
Remember me



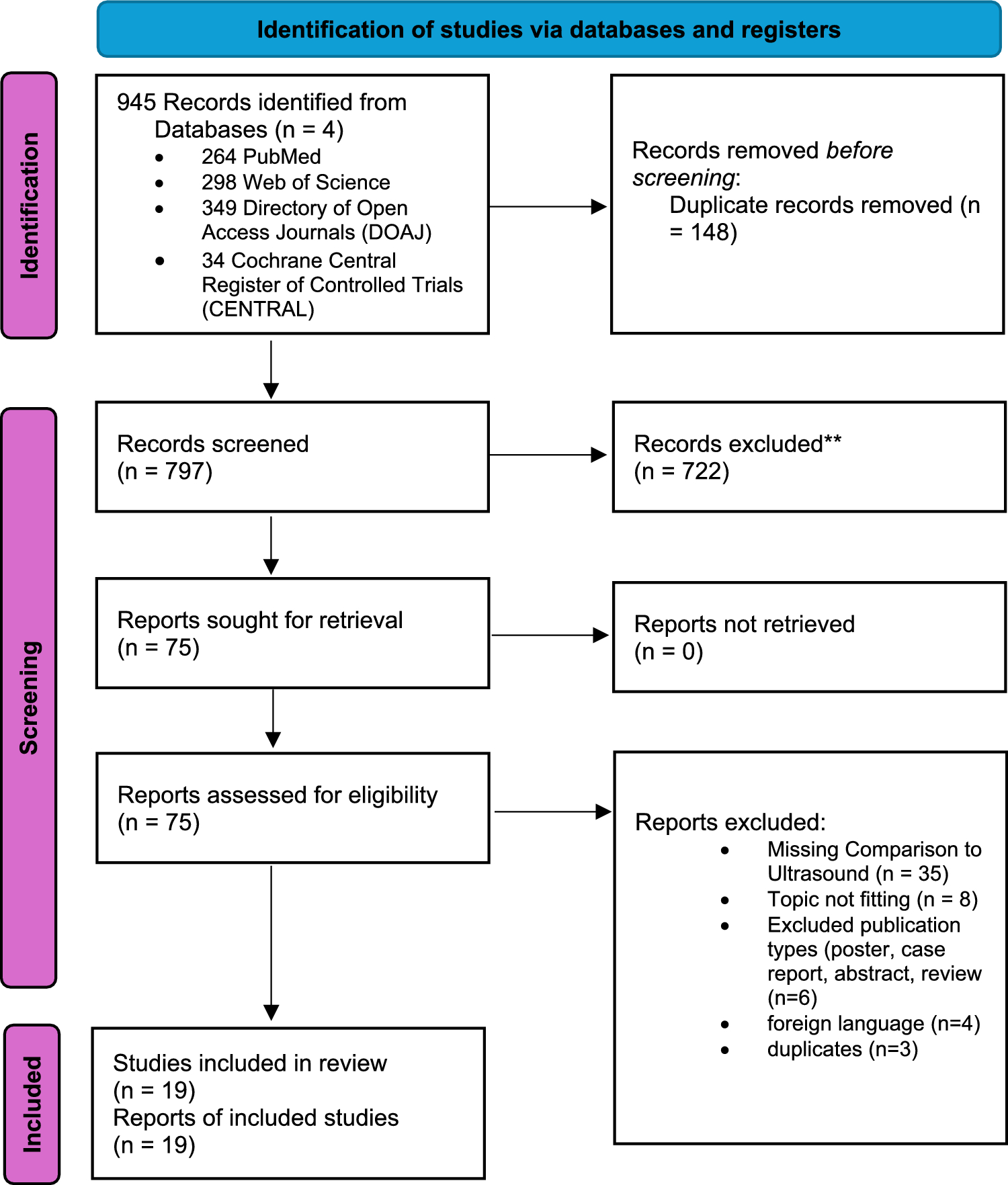
Our search concluded to 1,283 patients. Only 8 studies met the inclusion criteria and were included in the systematic review. Figure 1 summarizes the selection procedure in a PRISMA flowchart.
Fig. 1
PRISMA flowchart of the included studies
The characteristics of the studies included in our systematic review are shown in Table 1. Studies were conducted in Europe (3 studies), America (2 studies) or Asia (3 studies), and were published between 2014 and 2025. The design of the studies was prospective, observational in 1 study, case-control in 3 studies, observational/cross-sectional in 3 studies, and only one study was randomized, single blind, single center study. The number of patients included in the studies ranged from 29 to 336.
Table 1 Patients’ baseline characteristicsThe quality of assessment of the included studies is presented in Supplementary Table. In general, the methodological quality of the included observational studies was moderate to high. According to the Newcastle–Ottawa Scale, quality scores for cohort studies ranged from 6 to 8, and for case-control studies between 7 and 8 points, out of a maximum of 9 points. Most studies demonstrated good representativeness of study populations and adequate ascertainment of exposure and outcomes. Reduced scores were mainly related to limitations in the comparability arm and, for cohort studies, to incomplete follow-up. The single randomized controlled trial was judged to raise some concerns overall according to the Cochrane Risk of Bias 2 tool, primarily related to the randomization process and potential deviations from intended interventions, although outcome measurement was considered at low risk of bias.
Disease-related outcomesAll 8 studies assessed rheumatic and/or immunologic outcomes. Only 2 studies were interventional. In the study of Scrivo et al., RA patients were prospectively studied, having undergone a 3-week restriction of dietary sodium intake, reflected by a drop in their 24-hour sodium urine excretion under 85 mEq/die and subsequently returning to a 2-week period of normal sodium intake [18]. Upon sodium restriction, levels of Th17 cells followed a downward trend, while Treg cells tended to increase, with both effects being reversed during normal sodium intake and none of them reaching significance. Apoptotic and cellular proliferation markers remained unaffected by dietary restrictions, while serum TGFβ1 and IL-9 were significantly suppressed at the end of the study compared to baseline [18]. Kianifard et al. further studied the effects of potassium supplementation on chronic symptomatic RA patients [19]. Maximum disease improvement and joint pain alleviation was reported in the subgroup maintaining a vegetarian diet while receiving a well-tolerated potassium food supplement. This outcome was retrieved by comparing the pain visual analogue scale scores of patients at week 16 post-intervention compared to baseline, which demonstrated a significant mean change, significantly superior to a plain vegetarian diet or routine diet [19].
The rest of studies had a cross-sectional design. In the study of Vitales et al., RA patients were classified as low sodium intake or high sodium intake upon their sodium intake being less or exceeding 5 g/day, respectively [20]. In both groups, the populations of CD4 + CD25highFoxp3+ and CD69 + Treg cells were significantly limited, while Th17 cells were increased compared to healthy subjects, irrespective of sodium consumption patterns. Nonetheless, sodium intake was inversely correlated with the CD69 + Treg cell subset of RA patients. Disease activity measured with DAS28 did not differ between the two groups, while Treg-mediated cytokine secretion was equally suppressed and Th17 differentiation remained unaffected by sodium intake [20].
In the study of Marouen et al.., sodium excretion of early RA patients was reported to be significantly elevated compared to controls, even when adjusted for confounding factors such as tobacco, anti-hypertensive regimen and NSAIDs, as well as alimentary factors using the food frequency questionnaire (FFQ) [21]. Daily sodium excretion levels were higher in RA patients with erosions at diagnosis than without, while the presence of auto-antibodies and RF positivity did not have such impact. Lastly, disease activity as measured by DAS28-CRP was not correlated with sodium excretion patterns [21].
Conflicting evidence was documented in the study of Carranza-Leon et al., in which sodium excretion levels estimated with the Kawasaki formula were found equally elevated in both RA patients and controls [22]. Opposingly, the Na/K excretion ration was significantly greater in RA than in controls. Neither sodium nor potassium intake patterns were correlated with inflammatory markers or the DAS28 index [22], in line with the aforementioned studies [20, 21]. These results are in line with the preliminary observations by Kianifard et al., who found non-significant correlations between dietary potassium with pain visual analogue scale (VAS) scores, Health Assessment Questionnaire (HAQ) score and serum cortisol. No association was reported between dietary potassium and several other clinical variables (including joint counts pain/tenderness and swelling, ESR, CRP and DAS28). However, dietary potassium intake in RA patients was significantly low especially in women, who consumed less potassium compared to men [23].
By contrast, in the study of Minamino et al., spot urine Na/K ratio was found significantly indicative of disease activity, regardless of gender or prednisolone intake [13]. Furthermore, in the study by Anyfanti et al., disease activity as reflected by ESR and DAS28 levels was inversely related to urinary K excretion, while no such association was found with urinary Na or urinary Na/K ratio [24]. This evidence is in favor of the potential capacity of dietary sodium restriction to curb disease progression in RA.
Cardiovascular outcomesOnly 4 studies assessed the association of sodium and potassium intake with cardiovascular outcomes, mostly focusing on hypertension. Carranza-Leon et al. reported higher prevalence of hypertension, pointing towards increased salt sensitivity, in the RA group compared to controls [22]. Notably, levels of potassium excretion were inversely associated with diastolic blood pressure of RA patients. Although the Na/K excretion ration was significantly greater in RA than in controls, it was not associated with hypertension or metabolic syndrome comorbidities [22]. By contrast, urinary Na/K ratio displayed a positive correlation with both systolic and diastolic blood pressure of patients, as well as independent association with hypertension onset, in the study of Minamino et al. [13]. In the prospective interventional study by Kianifard et al., a downward trend was recorded in mean blood pressure levels of patients under potassium-rich diet, without however reaching significance [19].
Lastly, Anyfanti et al. assessed myocardial perfusion with subendocardial viability ratio, and arterial stiffness with pulse wave velocity (PWV) and augmentation index (AIx), as surrogate cardiovascular indices in patients with RA [24]. Levels of 24 h urinary sodium excretion were significantly correlated with HDL-c and uric acid levels, eGFR was proportional to urinary potassium excretion, while urinary Na/K ratio was significantly associated with all three lab markers. Although PWV and AIx were not correlated with urinary sodium or potassium levels, SEVR was inversely associated with both urinary sodium and urinary Na/K ratio, even when adjusted for cardiovascular risk factors [24].
Comments (0)