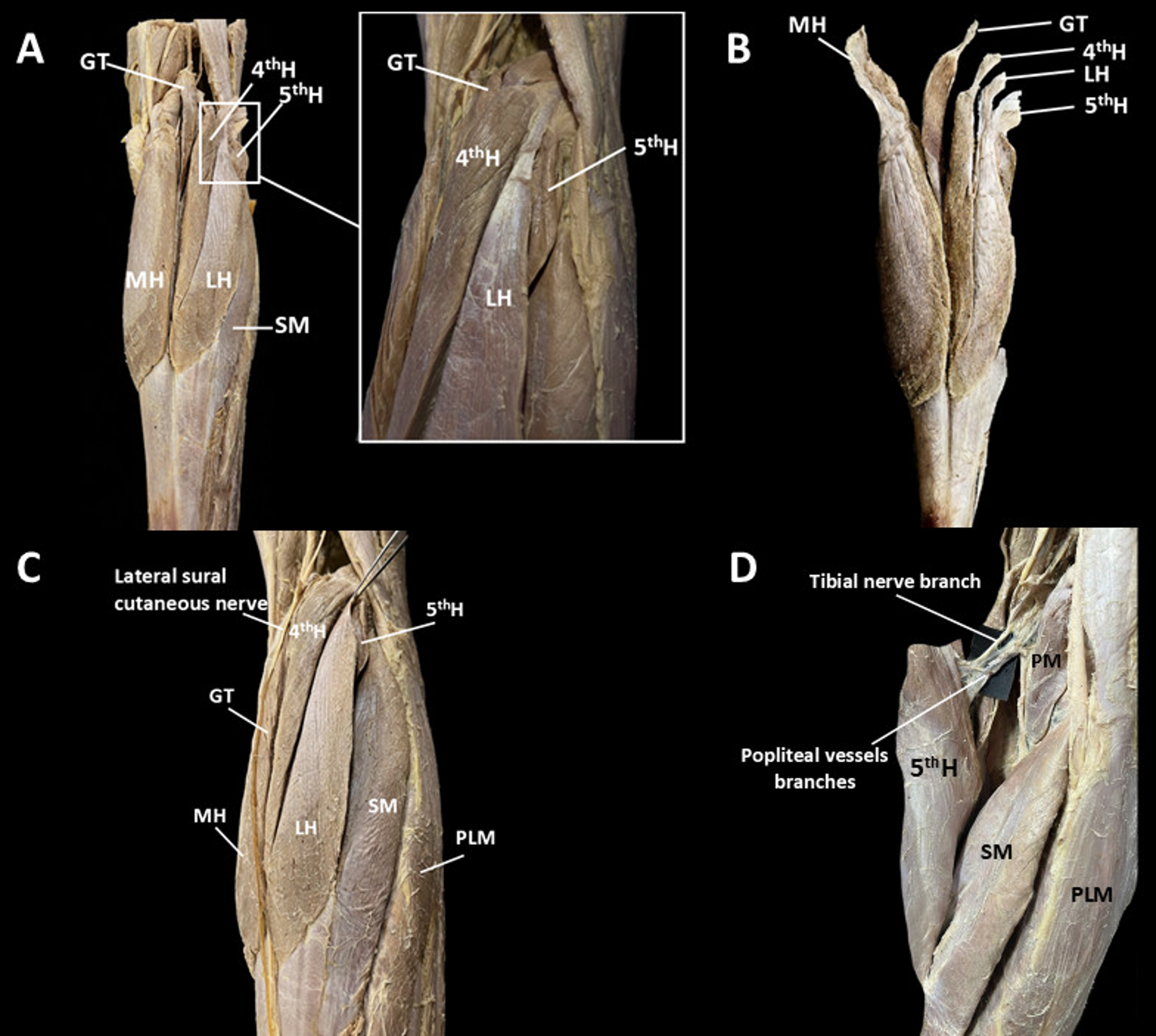
In this report, a novel five-headed configuration of the right GM is described, whereas the contralateral limb displayed a GT functioning as a “third head”. Beyond the presence of the GT, other variations of the GM have been reported, including the occasional absence of the lateral head or even the entire muscle [17], absence of the calcaneal tendon with the MH and LH inserting directly into the bone [15], aberrant origins from the thigh muscles [16], and additional supernumerary heads [2, 13]. Classical anatomical literature reports the presence of a third head of the GM, commonly referred to as the GT [3], and occasionally describes a bifid configuration of this additional belly [10]. Moreover, the literature also documents persistent separation of the medial and lateral heads up to their distal attachment to the calcaneal tendon or complete dissociation from the soleus muscle, cases of hypoplasia or absence of one head, the presence of sesamoid ossicles (e.g., the fabella) within the proximal tendinous attachments, and anomalous muscular slips that fuse the heads into a single muscular mass [18]. Further reported variations include aberrant connections with adjacent muscles such as the plantaris, soleus, and popliteus, as well as “ischio-calcaneal” bundles extending from the hamstrings to the calcaneal tendon [18].
In contrast to the findings of Rodrigues et al. [13], which described a GM in which each main head (LH and MH) was attached to the femur by three symmetrical and robust heads, the configuration observed in the present case is entirely atypical, highlighting an unusual pattern of developmental variation in the superficial muscles of the posterior leg compartment. It is well-established that the posterior leg compartment is poorly differentiated before the second month of development, and variations in these muscles likely result from incomplete separation of the original anlage into three or more distinct muscles. In this context, the GT and the fourth and fifth heads may be considered congenital muscle or tendinous structures originating from different regions of the distal dorsal surface of the femur. These supernumerary heads typically merge with the LH, MH, or both heads of the GM [20].
The unusual configuration described here likely amplifies the clinical risks already associated with supernumerary heads in the popliteal fossa, which may include leg pain, tenderness in the popliteal region, and reduced arterial pulsations in the leg and foot [12, 23]. Indeed, accessory bellies are not rare on MRI, most commonly presenting as a “third head” coursing lateral to the popliteal vessels in approximately 2% of routine knee examinations. Although frequently asymptomatic, their additional bulk and atypical trajectories may narrow the popliteal corridor and modify local shear and strain dynamics [9]. Within this anatomical context, the spectrum of popliteal artery entrapment syndrome (PAES) offers a coherent pathophysiological framework: both anatomic (Rich types I–V) and functional forms can be precipitated or exacerbated by anomalous or hypertrophic gastrocnemius slips, and dynamic imaging with duplex and CTA/MRA during provocative maneuvers is recommended to unmask compression that appears occult in neutral [5]. Beyond arterial disease, venous compromise warrants consideration: isolated popliteal vein entrapment from an accessory slip of the lateral gastrocnemius has been reported in young, athletic patients and can present with deep vein thrombosis (DVT)-like swelling or true thrombosis, with symptom relief after resection of the anomalous muscle [22]. Symptom overlap with chronic exertional compartment syndrome (CECS) is substantial; misdiagnosis in either direction is well documented, and coexistence (functional PAES ± CECS) is increasingly recognized, supporting a dual diagnostic pathway in refractory exertional calf pain [7, 8]. Complex multi-belly anatomy may also heighten the likelihood of musculotendinous-junction injury (“tennis leg”) and intramuscular haematoma, entities that commonly mimic DVT; a structured algorithm (clinical exam → duplex to exclude DVT → targeted US/MRI) helps avoid unnecessary anticoagulation and guides rehabilitation [4]. From a surgical standpoint, supernumerary bellies can obscure or displace the tibial nerve and popliteal vessels during posterior knee approaches and posterior cruciate ligament (PCL) reconstruction; pre-operative MRI mapping and meticulous protection are essential given the millimetric artery-to-PCL distances under arthroscopic conditions [6].
In addition, because MH flaps are a workhorse for peri-knee coverage, recognizing a multi-bellied configuration pre-harvest may influence side selection, arc-of-rotation planning, and pedicle handling to avoid iatrogenic neurovascular traction or partial devascularization of an accessory head [19]. Collectively, these considerations argue for (i) vigilant dynamic imaging in exertional symptoms, (ii) routine description of variant bellies and their relation to vessels/nerve in radiology reports, and (iii) explicit surgical planning notes whenever posterior approaches, vascular decompressions, or gastrocnemius-based reconstructions are contemplated [5, 9].
Finally, clear documentation and high-quality visualization of anatomical variants are essential components of modern anatomical practice. Beyond cataloging variations, detailed dissections and accurate imaging provide a reliable foundation for anatomical education, surgical planning, and clinical interpretation. In this context, the present report contributes to the growing need for well-documented anatomical evidence of morphological diversity.

Comments (0)