatal and postnatal infant characteristicsAmong the 15 infants diagnosed with AKI, 8 met diagnostic criteria based on sCr and 3 based on UOP, while 4 infants met criteria based on both parameters (Appendix 2). Infants who met both sCr and UOP criteria had higher stages of AKI compared to those who met criteria based on either parameter alone. There were no differences between the groups in terms of AKI duration, exposure to nephrotoxic medications [14], or twin status (Table 4). Interestingly, only 5 of the 15 infants with AKI had the condition documented in their problem list, and nephrology was consulted in just one of these cases.
Table 4 AKI characteristics by diagnosis criteriaIn unadjusted analysis, birth weight and GA were associated with AKI, but vasopressor need in the first week of life did not affect the outcome. Since gestational age (GA) and birth weight were highly correlated with latency to delivery, the latter was kept to minimize the number of covariates due to limited sample size. Twin status, latency to delivery, deep vertical pocket before SFLP and total number of anastomoses were examined in the mixed model while controlling for hypotension in the first week and gestational age at birth.
Final covariates included in the model were latency to delivery and total number of anastomoses. Adjusted analysis showed that the main predictors of AKI were latency to delivery (aOR 0.69, 95% CI 0.54–0.88, p < 0.01) and total number of arteriovenous (AV) anastomoses (aOR 0.78, 95% CI 0.64–0.94, p = 0.01).
Comments (0)