
Remember me
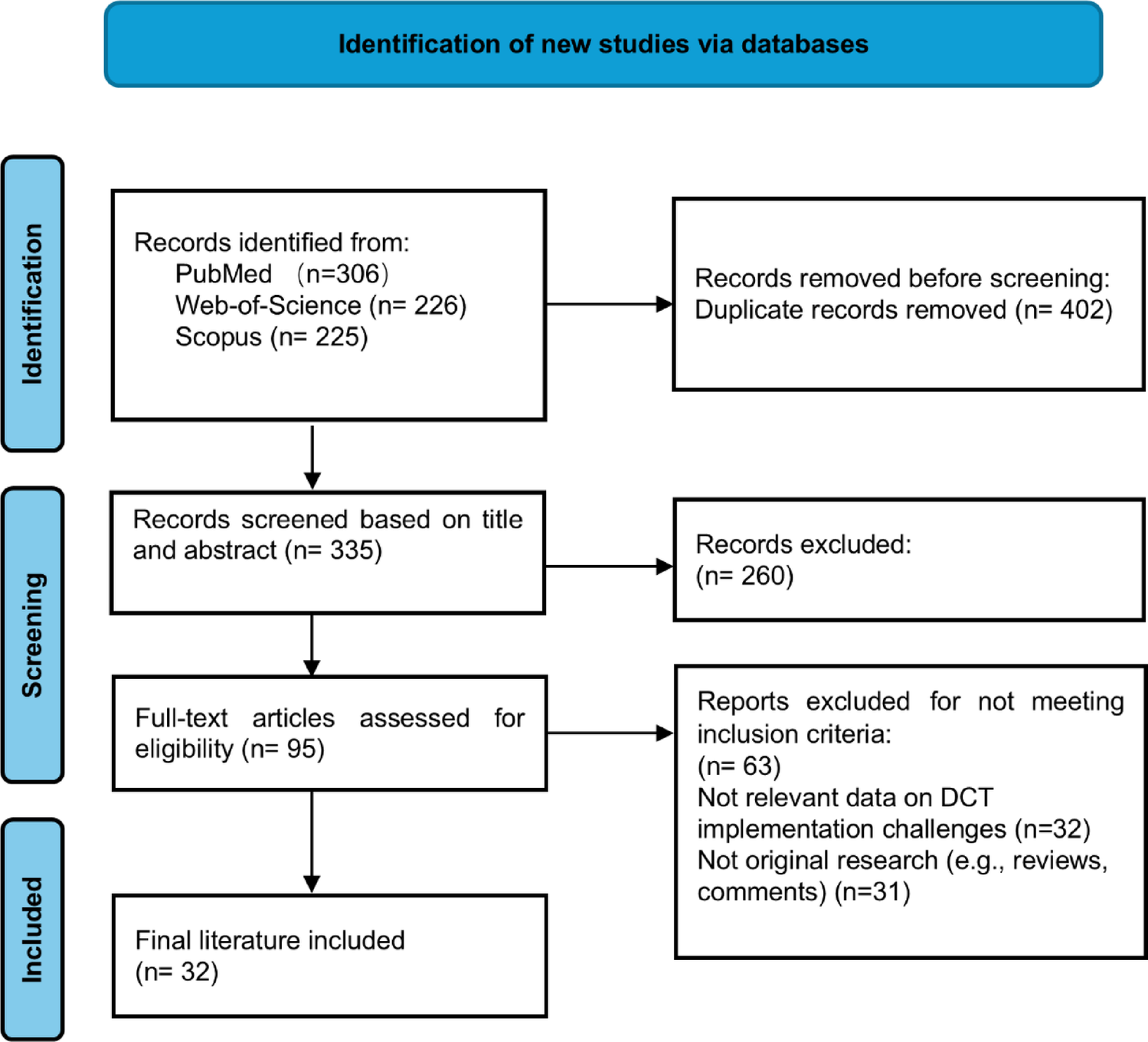
The survey received 2804 response attempts, of which 1,436 were eligible for analysis as they were fully completed. Incomplete survey responses were defined as those in which respondents abandoned the online survey before reaching the final question. The survey system recorded all responses as well as the percentage of questions completed.
Of the respondents, 80.4% were mothers (n = 1,155), 15.8% were fathers (n = 226), 2.4% were other types of caregivers (n = 35), and 1.4% were young adult patients, all of whom were ≥ 18 years old (n = 20) (Table 1). As the majority of survey respondents were parents, for the purposes of this analysis we will henceforth refer parents as the primary caregivers who contributed most substantially to this study, although the data reported by other types of caregivers and young adult patients (3.8%) is included in the analysis.
Table 1 Profile of the survey respondentsThe mean age of respondents, excluding young adult patients, was 42.7 years (SD = 7.4). The mean age of the patients represented in the survey responses was 8.7 years, with an age range from 2 months to 18 years.
88.6% of respondents lived in the country where the patient was born (n = 1,272); 3.6% (n = 52) of those living abroad held permanent residency and dual nationality; and 3.3% (n = 47) were permanent residents with immigrant status (See Supplementary Information).
Regarding the patients’ medical conditions, 96.5% (n = 1,386) of respondents reported that their child had a rare disease, while 3.5% (n = 50) indicated they didn’t know [10]. All respondents provided information about the patient’s diagnosis. The most frequently reported disease was phenylketonuria, with 24 responses, representing only 1.6% of the sample. In contrast, 1,295 different rare diseases were each reported by only one family (90.2%). Among those who indicated uncertainty, a review of the data revealed that only one parent reported a diagnosis of autism, which is not considered a rare disease in children and removed from the dataset. Based on these findings, we can confirm that the dataset analyzed in this study represents parents of children living with a rare disease.
Parents were also asked to report their country of birth, their child’s country of birth, and their current country of residence. In all three cases, Spain and France were the most frequently represented, together accounting for approximately half of the responses. This situation reflects the influence of the survey’s dissemination by the principal and corresponding author in Spain, as well as by one of the co-authors in France. Tables 2, 3, and 4 present data from the five most represented countries for these questions. The complete dataset is available as Supplementary Information.
Table 2 Country where the respondent was bornTable 3 Country where the patient was bornTable 4 Country of residenceMother Tongue and Competency in Other LanguagesThe online survey was completed in 21 different European languages, and the three most frequent were Spanish (44.7%, n = 642), English (10.0%, n = 144), and French (8.6%, n = 123). The Serbian version, while offered as a translation, did not receive any responses. The most common native (first) languages of the respondents were Spanish (37.9%, n = 545), French (8.8%, n = 124), and Catalan (6.3%, n = 90)Footnote 1♣ (see Supplementary Information).
Several questions about language competence in languages other than the respondents’ native language were included. Of the 1436 respondents, 800 (55.7%) reported being able to communicate in English, with a self-reported proficiency level of intermediate (38.7%, n = 310), advanced (36.7%, n = 294), native (13.9%, n = 111), and beginner (10.6%, n = 85).
Respondents were asked to assess the patient’s ability to speak English. Only 14.7% (n = 211) were able to speak the language fluently. 85.0% (n = 1,221) of the patients could not speak English, and four respondents (0.3%) did not respond to this question. Among those who were reported being able to speak English, 30.8% (n = 65) were native speakers, 29.4% (n = 62) were intermediate, 24.3% (n = 51) advanced, and 15.6% (n = 33) beginner.
38.1% of parents (n = 547) reported the ability to understand and make themselves understood in a language other than English and their native language. The three most spoken languages reported were: Spanish (30.3%, n = 166) French (28.7%, n = 157) and Italian (11.9%, n = 65). Regarding the patients, as reported by their parents, only 16.6% were able to speak a language other than their native language or English.
Experience as a Participant in a Pediatric Clinical TrialThirteen questions were presented to the parents of pediatric patients to analyze the experience of their child participating in clinical trials. 10.6% of the families had previous experience participating in a clinical trial (n = 153), while 89.3% had never participated in a clinical trial (n = 1,283). At the time the families reported this data, 46 (30.1%) were actively participating in a clinical trial.
Among the 153 families with prior experience participating in a clinical trial, 67.9% (n = 104) had participated in one trial and 16.3% (n = 49) had participated in two trials. Only five families reported having participated in three trials, two families in four trials, two families in five trials, and one family in seven trials. Fourteen families did not respond to the question. 46 (30.0%) of the 153 families reported participating in a clinical trial outside their country of residence.
Children Reported Being Excluded from Participating in a Clinical Trial AbroadSeventy-five (5.2%) of the 1,436 children were reported to be excluded from participating in a clinical trial abroad. 26 (34.7%), families reported that the exclusion was due to language barriers or the country of residence. Ten (13.3%) families reported being informed that language was one of the eligibility criteria specified in the clinical trial protocol and, for this reason, they were excluded from participation.
In 47.8% (n = 33) of the cases, the principal investigator was the person who informed the families about the exclusion. In the remaining cases, the information was provided by the patient’s physician, research nurse, or other healthcare professionals.
Regarding the reasons that motivated families to consider participating in a pediatric clinical trial abroad, 37.5% (n = 24) reported that the decision was driven by the opportunity to access a new experimental treatment not yet available in their country of residence. 32.8% (n = 21) were motivated by potential access to a new treatment that was not available through a similar clinical trial in their home country, 10.9% (n = 7) cited the opportunity to access a European-level center of excellence, and 18.7% (n = 12) reported other reasons.
Parents’ Reports of Their Experience of Their Child Participating in a Pediatric Clinical Trial AbroadThirty-eight (82.6%) of 46 families who participated in a clinical trial abroad stayed overnight during medical visits related to the trial (range 1–52 nights, mean 15,19 ± 14.67 SD). Of these, 47.4% (n = 18) stayed in a hotel, 28.9% (n = 11) stayed at the hospital, and 23.7% (n = 9) stayed in another type of accommodation. The average number of overnight stays per year varied among families. 15.8% (n = 6) families reported staying three nights per year, 13.2% (n = 5) reported staying two nights, and 10.5% (n = 4) reported staying four nights. See Fig. 1.
Fig. 1
Distribution of the number of overnight stays per family per year
Considering the variability in the number of overnight stays per family during a year of participation in a clinical trial abroad, several statistical parameters were analyzed: minimum value (19), maximum value (52), standard deviation (14.67), and mean (15.19). These variables were explored to assess the diversity of study designs and to estimate the length of time families would need to stay in the foreign country where the trial was conducted. The number of days is an indicator of participant burden, particularly given that some families, particularly given that some families might not speak the country’s official language.
Forty of 46 families (86.9%) who participated in a clinical trial abroad reported on the translation of the informed consent document and about the process to access to the content provided by the sponsor of the trial. Table 5 summarizes the different translation methods used. The most common approach was translation by a trained interpreter and signing a consent form in the local language (22.5%). In six of the 46 families (13.1%), it was not necessary to translate the informed consent form, as they were able to understand and communicate in the official language of the country where the clinical trial was conducted.
Table 5 Methods used to translate informed consent forms for international participantsAs the survey was targeted to caregivers and young adult patients, information about the assent form and process was not included.
Child or Parent Questionnaires or Outcome Reported MeasuresPatient- and parent-reported outcome tools are commonly used in clinical trials to collect data that only participants can provide, typically related to quality of life. However, validating these tools in the native language of the patient or parents can be a barrier to including international participants in a clinical trial. Despite this limitation, some studies use professional interpreters to translate the tools, helping to make the study more inclusive and avoiding discrimination based on language. These tools are often written in simplified or “plain” language, which facilitates ad hoc oral or written translation into the patient’s language when needed.
Of the 46 families who reported having participated in a clinical study abroad, 40 provided information about the languages in which the Patient Reported Outcome Measures (PROMs) were provided. From them, seventeen families (42.5%) stated that the questionnaires were available in the patient’s native language.
Twenty families gave specific details about how they accessed the questionnaires.
In 40% of cases (n = 8), families completed the questionnaires with the assistance of a professional translator. In 35% of cases (n = 7), parents were proficient in English and completed the questionnaires in that language. Table 6 summarizes the types of translation support that enabled parents to complete the clinical trial questionnaires.
Table 6 Types of translations that make questionnaires accessible to international parentsTranslation of Additional InformationOften, pediatric clinical trials provide supplementary information to patients and parents in various formats (patient diaries, flyers, websites, etc.). 39 parents replied to the question about whether any informative resources were offered as part of the clinical trial. Of these, 29 (74.4%) confirmed that additional informational materials were provided in the study in which they participated.
Among them, 51.7% accessed these resources in the original language (the official language of the site), while 48.3% had access to a translation in their respective native language.
Parents’ Preferences About Decentralization and Digitalization of Pediatric Clinical TrialsDifferent decentralization and digitalization options were presented to the parents who responded to the survey, in two different theoretical settings: (1) the study was conducted in their country of residence, and (2) the clinical trial was conducted abroad.
Parents were asked to report their preferences using a Likert scale: (1) Not really willing, (2) Not willing, (3) Undecided, (4) Somewhat willing, and (5) Willing. The proposed options could potentially reduce the number of study visits and travel requirements or enhance the patient/parent experience (e.g., completing questionnaires on a digital device instead of using paper forms).
In both scenarios, most (> 65%) parents indicated that they would accept any of the options. The most accepted option, both for trials conducted in the patient's country and for access to a cross-border study, was completing trial questionnaires using a digital device (76.1%). The least preferred options for studies conducted in the patient's home country were measuring vital signs at home by parents (67.2%) and using wearables to collect clinical data (67.7%). In the cross-border study scenario, the least preferred options were home nursing and having parents measure vital signs at home, with 65.5% of parents indicating they were “Willing” to accept these. See Figs. 2 and 3 Detailed data can be found in Supplementary Information.
Fig. 2
Parents' preferences regarding decentralization and digitalization when the trial is conducted in their country
Fig. 3
Parents' preferences regarding decentralization and digitalization when the trial is conducted abroad
Comments (0)