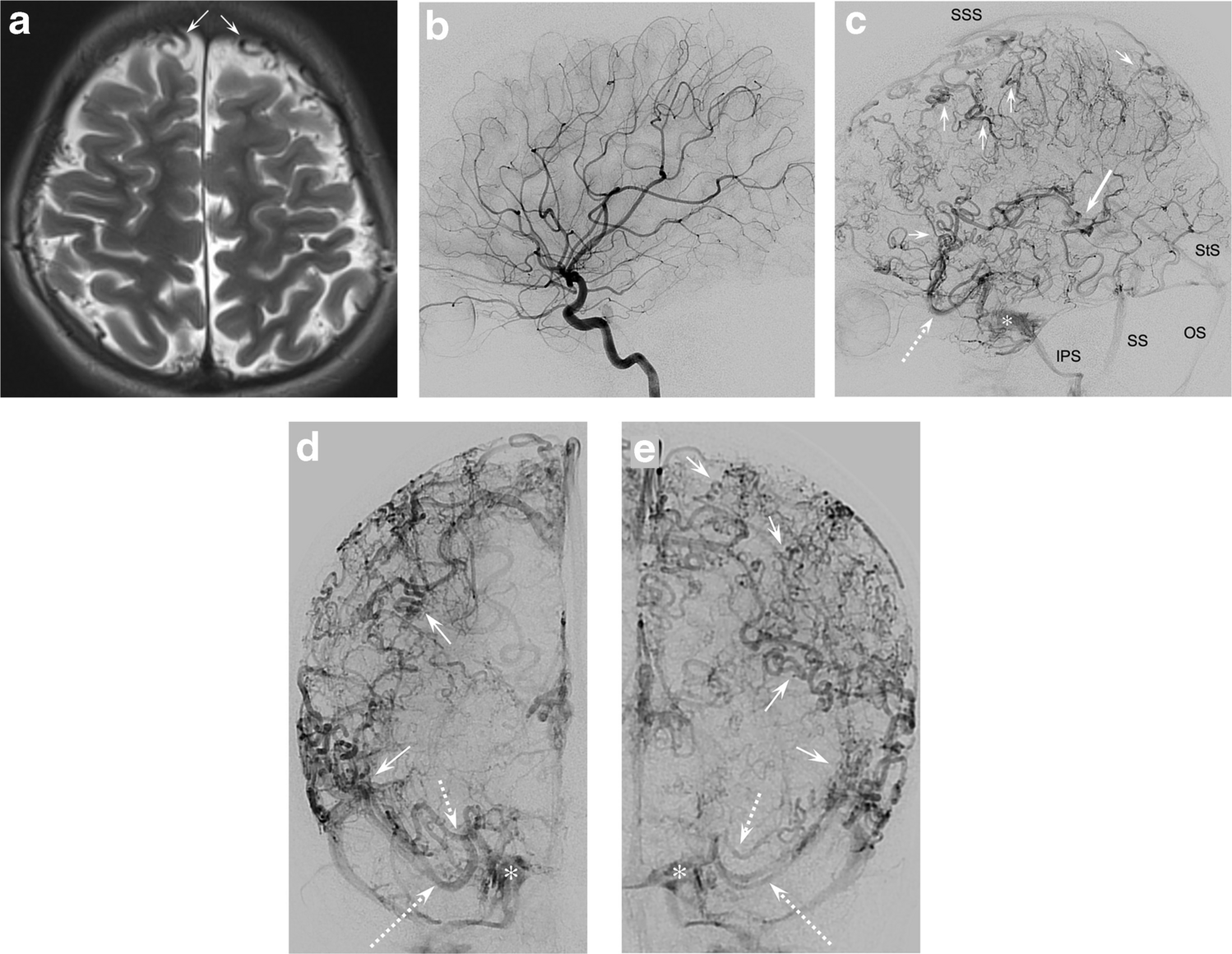
We present a unique case of severely maldeveloped cerebral venous system consisting of extensive tortuosities involving pial and small cortical veins in the absence of arteriovenous shunting and associated with a partial absence or maldeveloped deep venous system. These findings are highly unusual and have been described only in one, somewhat similar, case by Voronovich et al. [3]. The authors observed a 16-year-old boy with developmental delay who presented with seizures, intracranial hypertension, and stroke-like episodes. Angiography showed markedly tortuous small- to medium-sized cortical veins, while the deep venous system, including the vein of Galen and straight sinus, could not be identified. Due to signs of delayed venous outflow on digital subtraction angiography, the presence of intracranial calcifications, and diffusion restriction in the subcortical white matter, suggestive of ischemic changes, the term restrictive cerebral cortical venopathy was proposed. Differently, no imaging findings of venous outflow restriction or ischemia were present in our patient. Further, while both basal veins of Rosenthal were absent in their second and third segments, and the left internal cerebral vein was incompletely developed and tortuous, the vein of Galen and straight sinus were patent. On the other hand, both transverse sinuses were absent, and the main deep and cortical venous drainage was directed towards the cavernous sinus and through a normal-sized superior sagittal sinus into two large occipital sinuses.
The most striking finding in our patient were numerous highly unusual 360° coilings of the pial and small cortical veins, a feature not described in the literature so far. The connection from the malformed pial and small cortical veins to the large cortical and bridging veins was difficult to clearly visualize, even on venous 3-D digital subtraction angiography. Whether or not the seemingly reduced number of large cortical veins is directly related to the abnormal appearance of the pial and small cortical veins remains unclear. Similarly, other findings, including the tortuous tributaries to the inferior sagittal sinus, and either tortuous or entirely missing segments of the deep venous system, could not easily be attributed to a reduced number of large cortical veins. We observed some, but not a significant number, of compensatory dilated transcerebral and anastomotic medullary veins as discussed by Voronovich et al. [3].
Overall, the exact causality of the observed abnormalities involving both deep and superficial veins as well as dural sinuses remains difficult to determine. Such cerebral venous dysgenesis without evident outflow restriction would likely be related to a broader developmental failure of the cerebral venous system rather than to an event at a specific stage of embryonic development [3, 4]. In the literature, a few patients with malformed venous systems in the spectrum of cerebral venous dysgenesis have been reported; all of them were symptomatic, and none demonstrated the findings detailed in this report [5,6,7]. Notably, our patient had no seizures or focal neurological symptoms but had a history of infantile autism, attention deficit disorder, and dyslexia. Considering that our patient had no symptoms due to venous ischemia and an otherwise normal brain MRI, it remains debatable whether the presented case is consistent with a true pathological condition or should be regarded as an extremely rare variant of normal.
A complex chromosomal rearrangement involving three chromosomal segments, reflecting a phenomenon called chromotripsis, was found in our patient. Isolated, none of the aberrations is associated with disease, but a positional effect of the duplications cannot be ruled out, as known in other cases with chromotripsis [8]. It is also possible that this genetic finding is purely incidental without clinical consequence. Nevertheless, pediatric neuroradiologists and neurologists should be aware that patients with cerebral venous dysgenesis may benefit from genetic testing. More cases and data, including a detailed assessment of the venous anatomy using advanced vascular 3-D imaging, need to be collected to better understand these rare anomalies and their clinical importance.



Comments (0)