Of the odontogenic cysts, OKC is one of the most challenging ones. It is sufficiently common, has a relatively high rate of recurrence if not completely removed, and can have outgrowths, daughter cysts making it difficult to be removed in toto. Although OKCs have clinical and radiological features allowing for a clinical suspicion or diagnosis, there are other lesions with overlapping qualities, therefore a histological confirmation of the diagnosis is always required. On the other hand, although OKCs have a typical histological appearance (Fig. 2 M, N, O), these characteristics may be completely or largely lost in association with secondary inflammation. This is why combination of clinical, radiological and pathological findings are optimally needed for the proper diagnosis of the lesions. This combination of data was missing in a number of cases for the original reports, and was compensated for by the clinical, radiological and pathological review of all available data from the patients’ charts. This review of each individual case is a special strength of this study.
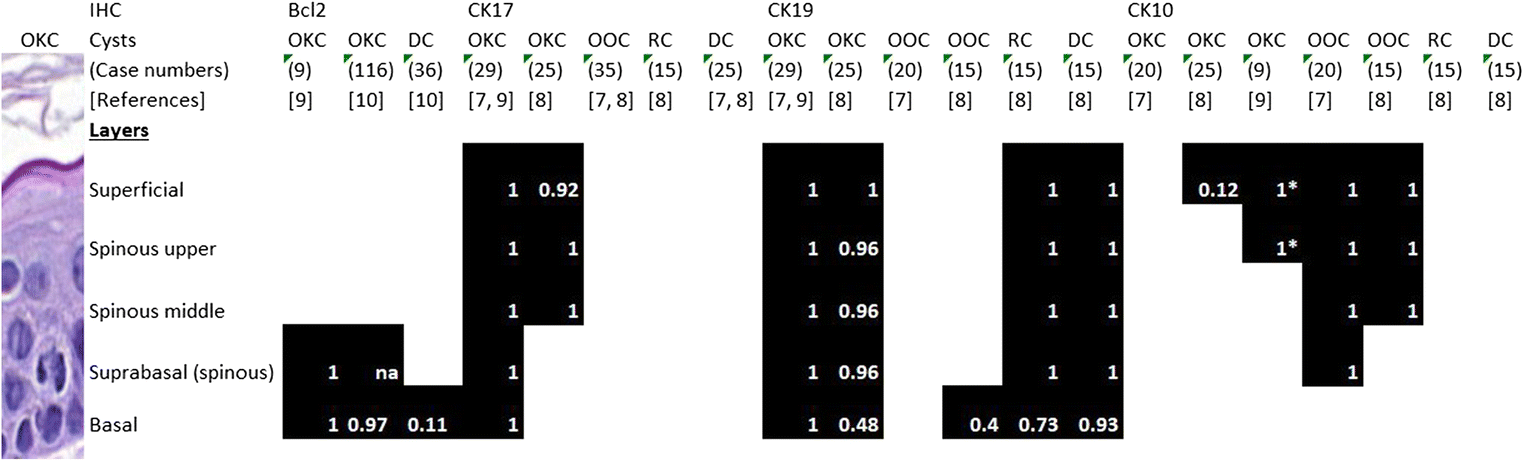
The distinctive CK17 and bcl2 IHC of OKCs consists of a strong transepithelial CK17 positivity (with or without focal basal or superficial sparing) and a strong basal (with or without weaker suprabasal) bcl2 positivity (Fig. 1, Fig. 2 M, N, O) [7,8,9]. Meara et al. have suggested that a strong CK17 positivity in all layers may point to syndromic OKCs, although they noted similar staining in 2/7 of their sporadic OKC cases as well; they also reported focal or only basal or only superficial CK17 labelling in 4/7 non-syndromic OKCs [11]. In keeping with these results, syndromic OKCs generally had strong CK17 staining, but sporadic cases also displayed similar intensities; in contrast, some areas displayed superficial sparing with CK17 in two OKCs from Gorlin-Goltz syndrome patients. Focal basal sparing was also seen in a few OKCs of this series, but all 20 cases studied with typical epithelium had marked transepithelially stained areas.
Secondary to inflammation, an altered epithelium may replace the typical lining of OKCs, and this is characterized by the loss of the typical IHC staining profile as well, although focal (transitional or typical) areas with typical IHC staining may remain and can be helpful in the diagnosis [9]. Twenty of the 21 OKCs of this consecutive series had the typical epithelium and IHC profile at least focally, whereas in one case, the epithelium was completely replaced by a non-specific squamous one lacking the typical IHC staining of OKCs; its diagnosis was established as being most consistent with an inflamed OKC on the basis of clinical and radiological data (Fig. 3). Marsupialization also leads to secondary inflammation, and loss of the typical basal bcl2 staining was interpreted as a sign of treatment effect in OKCs [12].
In contrast to the results of the detailed cytokeratin profiling studies by Aragaki [7] and Tsuji [8] comparing other common odontogenic cysts with OKCs (Fig. 1), many, though not all radicular and dentigerous cysts were not completely negative for CK17, but demonstrated some kind of staining (superficial layer, spinous layer, basal or even focal transepithelial labelling). This was never very strong, but small biopsies obtained during cystostomies may yield a confounding piece of epithelium with OKC-mimicking transepithelial CK17 staining. Others have also reported at least focal CK17 labelling in (some) dentigerous cysts, including the superficial layer staining often observed in the present study [11, 13,14,15]. Although a study by Zivkovic and colleagues looking at 30 dentigerous cysts reported transepithelial staining in these, using the same E3 clone CK17 antibody as in the present study (although from another manufacturer) [16], their results are in contradiction with our and others’ findings [7, 8, 11, 13,14,15]. In contrast to previous reports on the lack of expression of CK17 in radicular cysts [8, 16], the present study also found at least focal CK17 positivity in 25/34 radicular cysts. In concordance with the present results, non-transepithelial CK17 staining of the epithelium of some radicular cysts weaker than in OKCs was reported by Stoll et al. [13].
Basal bcl2 labelling was not common in non-OKCs, but was also seen in some other cyst types, most commonly in dentigerous cysts. Several studies have examined the bcl2 staining of OKCs versus other cysts, with the aim of substantiating the neoplastic nature of the former. For example, Piattelli et al. found bcl2 positivity (defined as >10% staining) in only 1/20 dentigerous cysts, and their 20 radicular cysts were all negative, in contrast to the 20 OKCs studied and unanimously showing basal bcl2 labelling. The authors not only proposed that bcl2 could play a role in the aggressive growth of OKCs, but believed that this was also useful as a diagnostic tool [17]. Similar results were reported by others, and finally a recent systematic review concluded that bcl2 positivity was so much greater in OKCs than dentigerous cysts, that it should be partly responsible for the active growth of OKCs through the inhibition of apoptosis, and therefore be a phenomenon in support of the neoplastic nature of OKCs [10]. However, the systematic review included only 36 dentigerous cysts and 4 of these (11%) showed bcl2 positivity [10]. Our study concentrated more on diagnostic uses of staining patterns rather than quantifying the cells stained. As a consequence, we were interested in any staining pattern that could mimic the typical basal positivity of OKCs, even if this was focal. In fact, bcl2 positivity was never as strong and diffuse in other cyst types, but there were some cysts that clearly exhibited continuous basal layer bcl2 labelling of weak to moderate intensity; these were predominantly developmental cysts, mostly dentigerous cysts (8/16 non-OKCs with basal bcl2 labelling), but radicular cysts (especially mature ones with atrophic epithelium) were also identified as having this staining pattern. Our findings are reinforced by the findings of Martins et al., who also found some basal bcl2 expression in non-inflamed radicular cysts although this was less common than that seen in similarly atrophic dentigerous cysts [18]. These authors also proposed that inflammation may inhibit bcl2 expression and therefore contribute to similarities of inflamed cysts of radicular and dentigerous origin. This suggestion may probably be generalized to most inflamed cysts with non-specific squamous epithelium.
The association of a strong basal bcl2 and significant transepithelial CK17 stainings in the same areas of non-OKC was not encountered in this series, but cannot be completely excluded on the basis of the number of cases studied.
The consecutive series (on the basis of the clinicopathological diagnoses), as could be expected, contained mainly the commonest odontogenic cysts, i.e. radicular cysts, dentigerous cysts and OKCs. The latter were slightly overrepresented because of surgeries on 4 patients with the Gorlin-Goltz syndrome and up to 5 OKCs removed from these patients. However, the series also included a few rarer cysts like a paradental cyst (inflammatory collateral cyst) (K17), one botryoid odontogenic cyst (K9), one nasopalatine duct cyst (S38) and lateral periodontal cysts (K7, K16, K22). Of these, the developmental cysts without inflammation demonstrated some (faint to moderate) basal bcl2 staining, without suprabasal extension, and all of the rarer cyst types also displayed various CK17 expression, including focal transepithelial staining (Fig. 4, Supplementary material). None of these created differential diagnostic problems regarding OKC. In fact, the basal bcl2 seen in some dentigerous and botryoid cysts suggests that this pattern may be more common in developmental cysts. A strong bcl2 expression was also described in a botryoid odontogenic cyst reported recently, being the only case studied in this respect we could identify [19].
To summarize, the study strengthens that the strong diffuse transepithelial CK17 and basal bcl2 are typical of OKCs, but also highlights that these patterns of staining, although to a lesser intensity and extent, can be seen in other odontogenic cysts, too. This is in contradiction with some previous publications referring to the CK17 negativity of radicular and dentigerous cysts [7, 8]. Although the characteristic CK17 and bcl2 IHCs are rare in combination in non-OKCs, inflamed OKCs also loose these stains at the sites of altered epithelium, which may form the majority or the whole of the cyst lining. Therefore, these IHC patterns cannot serve as a yes or no alternative of the clinicopathological diagnostic steps of OKCs, but are rather adjuncts that can serve in some difficult cases. The present experience suggests that they have limited value in the differential diagnosis. The only cyst (K2) where the IHC helped to make the diagnosis of OKC was an inflamed OKC with a small bit of transitional epithelium with basal bcl2 and patchy transepithelial (non-typical) CK17 staining and minimal typical residual epithelium identified only on revision and recut.

Comments (0)