
Remember me
A 70-year-old woman presented to our hospital for a thorough examination of liver nodules. She had a documented medical history of alcoholic liver disease diagnosed at the age of 60 years. Her alcohol intake history included consumption of 40 g of pure ethanol daily for 50 years. She had an allergy to iodine-based contrast agents. In X-4 years, she underwent abdominal computed tomography (CT) scan, during which micronodules were detected in bilateral lobes of the liver. In addition, two small nodules (< 10 mm) showing strong enhancement in the arterial phase were detected in S4, S6 on gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid enhanced magnetic resonance imaging (Gd-EOB MRI). Since then, she had undergone periodic imaging examinations. In year X, she was admitted to our hospital for close examination and treatment after an abdominal CT scan revealed that several nodules had grown over 4 years.
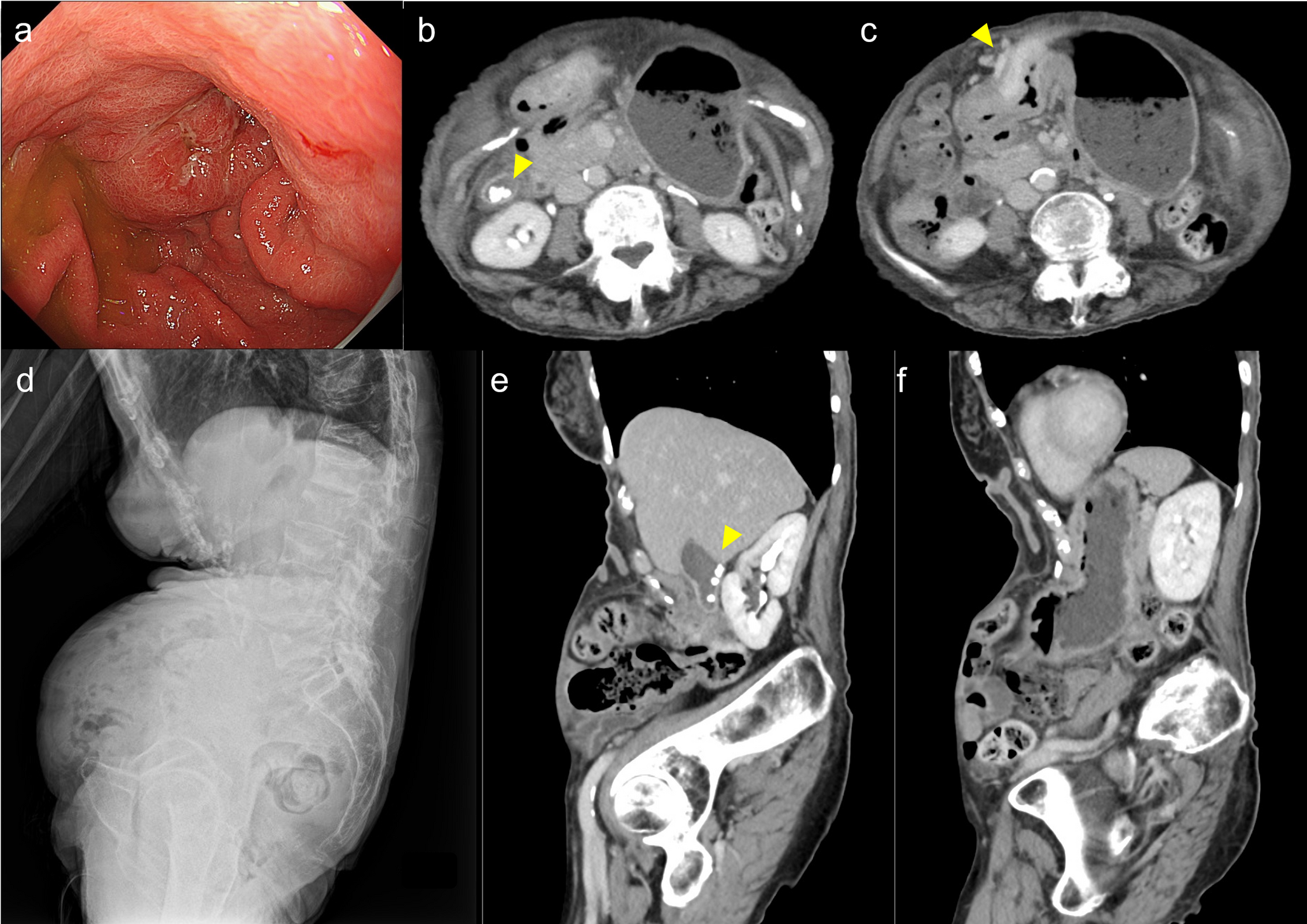
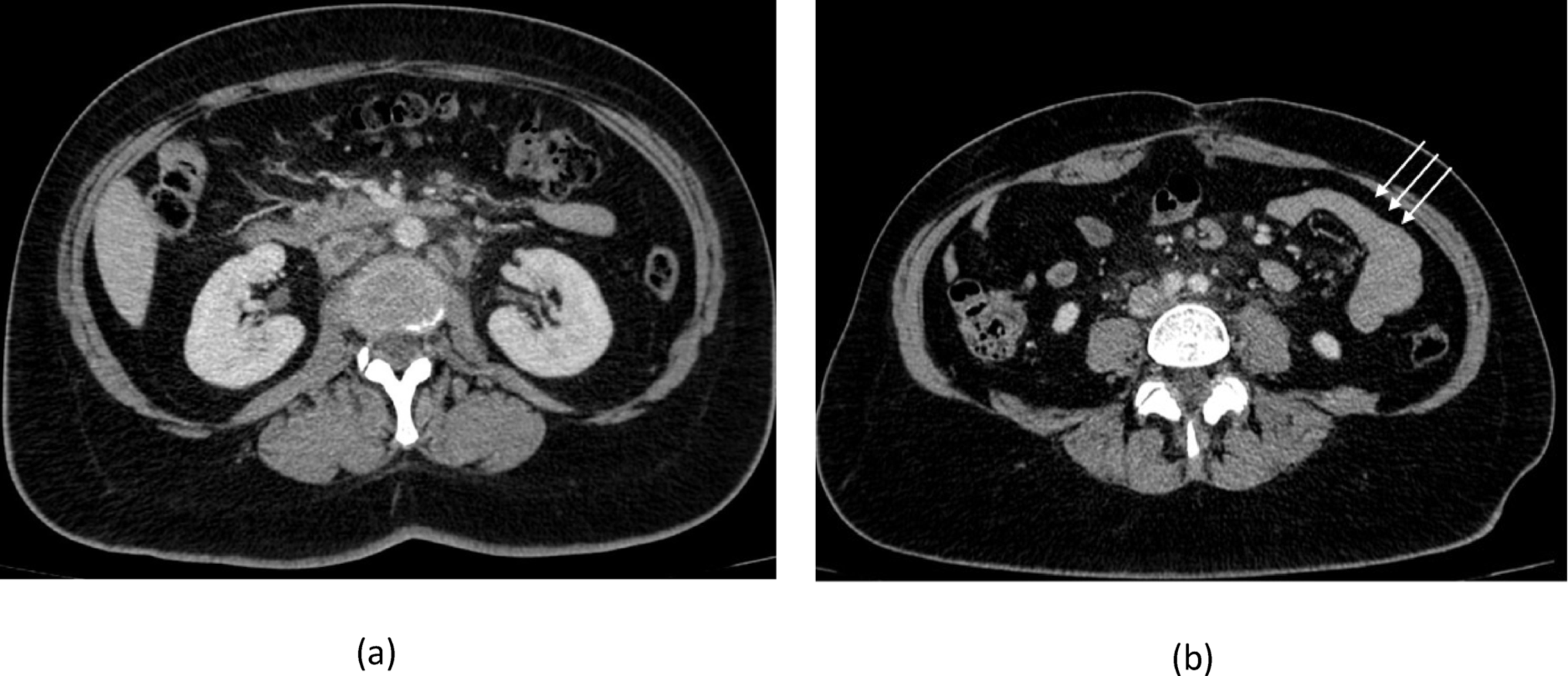
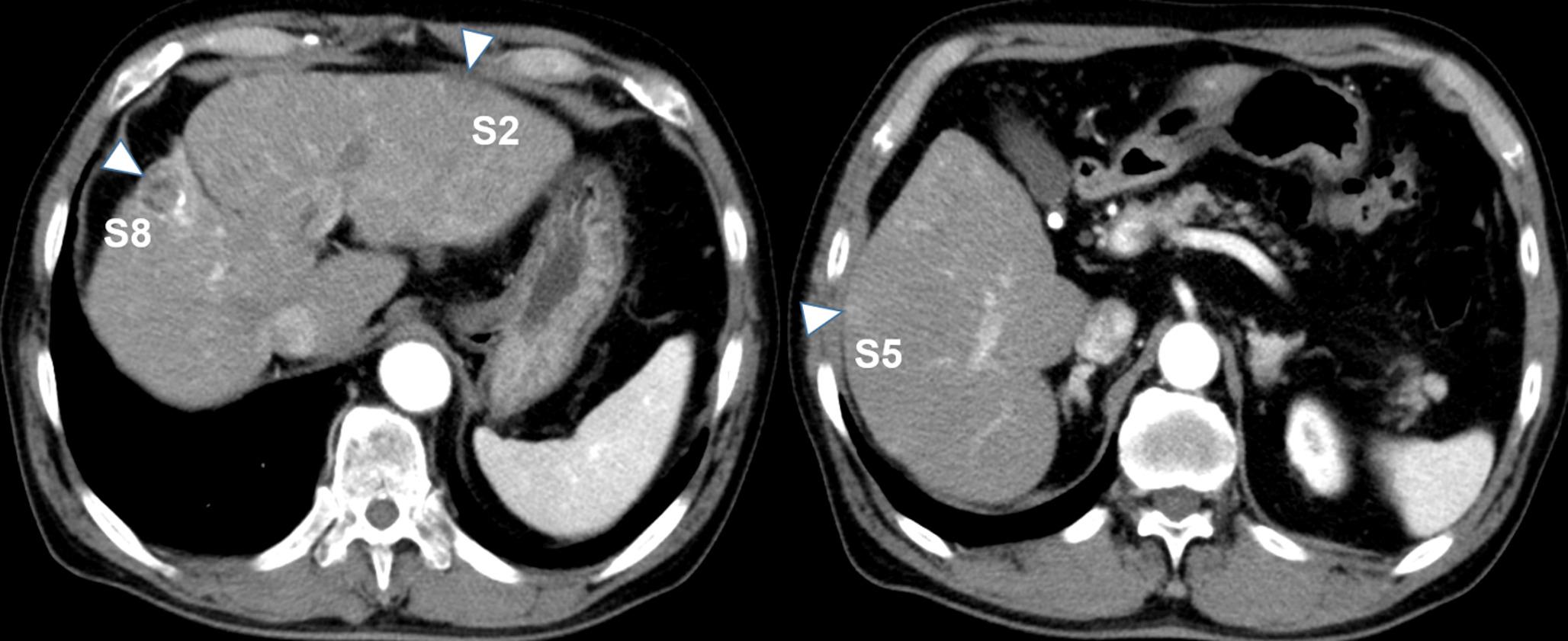
The blood tests revealed modest hepatic dysfunction, corresponding to Child–Pugh class A. However, levels of alpha-fetoprotein (AFP) and protein induced by vitamin K absence or antagonist-II (PIVKA-II) were both normal. The blood test results obtained upon admission are presented in Table 1. The abdominal CT scan revealed the 25 mm nodule at S4 and the 19 mm nodule at S6. There was also a new 12 mm nodule at S7 (Fig. 1a-c). In addition, multiple viable small lesions were detected throughout the liver. On Gd-EOB MRI, these nodules were highly enhanced on T1-weighted imaging (T1WI), low-signal on fat-suppressed T1WI, high-signal on T2-weighted imaging, high-signal on diffusion weighted imaging, strongly enhanced in the arterial early phase. In the hepatobiliary phase, the S4 and S6 nodules showed low signal intensity consistent with decreased uptake, whereas the S7 nodule demonstrated weakly enhanced signal intensity with only minimal reduction of uptake (Fig. 2a-c). Neither extrahepatic lesions nor intrahepatic vascular invasion were detected on both CT and MRI.
Table 1 Laboratory serum test resultsFig. 1
Clinical course of the patient. This figure demonstrates the temporal changes in the target nodules observed on contrast-enhanced computed tomography (CT) scans (arterial phase) and tumor marker levels in response to various treatments. The upper, middle, and lower panels (a, b, and c) display the S4, S6, and S7 nodules, respectively. These panels demonstrate the temporal changes in the different hepatocellular carcinoma (HCC) nodules in response to various treatments. a The S4 and b S6 nodules showed reduced contrast enhancement following the initiation of lenvatinib treatment. The subsequent introduction of atezolizumab plus bevacizumab therapy resulted in further tumor shrinkage and hypovascularization. c The S7 nodule continued to grow throughout the treatment period; however, proton beam therapy (PBT) led to a reduction in size and hypovascularization of this lesion. AFP, alpha-fetoprotein; PIVKA-II, protein induced by vitamin K absence or antagonist-II
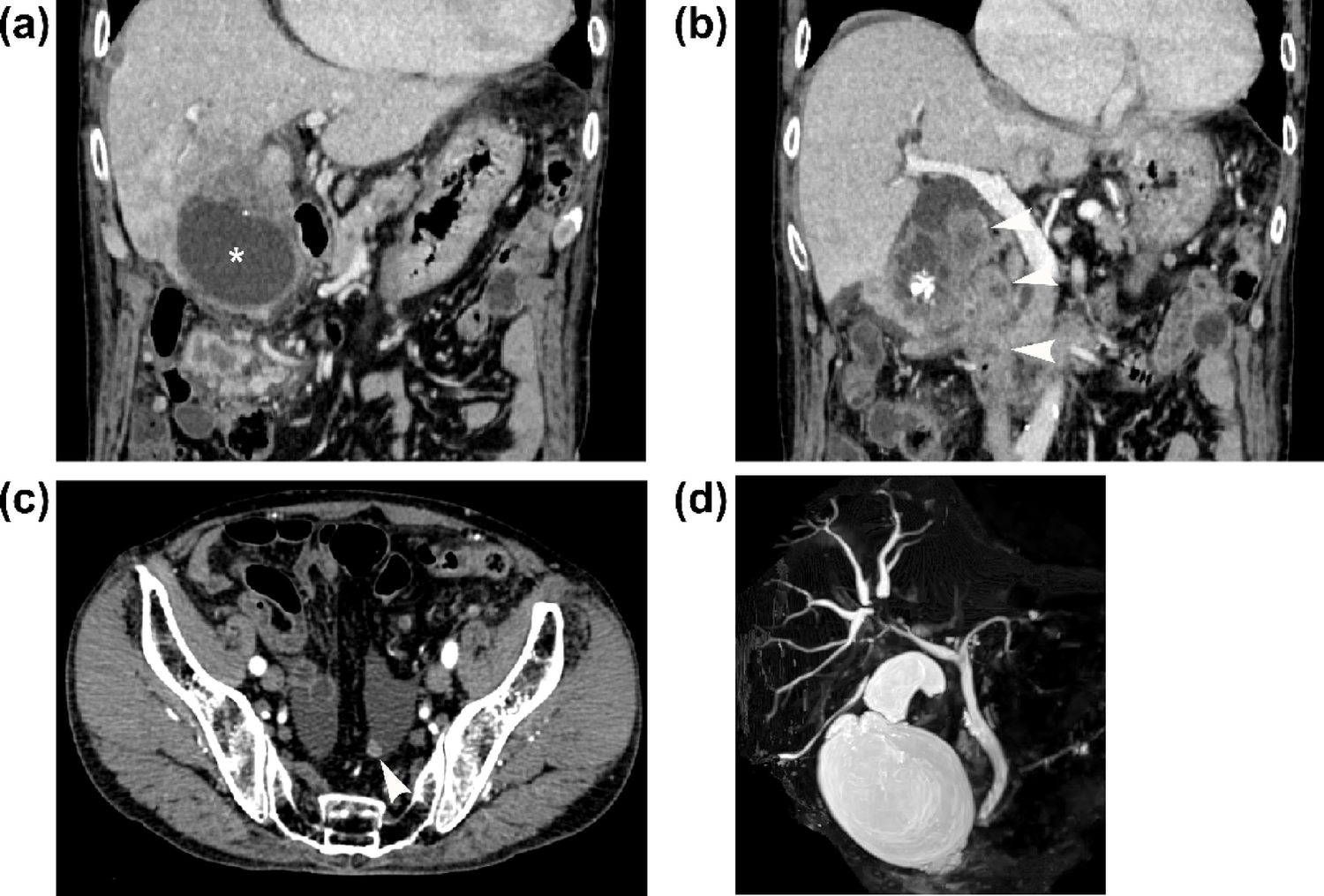
Fig. 2
Magnetic resonance imaging (MRI) assessment of the S4, S6, and S7 nodules at the initial examination. Nodules in the a S4, b S6, and c S7 demonstrated the following characteristics: hyperintensity on T1-weighted imaging (T1WI), isointensity on fat-suppressed T1WI, hyperintensity on both T2-weighted imaging (T2WI) and diffusion-weighted imaging (DWI), early enhancement in the arterial phase. In the hepatobiliary phase, the S4 and S6 nodules demonstrated decreased uptake with low signal intensity, while the S7 nodule retained weakly enhanced signal intensity with less reduction in uptake. In panel (c), the top‑right inset provides the enlarged hepatobiliary phase view. White arrowheads indicate the nodules. Most of these imaging features were consistent with hepatocellular carcinoma (HCC)
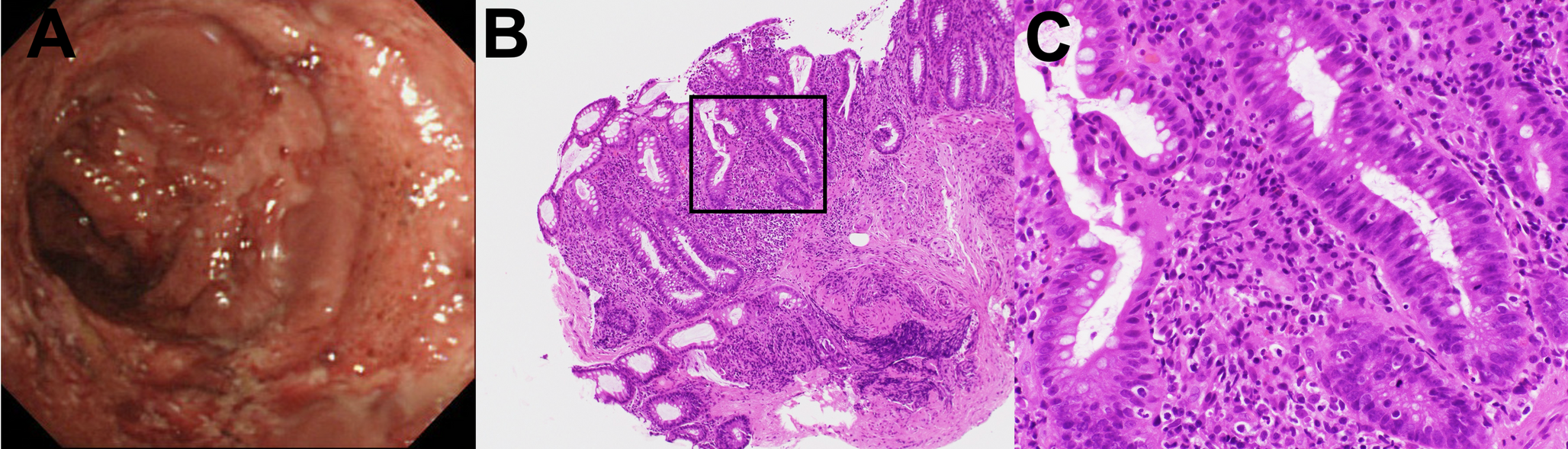
While the imaging results were mostly consistent with HCC, we proceeded with a percutaneous ultrasound-guided biopsy of the S6 nodule for histological confirmation, considering the absence of any elevation in characteristic tumor markers. Analysis of a biopsy specimen obtained from the S6 nodule showed a typical image of a well-differentiated HCC with proliferation of atypical cells, multiple layers of hepatocellular carcinoma, and structural disorganization (Fig. 3a). The background liver showed cirrhosis with extensive fibrosis and inflammatory cell infiltration in the portal vein area, while the hepatocytes had the appearance of alcoholic hepatitis with fatty deposits, overall classified as A2F4 according to the New Inuyama classification [12]. The S6 nodule was histologically confirmed as HCC. The S4, S7, and other micronodules were also diagnosed as HCC based on imaging findings, referring to histological features of the S6 biopsied lesion. Based on imaging findings of those HCC nodules such as affecting multiple segments in her liver and the absence of portal vein invasion, the patient was diagnosed with MO-HCC, developed on a background of alcoholic cirrhosis [13, 14].
Fig. 3
Immunohistochemical staining for β-catenin in liver nodule biopsies. a–c Biopsy samples obtained from the S6 nodule prior to treatment. The S6 nodule was negative for β-catenin. d–f Biopsy samples obtained from the progressively-enlarging S7 nodule at 31 months following treatment initiation. Most tumor cells demonstrated nuclear β-catenin positivity. a Hematoxylin and eosin (H and E) staining, × 20. b β-catenin staining, × 20. c β-catenin staining, × 80. d H and E staining, × 20. e β-catenin staining, × 20. f β-catenin staining, × 80
As her hepatic function was reserved, she was classified to have BCLC stage B. Her condition met the up-to-7 criteria out; thus, a course of systemic chemotherapy was decided upon [4]. The treatment course and the changes in each particular nodule at S4, S6 and S7 over time are illustrated in Fig. 1. In December X, lenvatinib was initiated (atezolizumab plus bevacizumab was not indicated for HCC in Japan and was the first-line drug at the time). After initiating lenvatinib therapy, the AFP levels showed a progressive increase. A subsequent MRI scan in February X + 2 revealed disappearance of the micro-nodules, while the S4 and S6 nodules had become hypovascular. However, the size of the nodule at S7 had increased from 12 to 32 mm. Based on response evaluation criteria in solid tumors (RECIST) criteria [15], the patient was diagnosed with progressive disease (PD) and transitioned to atezolizumab plus bevacizumab therapy, which had passed adaptation for HCC in Japan [6]. After starting atezolizumab plus bevacizumab therapy, the AFP levels returned to normal. In total, 34 courses of atezolizumab plus bevacizumab therapy were administered; 22 of these courses involved atezolizumab alone, with bevacizumab omitted owing to the adverse effect of proteinuria. An MRI scan performed in April X + 3 revealed further diminution of nodules S4 and S6, but an increase in the size of the lesion in S7 from 32 to 40 mm. Due to the disparate response among those nodules to atezolizumab plus bevacizumab therapy, a liver tumor biopsy of S7 nodule was conducted. Pathologically, the S7 nodule was diagnosed as an intermediate to highly differentiated HCC (Fig. 3d). In order to investigate the difference in treatment response, β-catenin staining was performed. The S6 nodule exhibited a negative expression of β-catenin, whereas the S7 nodule demonstrated a positive nuclear expression (Fig. 3b, c, e, f).
As the other lesions were under control, PBT was administered to treat the lesion in S7 in June X + 3 following 20 courses of atezolizumab plus bevacizumab therapy. The combination therapy was subsequently restarted, and a CT scan in September X + 3 showed decreased contrast enhancement, which was suspected to be necrosis in the S7 nodule. Subsequently, a CT scan in June X + 4 showed tumor resolution. After completing an additional 14 courses of atezolizumab plus bevacizumab therapy (34 courses in total), the treatment was discontinued in July X + 4 based on the sustained normalization of tumor markers, complete disappearance of target lesions, and absence of any new HCC lesions. The patient currently remains in good general health with no recurrence.
Comments (0)