
Remember me
A 70-year-old woman was referred to our hospital after multiple liver tumors were detected during a routine health examination. She had no specific symptoms at presentation. Based on liver biopsy findings, she was diagnosed with NET G2 liver metastases. Her medical history included an untreated left pharyngeal pleomorphic adenoma, which was confirmed on review at our pathology department. Additionally, a cardiac pacemaker was inserted to treat a complete atrioventricular block.
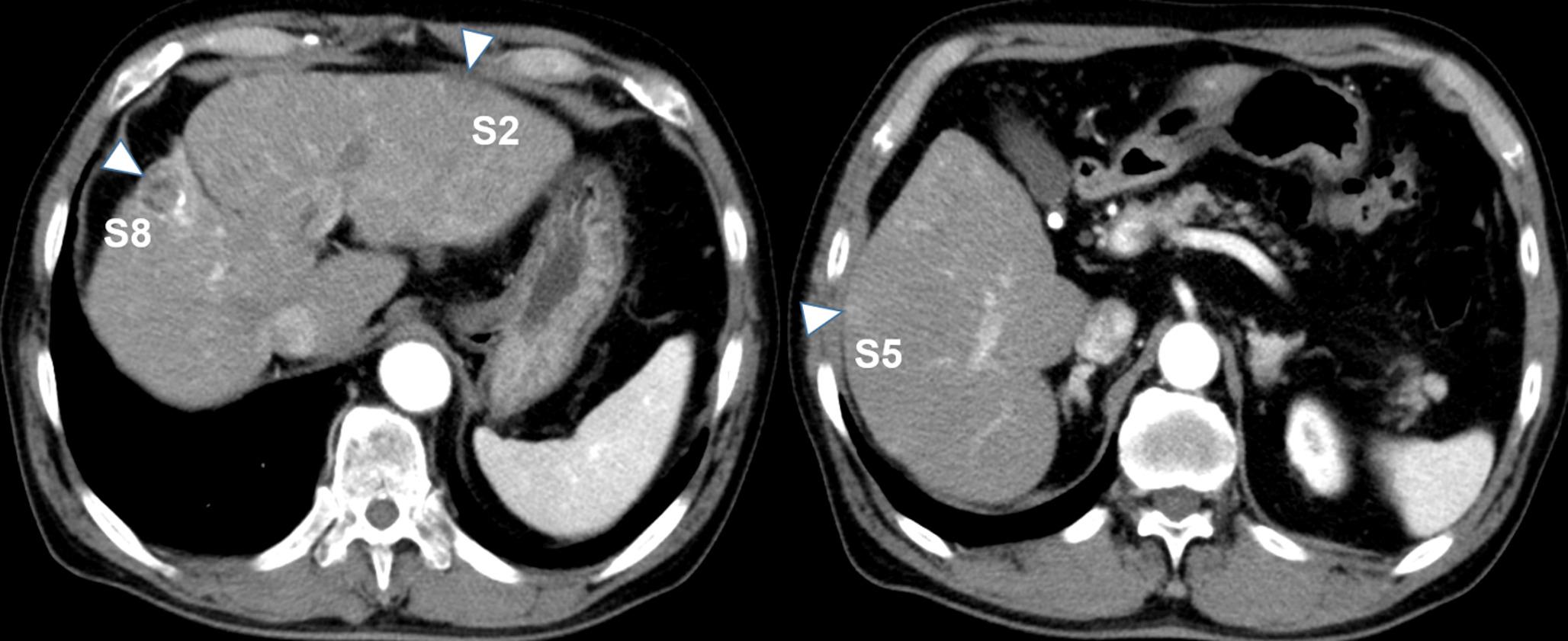
Initial evaluation with upper and lower gastrointestinal endoscopy and contrast-enhanced CT failed to identify the primary lesion. As the liver metastases were confined to the right lobe (Fig. 1a, b, arrowheads: tumor area), right hepatectomy was performed with curative intent. Histopathological examination revealed tumor cells with round to oval nuclei arranged in trabecular and insular patterns, indicating expansive growth. Immunohistochemically, the tumor was positive for synaptophysin and negative for chromogranin A. With a Ki67 labeling index of 20.6%, the diagnosis was revised to NET G3.
Fig. 1
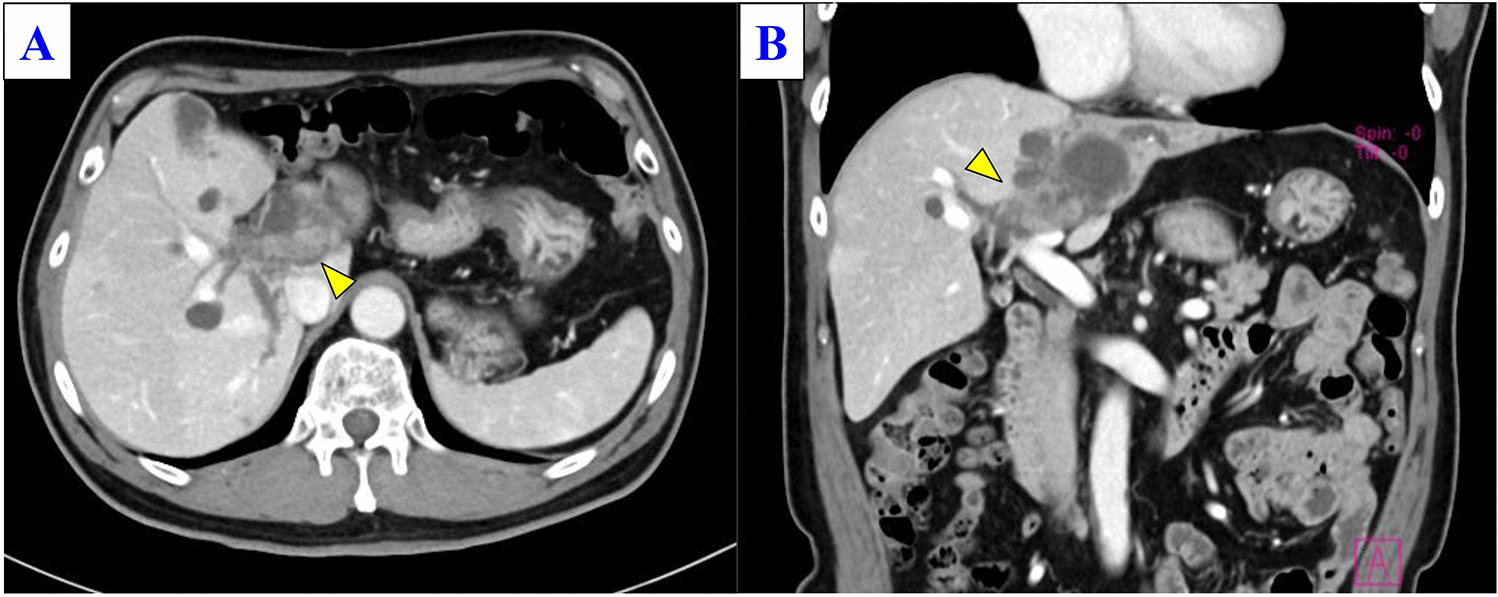
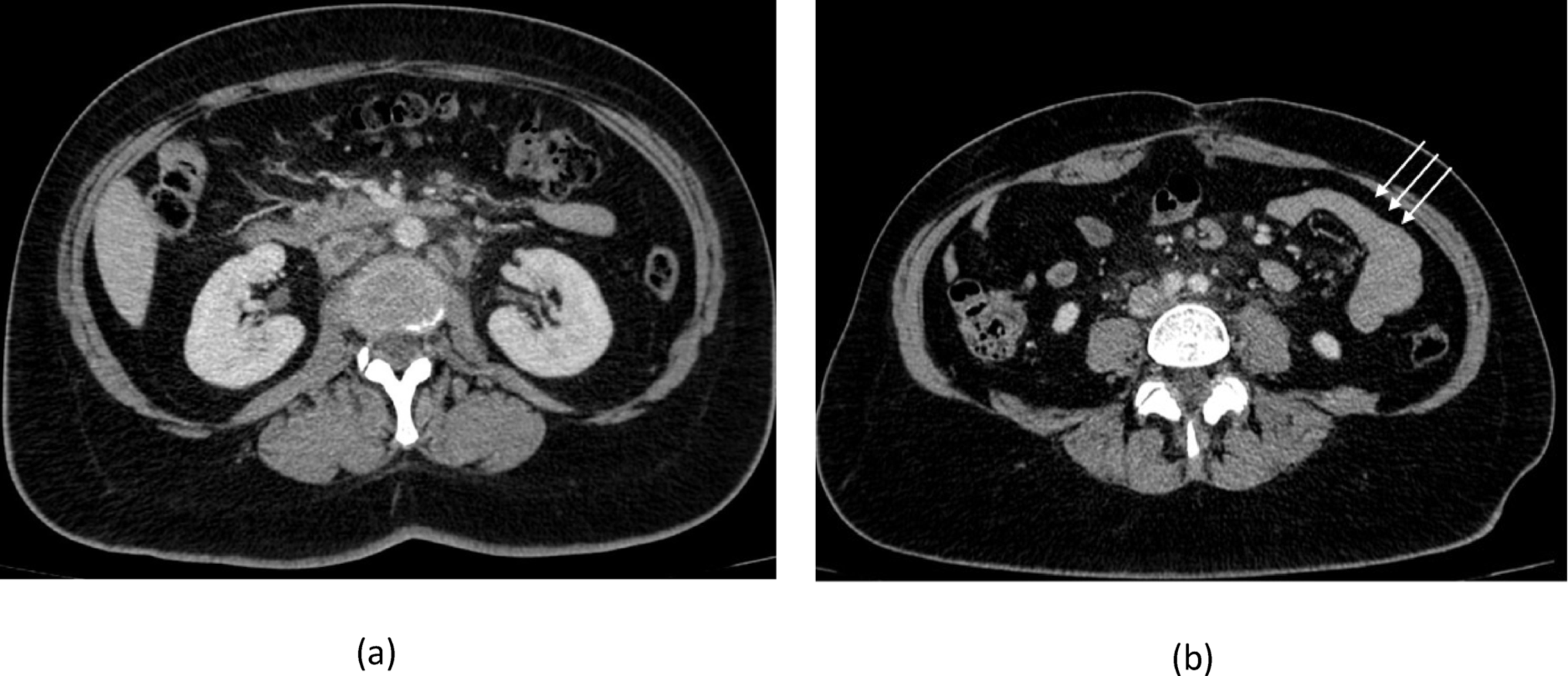
Dynamic computed tomography (CT) images at the arterial phase upon referral to our hospital. a A coronal image showing a low-attenuation area in segment 7 of the right hepatic lobe (arrowhead). b An axial image showing a low-attenuation area in segment 5 of the right hepatic lobe (arrowhead)
Post-hepatectomy follow-up imaging showed no evidence of new lesions. However, 68 Ga-DOTATOC PET/CT, performed to evaluate potential residual disease at another hospital, revealed an uptake in the perirectal region and at the site of the known left pharyngeal pleomorphic adenoma. Subsequently, a detailed medical history of the perirectal lesion revealed that the patient had undergone endoscopic mucosal resection (EMR) of a rectal carcinoid tumor at a local clinic 10 years prior to the current presentation. Review of the endoscopic images from the initial EMR revealed a tumor measuring 17 × 15 mm, with pathological findings indicating uncertainty regarding the completeness of resection. Although the original specimen was unavailable for WHO 2019 classification review, we clinically diagnosed the liver lesions as metastases from the rectal NET. Contrast-enhanced CT revealed a 5-mm lymph node corresponding to the perirectal uptake area identified on DOTATOC-PET/CT, which was considered to be local recurrence after EMR.
Given the recurrence of NET in both local and liver sites 10 years after initial endoscopic treatment, we initiated systemic therapy before rectal and perirectal lymph node resection. Specifically, daily treatment with 10 mg of everolimus was initiated. After 12 months of stable disease, the patient underwent laparoscopic intersphincteric resection with D2 lymph node dissection and lateral pelvic node dissection. Pathological examination revealed NET metastases in lymph nodes #251 (Ki67 20.5%, NET G3) and #263 (Ki67 15%, NET G2); however, no residual tumor was found in the rectum.
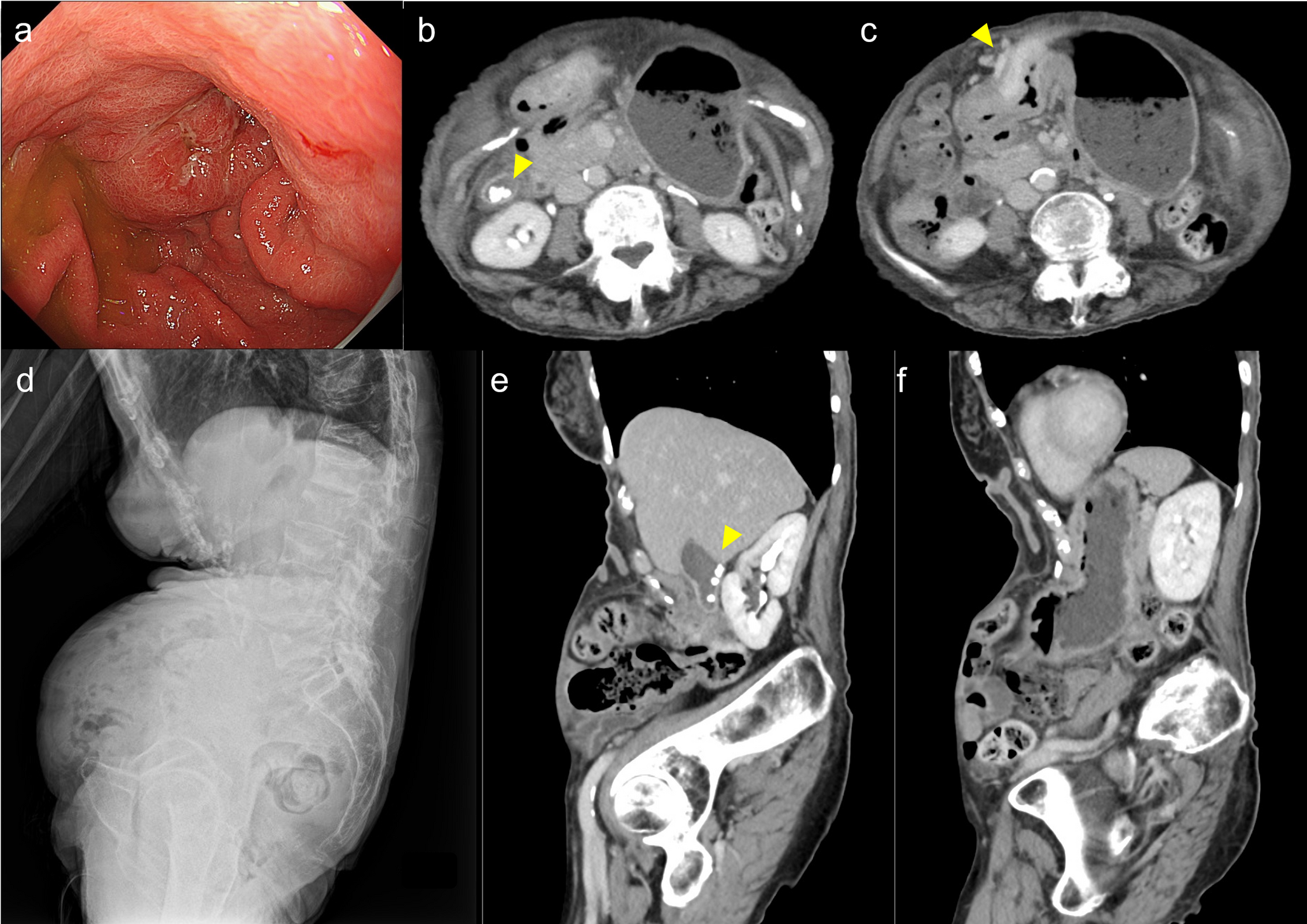
Two years and five months after rectal surgery, the patient developed diplopia. Contrast-enhanced CT revealed a tumor in the left-orbital medial rectus muscle region, a lesion adjacent to the right ventricle, and an ovarian lesion. (Fig. 2a, b, c, arrowheads: tumor area). Somatostatin receptor scintigraphy (SRS) showed an uptake by these lesions (Fig. 2d, e, f) and by the known pharyngeal pleomorphic adenoma (Fig. 2 g, arrowheads: tumor area, 2 h). To determine whether the orbital lesion originated from a NET metastasis or from the known pharyngeal pleomorphic adenoma [6], orbital biopsy was performed, confirming NET metastasis (Ki67 19.8%, NET G2; Fig. 3a, b, c, d, e).
Fig. 2
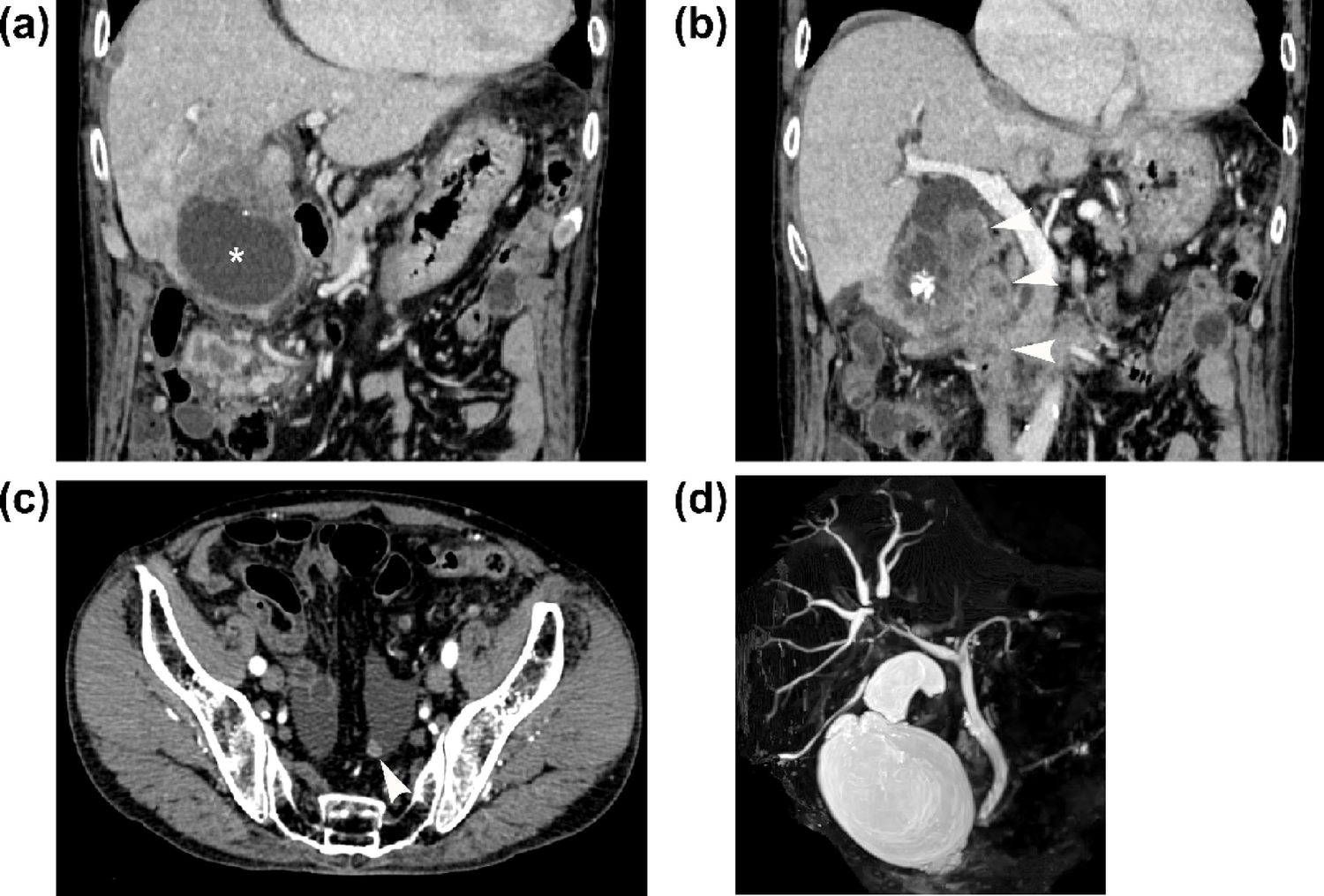
Imaging findings of the systemic lesions. a–c Dynamic CT images: a Head axial view, b chest and abdomen coronal view, and c pelvis axial view. Arrowheads indicate an enhancing mass in the left medial rectus muscle, a small nodule adjacent to the right ventricle, and a faintly enhancing nodule in the left ovary, respectively. d–f SRS: Images correspond to sections (a), (b), and (c). Each lesion identified on CT shows somatostatin receptor expression. g Enhanced head CT (axial view): The arrowhead indicates a known pleomorphic adenoma. h SRS (head, axial view): Significant uptake is noted in the pleomorphic adenoma, corresponding to the CT finding in g
Fig. 3
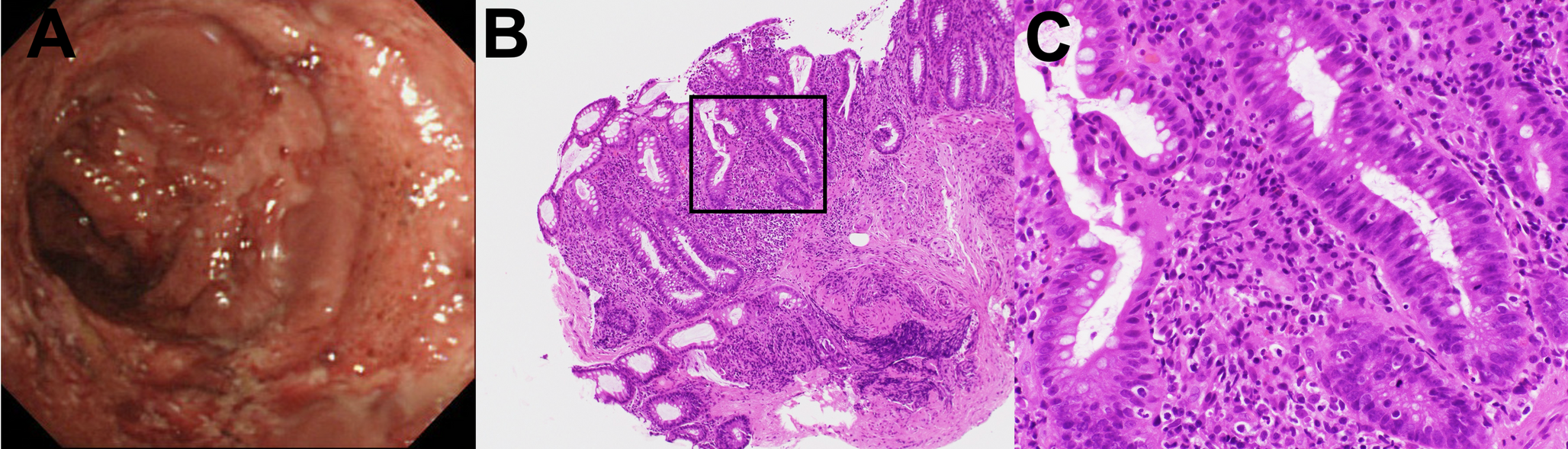
Histopathological findings of the orbital mass biopsy. a Low-magnification hematoxylin and eosin (H.E staining) image: An overview of the biopsy specimen. b High-magnification H.E image: The tumor shows nested growth of relatively uniform cuboidal epithelial cells. c Synaptophysin staining: Low-magnification image of the section corresponding to (a). d High-magnification image of Synaptophysin staining e Ki-67 immunohistochemistry: The Ki-67 labeling index is 19.8%
Considering the multiple metastatic sites and the need to preserve visual function, systemic therapy with everolimus and lanreotide was initiated. The decision to combine these agents was based on the development of new metastases despite prior everolimus treatment and the positive octreotide uptake in the lesions. Tumor response was evaluated according to RECIST version 1.1 criteria after three months of treatment. The orbital lesion showed a complete response (Fig. 4a, b), the right ventricular mass remained stable, and the ovarian lesions progressed (Fig. 4c). Surgical resection of the ovarian metastases revealed NET G3 (Ki67 30.1%). Four months after ovarian surgery, the right ventricular mass showed slight progression (Fig. 4d). Cardiac surgery achieved complete resection of the lesion, which was confirmed as NET G2 (Ki67 15%) (Fig. 4e, f).
Fig. 4
Follow-up imaging and histopathological findings after initiation of everolimus and lanreotide. a Head CT (axial view): The previously observed tumor in the left medial rectus muscle has disappeared. b SRS (head, axial view): Corresponding to (a), no somatostatin receptor uptake is identified in the orbital region. c Enhanced CT of the pelvis: The ovarian lesion shows a clear increase in size (arrowhead). d Enhanced CT of the chest and abdomen: The lesion adjacent to the right ventricle shows a slight tendency toward enlargement (arrowhead). e Histopathology of the cardiac lesion (H.E staining): The tumor has invaded the right ventricular myocardium. It shows nested growth of cuboidal tumor cells with subround nuclei, consistent with metastasis from a neuroendocrine tumor. f Ki-67 immunohistochemistry: The Ki-67 labeling index is 15%
Six months after cardiac surgery, the patient developed pancreatic, adrenal, and bone metastases. Treatment was switched to PRRT, which became available in Japan at that time. After three years of PRRT, the patient continues to display a complete response of the orbital lesion, no recurrence at ovarian or cardiac sites, and stable disease in other metastatic sites, while maintaining ECOG PS 0 and continuing regular work activities. Throughout the 10-year clinical course following the initial right hepatectomy, the patient remained free of recurrent liver metastases.
Comments (0)