In this study, we performed a cross-sectional plasma cholestanol screening in 103 children with ASD to investigate the potential cases of undiagnosed CTX and explore associated sterol metabolism patterns. Although 27 ASD patients (26.2%) had elevated cholestanol levels (≥ 7 µg/mL), no cases of CTX were confirmed by CYP27A1 gene analysis. However, an unexpected observation was the concurrent elevation of cholestanol and additional sterol fractions - particularly campesterol, sitosterol and stigmasterol - in these patients, with levels significantly higher than in typically developed children. Importantly, the dietary assessments revealed no significant differences in total fat intake or consumption of foods high in phytosterols between ASD patients with elevated and normal cholestanol levels, suggesting that the elevated sterol levels observed are unlikely to be due to dietary or environmental factors. These results support the hypothesis that subtle alterations in bile acid metabolism may be present in a subset of children with ASD. Our findings suggest that cholestanol-based CTX screening in clinically unselected ASD cohorts may have a low diagnostic yield; targeted evaluation guided by additional suggestive clinical features may be more informative. However, our results indicate that bile acid-related metabolic pathways may be future targets for ASD research and therapeutic exploration.
The clinical course of CTX is heterogeneous and the presentation varies according to age: chronic diarrhea and persistent neonatal cholestasis often occur in infancy, intellectual disability and juvenile cataract in early childhood, while progressive neurologic findings - cerebellar, pyramidal and extrapyramidal signs - often do not appear until adolescence or adulthood (Federico and Gallus 1993; Mignarri et al. 2014). Although earlier studies considered neurological deterioration predominantly in adulthood, more recent studies have emphasized that neurological symptoms can also occur in childhood (Wong et al. 2018; Zubarioglu et al. 2024). Early diagnosis is critical, as timely administration of CDCA can prevent or stabilize neurological impairment (Stelten et al. 2019, 2021; Verrips et al. 2020). However, due to significant clinical overlap with other neurodegenerative diseases, CTX is often underdiagnosed or misdiagnosed, resulting in an average diagnostic delay of nearly two decades (Mignarri et al. 2014; Zubarioglu et al. 2024). In response, targeted screening strategies have been proposed in at-risk populations, particularly patients with juvenile cataracts, where CTX diagnosis has actually been made in a subset of cases with a prevalence between 0.99 and 3.3% (Freedman et al. 2019, 2023; Atilla et al. 2021; Fernández-Eulate et al. 2022). However, large-scale screening measures for CTX are largely limited to cataract populations.
Previous case reports and observational studies have described the co-occurrence of CTX and ASD, suggesting that ASD may represent an early neurodevelopmental manifestation of CTX in rare cases (Stelten et al. 2018; Zubarioglu et al. 2024). Behavioral and psychiatric symptoms, including autism-like features, may not only be part of the broader CTX phenotype, but may also respond positively to CDCA replacement therapy if initiated early, indicating a potentially reversible component of neuropsychiatric involvement (Stelten et al. 2018). However, ASD populations have not been routinely included in CTX screening strategies and few literatures have examined this association, despite the possibility that subtle metabolic disturbances may contribute to the ASD phenotype. The limited number of publications addressing CTX screening in individuals with ASD emphasizes the importance of further studies in this under-researched area (Karadag et al. 2024).
To date, the only study in the literature to screen for CTX in an ASD population is a prospective observational study that included 101 pediatric patients diagnosed with ASD who also had at least one systemic or psychiatric symptom suggestive of CTX according to the Mignarri Suspicion Index (Karadag et al. 2024). All participants underwent direct CYP27A1 gene sequencing without prior plasma sterol screening, and two patients (1.9%) were found to carry biallelic variants of uncertain significance (VUS). Although plasma cholestanol cut-off values were not assessed or optimized due to the lack of pre-screening, the study highlighted that targeted genetic testing in clinical high-risk ASD subgroups, especially in patients with early systemic and psychiatric comorbidities, may facilitate early identification of CTX and enable timely CDCA treatment to prevent irreversible neurological deterioration.
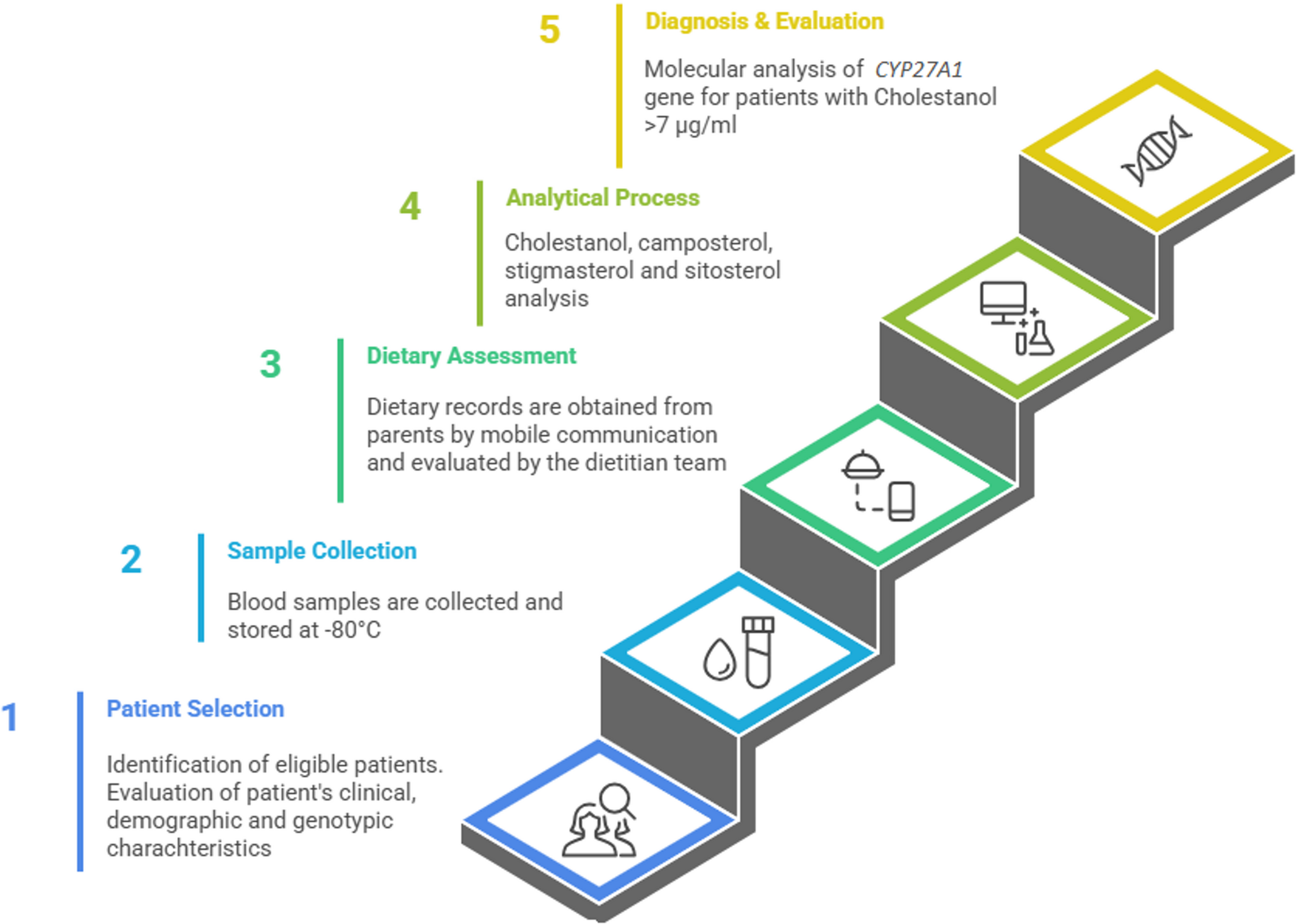
In our study, a complementary biochemistry-based strategy was used to explore CTX risk in a similarly sized, clinically unselected cohort of 103 children diagnosed with ASD, using measurement of plasma cholestanol measurement as an initial screening step and performing CYP27A1 gene analysis only in those with elevated levels. Elevated plasma cholestanol levels were detected in 27 participants; however, no case of CTX was confirmed by genetic analysis. The absence of a CTX diagnosis in this cohort may suggest that individuals with isolated ASD may not be an appropriate target group for CTX screening, especially in the absence of characteristic features such as juvenile cataract, chronic diarrhea, or tendon xanthomas. However, our results revealed an unexpected secondary observation regarding plasma sterol profiles within the ASD population. A notable proportion of ASD patients (26%) had plasma cholestanol concentrations above 7 µg/ml and mean plasma cholestanol levels were significantly higher in the ASD group compared to typically developed children (p < 0.001). False high cholestanol levels may occur due to high dietary phytosterol intake, contamination of samples or concurrent hepatic conditions such as cholestasis or sitosterolemia. However, in our study, possible causes of secondary elevation were systematically excluded. The effects of high nutritional phytosterol intake were ruled out by dietary intake records and no concomitant hepatic or pharmacologic confounders were identified. This observation raises the question of whether subtle disturbances of bile acid metabolism are more common in ASD than previously thought and suggests the need to investigate the possible role of sterol metabolism abnormalities in the pathophysiology of ASD.
Sterol metabolism provides an informative surrogate marker for bile acid metabolism, as both metabolic pathways start from cholesterol and involve overlapping enzymatic steps (Russell 2003). In liver tissue, cholesterol is first converted to 7-α-hydroxycholesterol by cholesterol 7α-hydroxylase (CYP7A1), which is the rate-limiting step of the classical bile acid synthesis pathway (Federico and Gallus 1993; Nie et al. 2014). Subsequent enzymatic reactions ultimately produce the primary bile acids cholic acid and chenodeoxycholic acid. Disruptions at any point in this cascade - whether due to enzyme deficiencies, mitochondrial dysfunction or regulatory impairments - can lead to an accumulation of metabolic intermediates and a diversion of cholesterol into alternative pathways (Nie et al. 2014). This diversion leads to increased concentrations of neutral sterols such as cholestanol and phytosterols such as campesterol and stigmasterol (de Sain-van der Velden et al. 2008). Elevated serum sterol concentrations may therefore serve as an accessible biochemical indicator of impaired bile acid synthesis contextualizing our findings within a broader framework of altered sterol and bile acid homeostasis in individuals with ASD.
Bile acid biosynthesis is a tightly regulated, multi-step metabolic pathway involving numerous hepatic enzymes, and even mild impairments of this cascade, whether through genetic polymorphisms, impaired transcriptional control or alterations in the gut microbiota, can disrupt sterol homeostasis (Yang et al. 2024). Untargeted urine metabolomics in acute intermittent porphyria have revealed a disturbance of bile acid metabolism, which may contribute to the prediction of clinical attacks (Lefebvre et al. 2025). Similarly, in Niemann-Pick disease type C, specific glycine-conjugated bile acid species have been found to be significantly elevated and now serve as sensitive diagnostic biomarkers (Jiang et al. 2016).
Beyond CTX, several disorders of cholesterol biosynthesis can present with neurodevelopmental phenotypes and may also disrupt bile acid homeostasis. Smith-Lemli-Opitz syndrome (SLOS), which results from impaired cholesterol biosynthesis, is well recognized as being associated with autistic features (Sikora et al. 2006). Abnormal bile acid synthesis has been reported in SLOS, and bile acid-based interventions have been explored in more severely affected individuals (Svoboda et al. 2012). Recent studies have also highlighted a potential link between bile acid metabolism and ASD. In a population-based case-control study, maternal mid-pregnancy serum of women whose children were later diagnosed with ASD was shown to display elevated levels of metabolites involved in bile acid biosynthesis, suggesting that alterations in maternal bile acid profiles may play a role in early fetal neurodevelopment (Ritz et al. 2020). This is supported by an experimental study using a mouse model of ASD that found evidence of impaired bile acid production in the liver, again suggesting a possible link between bile acid metabolism and neurodevelopment (Cao et al. 2023). Consistent with these findings, a large Swedish population-based study found an increased risk of ASD in children born to mothers with intrahepatic cholestasis during pregnancy, providing further evidence of elevated maternal bile acid levels as a potential factor in susceptibility to neurodevelopment (Chen et al. 2024). Overall, these findings suggest that intrinsic disturbances in bile acid metabolism, whether maternal, hepatic or systemic in origin, represent a contributing mechanism in ASD and warrant further investigation as potential biomarkers or therapeutic targets.
This possible association between ASD and bile acid metabolism raises the question of where it comes from. This could be caused or exacerbated by abnormalities in the gut microbiome, a common feature observed in affected individuals (Pulikkan et al. 2019). Intestinal bacteria play a central role in the deconjugation, transformation and enterohepatic circulation of bile acids. Dysbiosis may lead to altered bile acid pools, resulting in impaired reabsorption and accumulation of intermediate sterols (Jones et al. 2014). This is particularly important as infantile diarrhea, as seen in CTX, indicates malabsorption of bile acids; similarly, a subset of idiopathic ASD cases also have chronic diarrhea, which could indicate subtle bile acid diarrhea or malabsorption. In addition, gut-derived metabolites may modulate systemic inflammation and metabolic signaling, further influencing brain development. Aberrant bile acid profiles may also result in failure to activate gut–brain signaling pathways, such as those involving FXR and TGR5, which normally support neurodevelopment (Pols et al. 2011). In children with ASD, gastrointestinal symptoms often co-occur with behavioral symptoms, and altered microbial profiles have been associated with changes in lipid metabolites (El-Ansary et al. 2020). Therefore, the gut–liver–brain axis may act as both a source and mediator of bile acid and sterol imbalance in ASD, providing a unifying framework that integrates environmental, microbial and host-specific metabolic contributions to neurodevelopmental risk.
In addition to the elevated cholestanol levels, we observed elevated levels of plant sterols in some children with ASD. These phytosterols are provided with food and serve as surrogate biomarkers for intestinal cholesterol absorption. However, prior studies evaluating plant sterols in ASD have reported heterogeneous findings. For example, Tierney et al. quantified sitosterol and cholesterol precursors in an ASD cohort and reported that sitosterol concentrations were generally within laboratory reference ranges, with only mild elevations in a small subset (Tierney et al. 2021). In our cohort, sitosterol likewise remained within the reference interval at the group level (median 3.69 µg/mL), yet it was modestly higher than in typically developed controls, indicating a subtle shift rather than overt sitosterolemia; only one child had sitosterol > 15 µg/mL and ABCG5/ABCG8 sequencing was negative. In particular, elevated plasma levels of plant sterols have been reported in untreated CTX patients and shown to decrease after bile acid replacement therapy with CDCA (Mignarri et al. 2016). In this study, the authors hypothesized that high cholic acid levels prior to treatment may improve sterol absorption, a mechanism that may be reversible with CDCA. However, none of the participants in our cohort were diagnosed with CTX; nevertheless, similar elevations in phytosterols were noted. This finding raises the question of whether some individuals with ASD have unique alterations in sterol absorption or sterol metabolism that may be related to bile acid composition, intestinal transporter activity, or gut microbiota. Although dietary intake may influence sterol levels, our analysis considered dietary sterol sources and excluded secondary dietary factors. These results suggest that phytosterol profiling may provide additional insight into cholesterol homeostasis and metabolic heterogeneity within populations with ASD.
This study has several limitations. First, although our sample size of 103 children with ASD is relatively large compared to many previous studies, it remains small for a screening study aimed at assessing the prevalence of a rare disorder such as CTX. Second, although we determined plasma sterol levels as a proxy for bile acid metabolism, we did not evaluate the full spectrum of bile acid intermediates and elements of the metabolic pathway, which would have allowed a more comprehensive assessment of subtle disorders of bile acid synthesis. Third, dietary recalls were collected only in ASD participants; therefore, dietary energy/macronutrient intake and phytosterol-rich food consumption could not be directly compared between ASD and control children. Lastly, although significant changes in sterol levels were found, we did not investigate potential associations between these biochemical findings and autism symptom severity using standardized clinical rating scales such as the Childhood Autism Rating Scale (CARS).


Comments (0)