Thoracoscopic biopsy should be considered for pulmonary nodules with the halo sign during immunotherapy for hepatocellular carcinoma
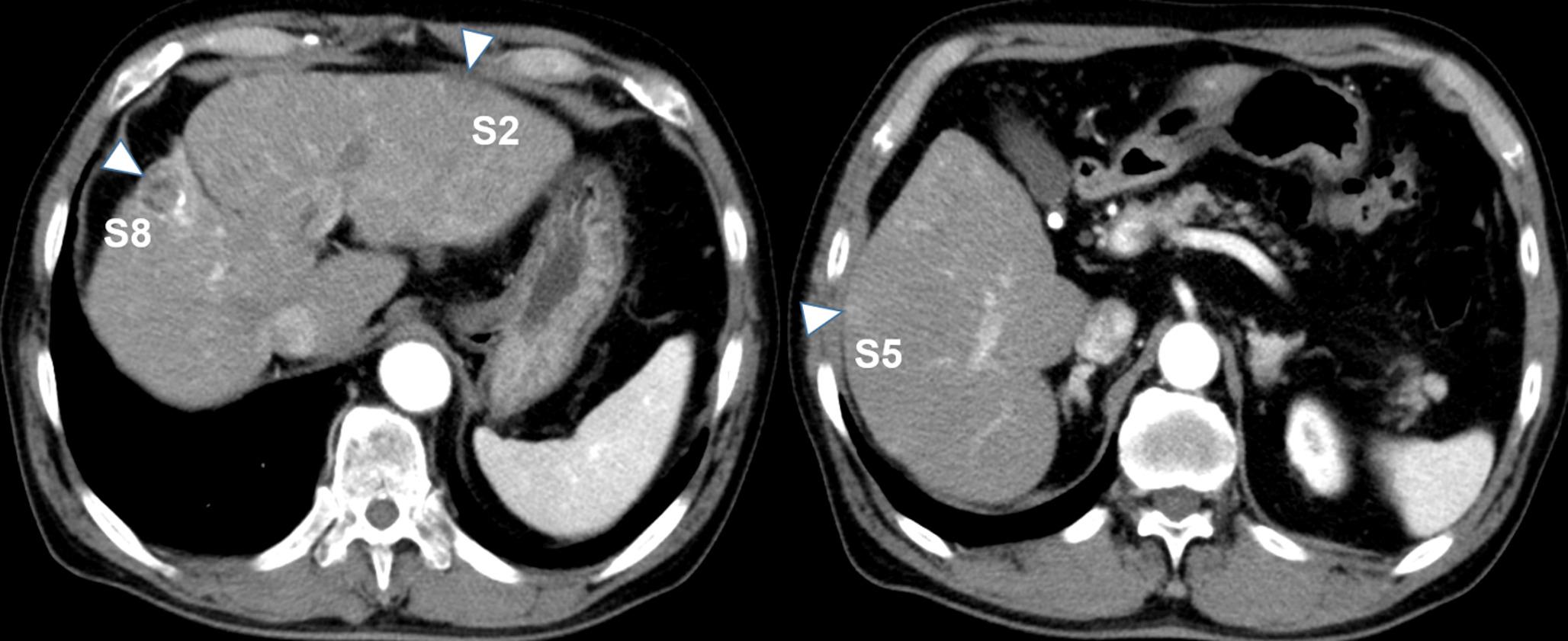
Multiple pulmonary nodules developing during immune checkpoint inhibitor (ICI) therapy pose a broad differential diagnosis that includes infection, vasculitis, malignancy, and immune-related adverse events (irAEs). A 77-year-old man receiving atezolizumab–bevacizumab therapy for recurrent hepatocellular carcinoma developed multiple bilateral pulmonary nodules with surrounding ground-glass opacities (halo sign). Although bronchoalveolar lavage cultured Aspergillus versicolor, fungal markers were negative, and the nodules progressed despite antifungal therapy. Tumor markers for hepatocellular carcinoma were decreasing, and several nodules showed bronchus-penetrating morphology, findings atypical for metastatic lesions. Bronchoscopy was nondiagnostic, consistent with its known limited sensitivity in immune-related pneumonitis. Video-assisted thoracoscopic biopsy revealed organizing pneumonia characterized by intra-alveolar granulation tissue plugs and type II pneumocyte hyperplasia. Corticosteroid therapy resulted in radiographic improvement. Organizing pneumonia is a recognized pattern of ICI-induced pneumonitis and may present with nodular or halo sign–positive lesions, even in asymptomatic patients. This case underscores the importance of considering irAE pneumonitis when multiple pulmonary nodules with the halo sign develop during ICI therapy and highlights the need for surgical biopsy when noninvasive evaluation remains inconclusive.

Comments (0)