
Remember me
Pregnancy with chronic liver disease carries substantial maternal and fetal risks. In cirrhotic patients, the likelihood of hepatic decompensation during pregnancy is markedly elevated, manifesting as ascites, variceal bleeding, or encephalopathy, and is often accompanied by cholestasis and the need for intensive care unit admission [1]. Among these complications, variceal bleeding is a leading cause of maternal mortality and necessitates vigilant risk assessment and management during pregnancy [2].
Acute-on-chronic liver failure (ACLF) is a syndrome defined by acute decompensation in patients with underlying chronic liver disease or cirrhosis, resulting in hepatic and extrahepatic organ failure and high short-term mortality [3, 4]. The acute insults commonly include alcohol abuse, bacterial infection, disease exacerbation, and gastrointestinal hemorrhage [5, 6].
Here, we report a rare case of ACLF precipitated by postpartum esophageal variceal bleeding after cesarean section in a patient with alcohol-associated liver disease (ALD). This case highlights how pregnancy-related hemodynamic changes may worsen portal hypertension and trigger acute decompensation in cirrhosis.
Case reportA 41-year-old woman with long-standing heavy alcohol consumption (approximately 500 g/week since her early twenties) had first been noted to have liver dysfunction at age 25, diagnosed as hepatic steatosis. She developed hypertension at age 35, but despite persistently abnormal liver tests, she did not seek further evaluation.
At age 38, during preconception counseling, laboratory tests again showed elevated aminotransferases (aspartate aminotransferase [AST], 120 U/L, and alanine aminotransferase [ALT], 60 U/L). Ultrasonography demonstrated hepatic steatosis with an irregular liver surface (Fig. 1A, B), and viral and autoimmune liver diseases were excluded. Based on her long-standing alcohol use and these findings, alcohol-associated liver disease (ALD) was diagnosed. Non-invasive fibrosis assessment indicated moderate fibrosis, and she was advised to abstain from alcohol. At age 39, after failing to reduce alcohol intake, she was referred to our department for worsening liver dysfunction. At age 40, esophagogastroduodenoscopy (EGD) showed no esophageal varices, and she subsequently conceived through in vitro fertilization. Her pre-pregnancy body mass index was 24.8 kg/m2, and she successfully abstained from alcohol during pregnancy, which was complicated by hypertension. During pregnancy, the patient was followed by the obstetrics team with biweekly visits. After alcohol abstinence, aminotransferase levels (AST ~ 40 U/L, ALT ~ 20 U/L), total bilirubin (~ 1.0 mg/dL), and platelet counts (~ 14.0 × 104/μL) remained stable. However, hepatic imaging evaluations were not performed during pregnancy.
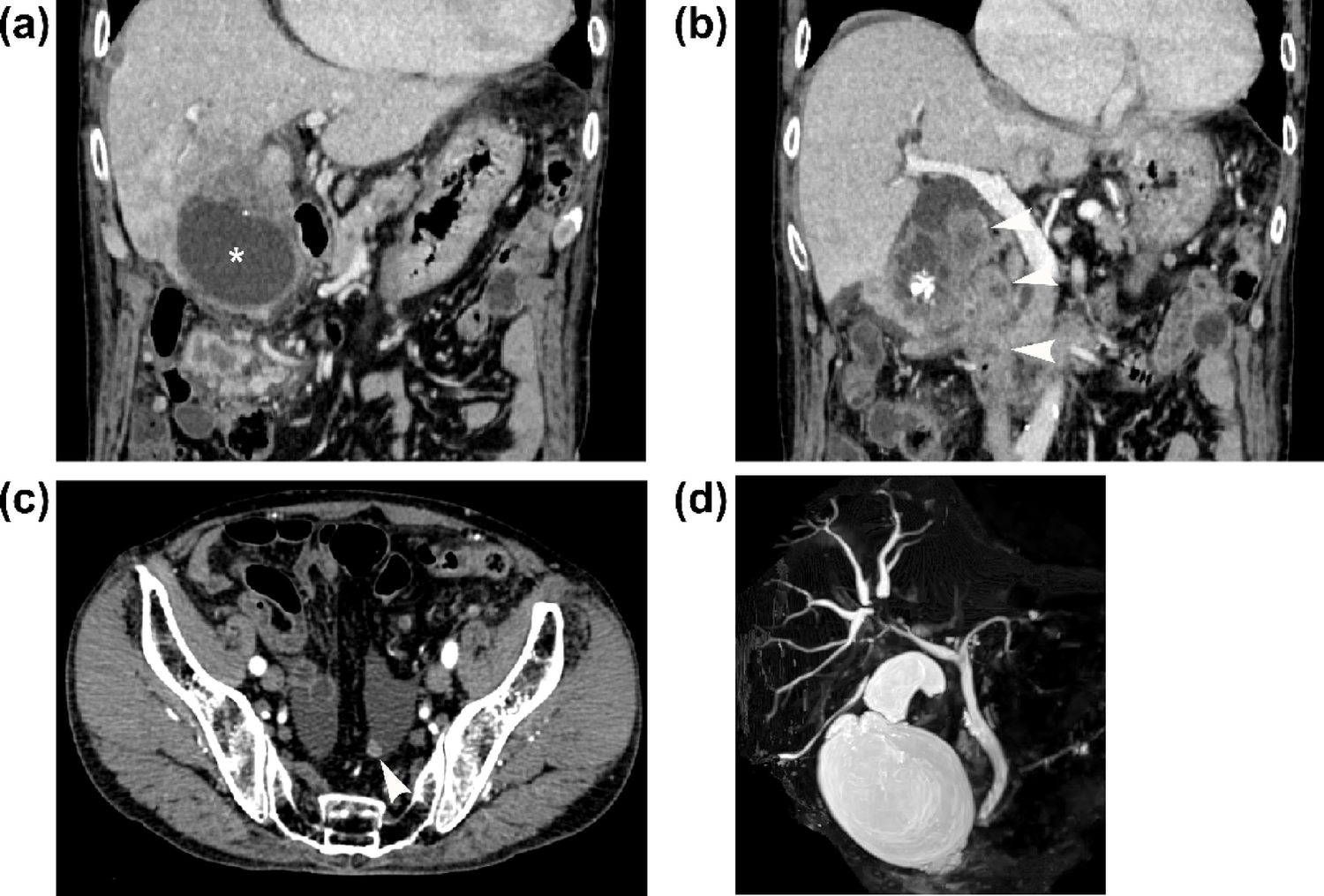
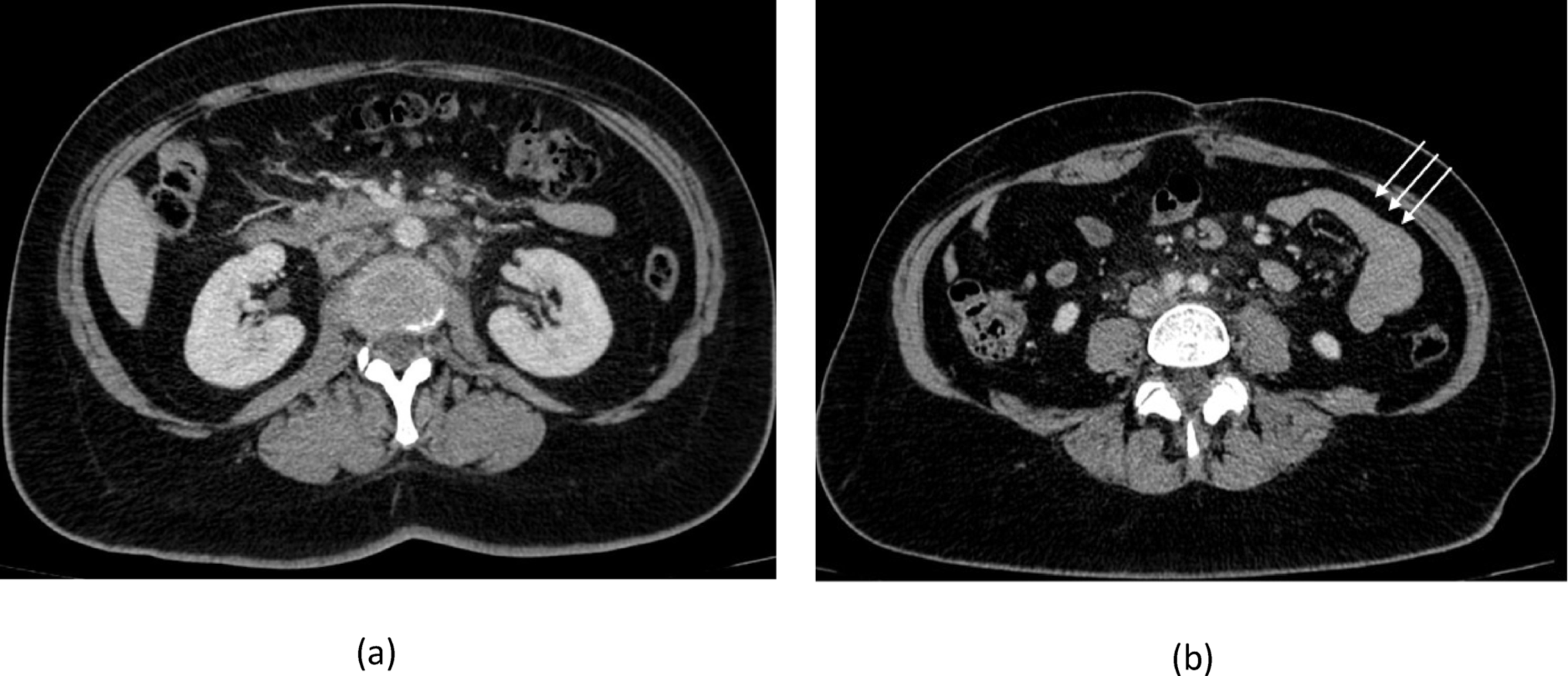
Fig. 1
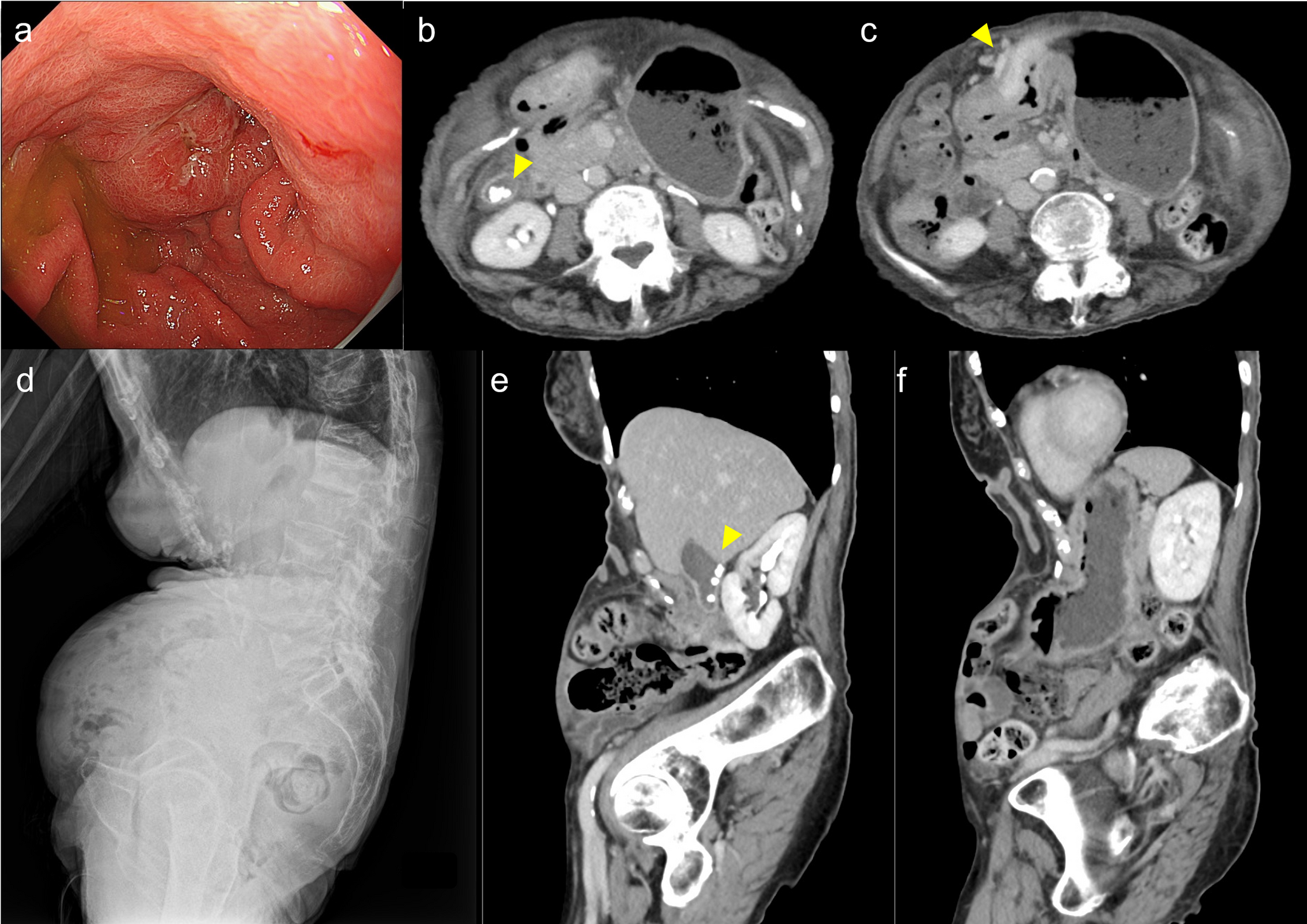
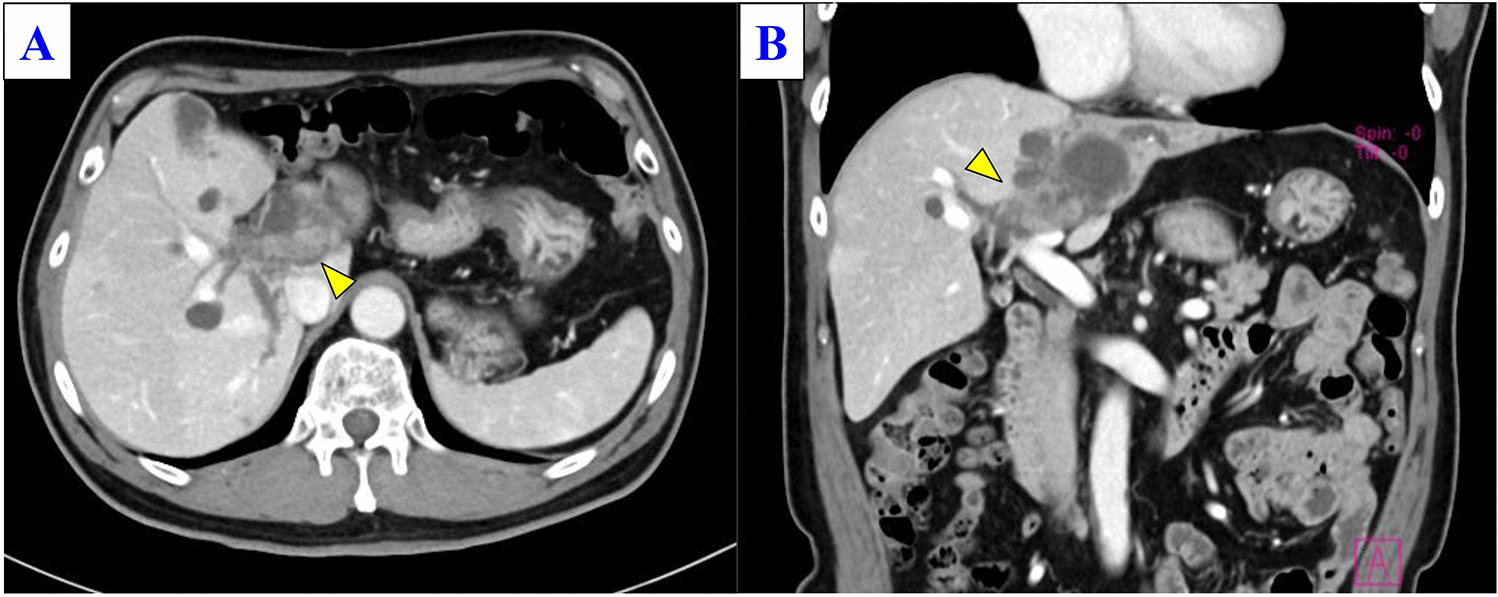
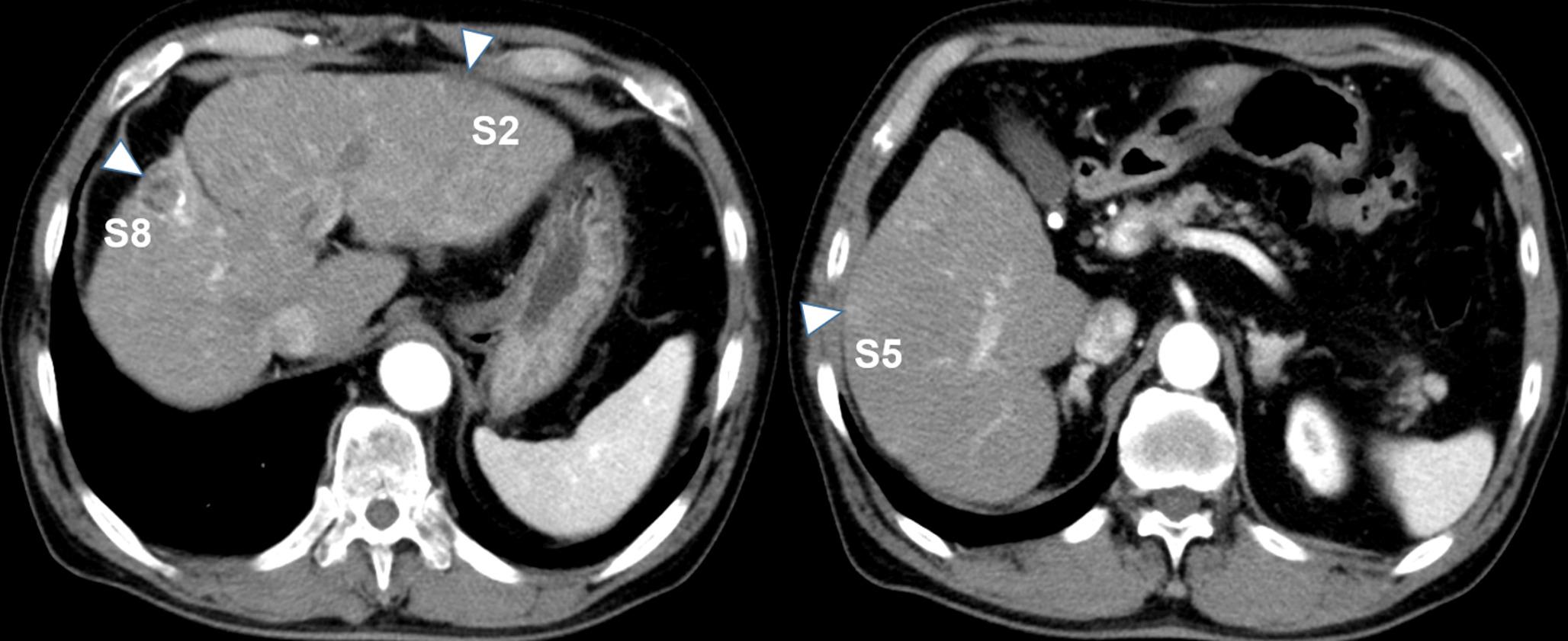
Abdominal ultrasonography and contrast-enhanced computed tomography findings. A, B Ultrasonography three years before admission: A Blunted liver edge with an irregular surface (arrowheads). B Hepatorenal contrast showing increased hepatic echogenicity, consistent with hepatic steatosis. C, D Ultrasonography at referral (hospital day 7): C Irregular liver surface (arrowheads) with coarse parenchymal echotexture. D Moderate ascites (arrows) without evidence of hepatic malignancy. E, F Contrast-enhanced CT on hospital day 8: Dilated vessels in the lower esophagus (arrowheads) without active bleeding
She was admitted for threatened preterm labor and underwent emergency cesarean section on hospital day 4 at 31 weeks and 3 days for superimposed preeclampsia with thrombocytopenia (platelet count approximately 8.0 × 104/μL), without evidence of hemolysis (including normal lactate dehydrogenase levels) or marked elevation of aminotransferases, with an estimated intraoperative blood loss of approximately 1000 mL. The neonate had transient tachypnea. In the early postoperative period, ascites worsened and liver dysfunction persisted (total bilirubin 3.08 mg/dL, and prothrombin time [PT] 53%). She was referred to our department on hospital day 7. At presentation, she was alert but required high-flow nasal oxygen therapy (60 L/min) to maintain an SpO₂ of 93%. Physical examination revealed mild jaundice, abdominal distension, and bilateral leg edema. Laboratory results showed elevated liver enzymes, low albumin (2.4 g/dL), prolonged PT (64.6%), and markedly increased fibrosis markers (FIB-4 2.27, mac-2 binding protein glycosylation isomer 6.76 AU/mL, autotaxin 2.397 mg/L, type IV collagen 7S 39.7 ng/mL) (Table 1). Ultrasonography indicated cirrhosis with moderate ascites but no malignancy or portal vein thrombosis (Fig. 1C, D). Her Child–Pugh score was 11 (class C) and MELD score 12.
Table 1 Laboratory data at referral to our department (hospital day 7)On hospital day 8, she developed hematemesis. Computed tomography (CT) revealed dilated esophageal vessels (Fig. 1E, F), and emergent EGD showed actively bleeding newly developed esophageal varices, which were treated with endoscopic variceal ligation (Fig. 2A, B). On hospital day 10, she developed agitation followed by grade 4 hepatic encephalopathy, with ammonia rising to 138 μg/dL (Table 2). She fulfilled the EASL–Chronic Liver Failure Consortium criteria for ACLF with brain failure and respiratory failure, consistent with the severity of ACLF grade 2 [7, 8]. Comprehensive infection screening to identify potential infectious triggers of ACLF was negative.
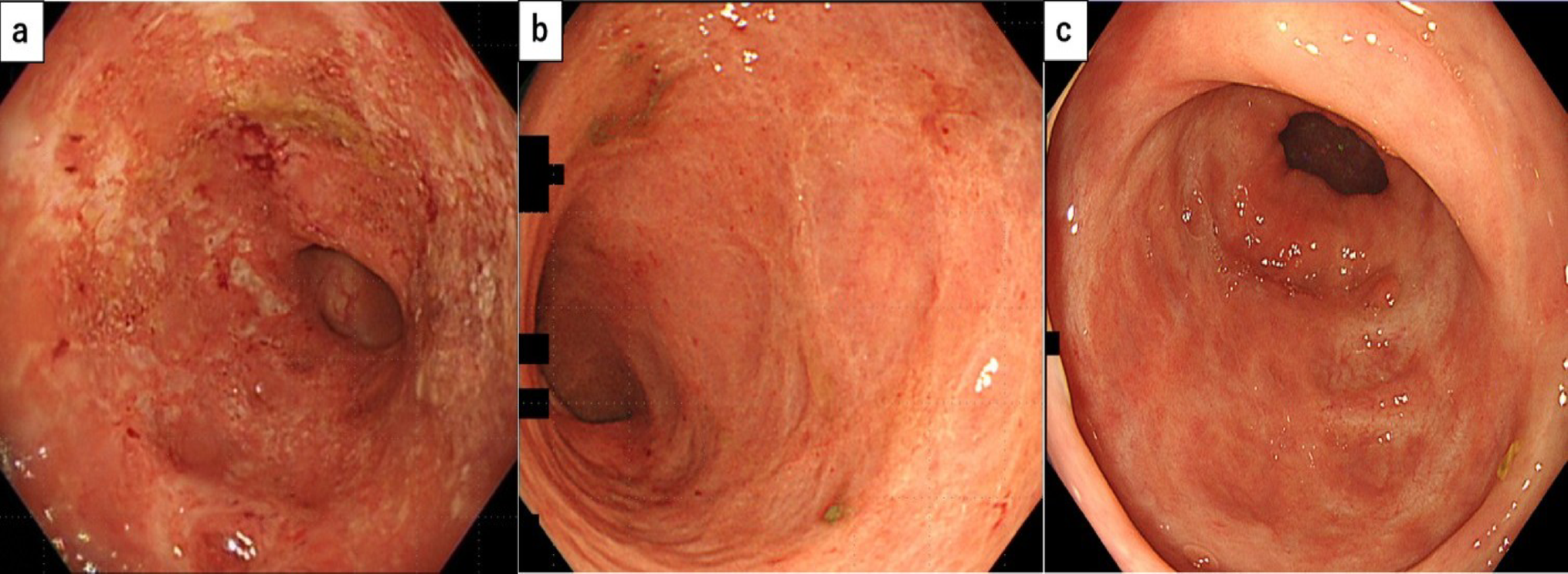
Fig. 2
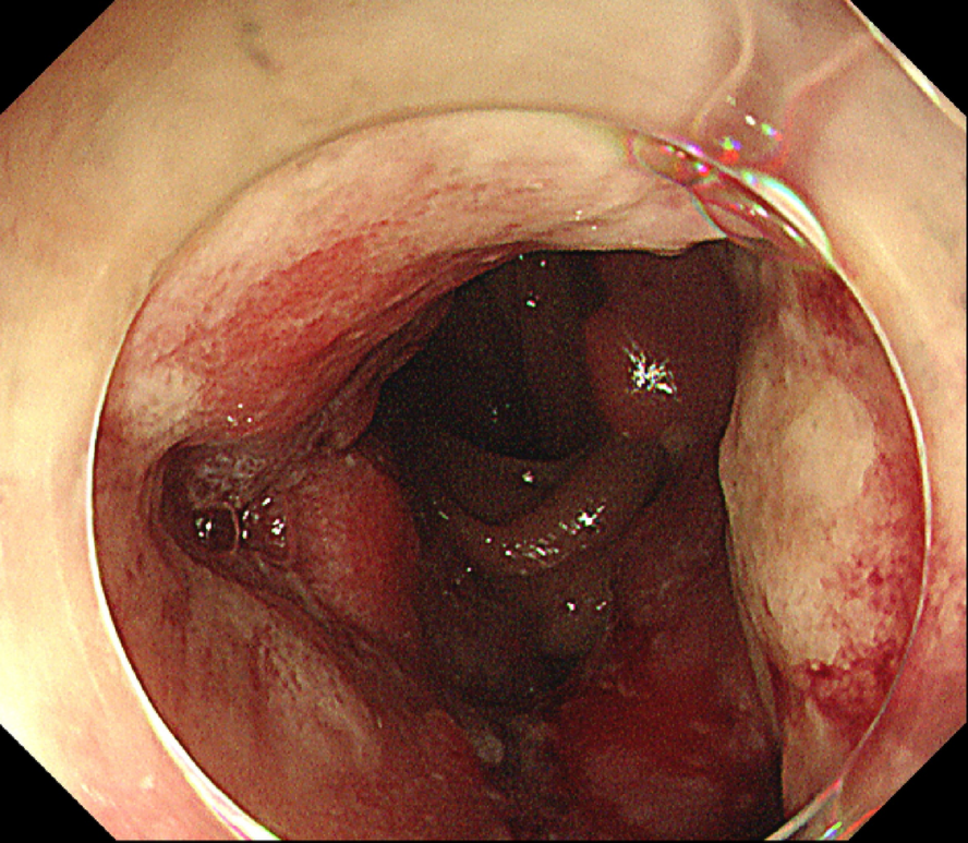
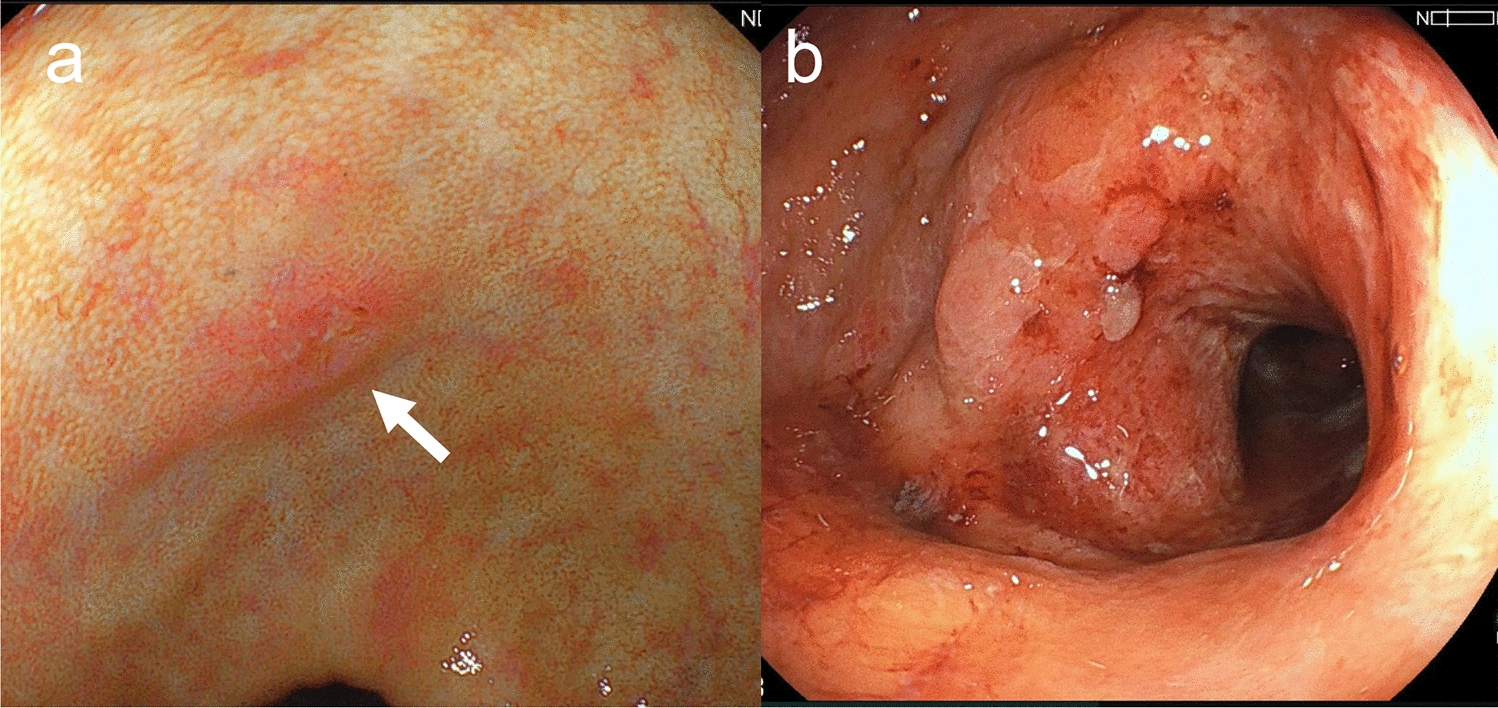
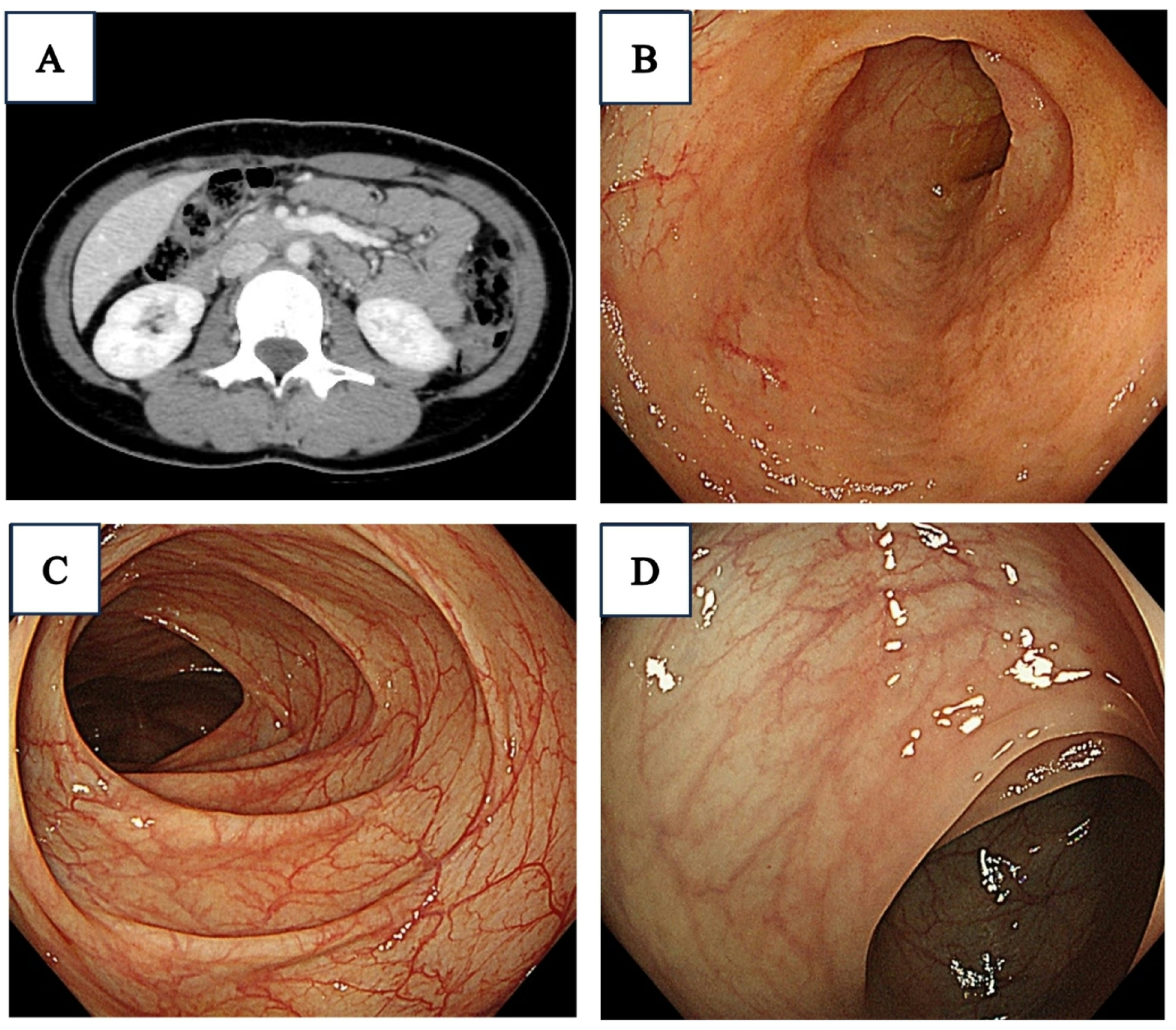
Esophagogastroduodenoscopy. A, B Endoscopy on hospital day 10 showing active bleeding from lower esophageal varices, with hemostasis achieved by endoscopic variceal ligation. C, D Follow-up endoscopy on hospital day 21 showing no lesions requiring treatment (Li, F1, Cb, RC0)
Table 2 Laboratory data at the time of ACLF diagnosis (hospital Day 10)On hospital day 11, she remained comatose with ammonia 177 μg/dL. Brain CT was unremarkable. Therapeutic plasma exchange and hemodiafiltration were initiated to manage encephalopathy and prevent multi-organ failure, while liver transplantation remained a contingency. Her neurological status improved progressively—grade 3 on day 12, grade 1 on day 15, and full recovery by day 22. Ammonia levels and ascites decreased, and hemodiafiltration was discontinued on hospital day 17. Her respiratory status gradually improved, and supplemental oxygen was discontinued. Follow-up EGD on hospital day 21 showed small residual varices without high-risk stigmata (Li, F1, Cb, RC0) (Fig. 2C, D). She was discharged home on hospital day 28 with reinforcement of strict alcohol abstinence and psychiatric support (Fig. 3). The neonate recovered well and was discharged on day 60.
Fig. 3
Clinical course of the patient. BCAA, branched chain amino acids; EGD, esophagogastroduodenoscopy; EVL, endoscopic variceal ligation; HE grade, hepatic encephalopathy grade; iv, intravenous; NH3, ammonia; po, per oral; PT, prothrombin time; TPN, total parenteral nutrition
Comments (0)