This study identified cancer risks separately for male and female coal mine workers and showed differences in cancer risk between male and female coal mine workers by job.
Compared to the general population, cancer risk varies across Work Categories and by sex. Male Production workers were more at risk of cancer than the general population and when compared to the rest of cohort after adjusting for smoking (Supplementary Table S8). Male Production workers showed an overall increased risk of cancer and specifically of lip, colorectal, larynx, lung, melanoma, prostate, urinary tract and lymphoid cancer. Male Maintenance workers have an increased risk of lip, gallbladder, melanoma, and mesothelioma. Administrative and the Occasionally exposed male workers had an increased risk of melanoma and mesothelioma. Male Exploration drillers had excess melanoma and lip cancers, Construction workers of pharyngeal and lung cancer Unexposed non-office workers of colorectal cancer, Truck drivers and Labourers of lymphoid leukemia. Melanoma risk was significantly increased in female Administration workers.
Lung cancer was higher among male Construction and Production workers compared to the rest of the cohort, after adjusting for era, age and smoking. Coal mine workers, particularly Production and Construction workers are exposed to respirable crystalline silica and diesel engine emissions, both of which are known carcinogens carcinogens [1, 2]. Underground coal miners cannot smoke at work so they may smoke less than the general population. A previous meta-analysis [5] did not show an increased risk of lung cancer in coal miners. However, lower smoking rates in coal mine workers may explain these findings, as case-control studies in which smoking was controlled showed higher risks for lung cancer than cohort studies with no smoking adjustment [5]. Investigation of the coal workers’ pneumoconiosis rates by Work Category could be informative.
The inclusion of many more recently exposed workers in the cohort may have diluted the observed risk because of the healthy worker effect. In other words, older workers may have been diagnosed with cancer and left the cohort before 1992. Alternatively, there may have been more dust exposure among Production workers in the earlier years [12].
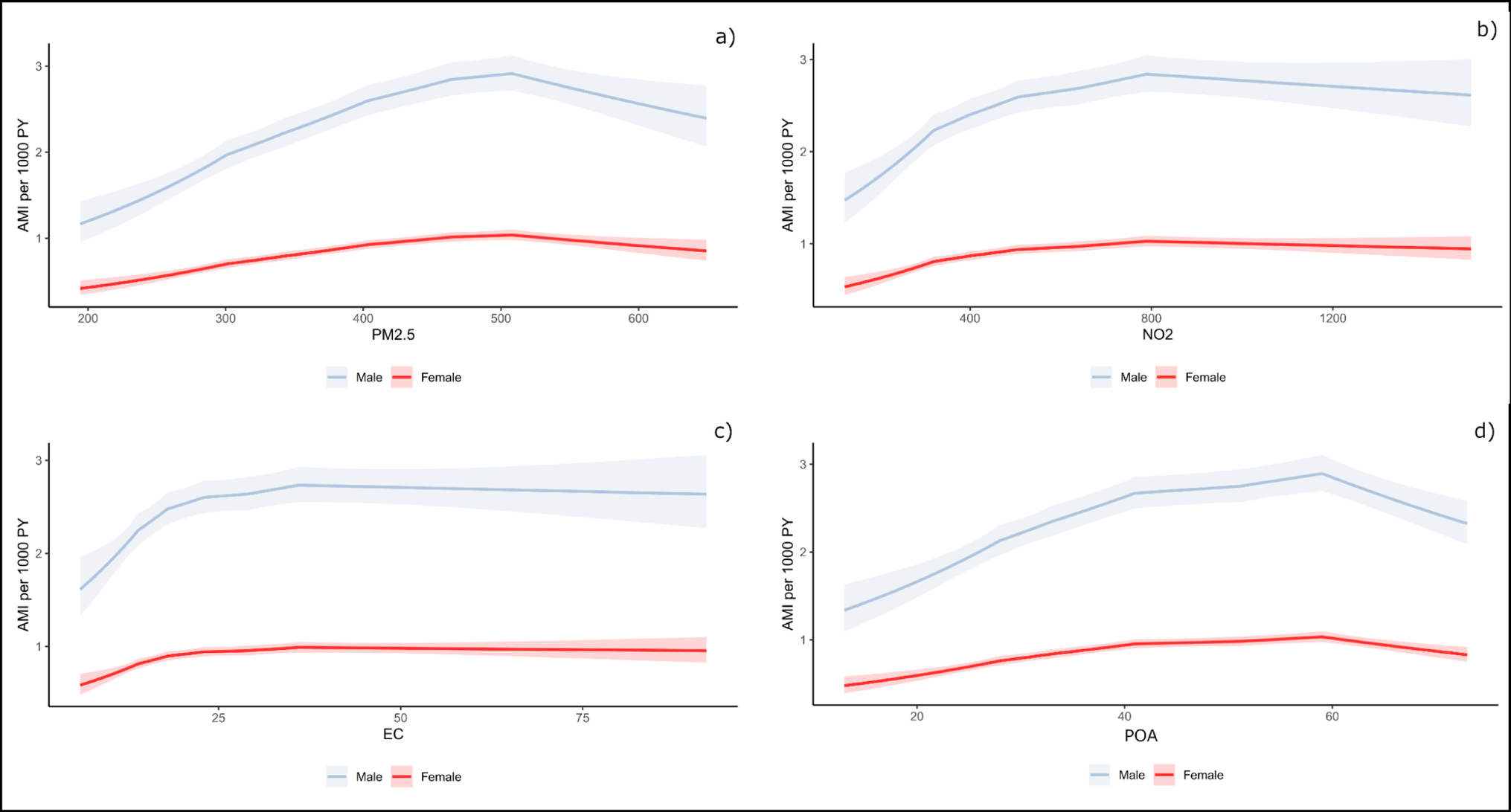
Coal mine workers are exposed to coal mine dust, including RCS and DEE. However, exposure data were not available for specific mines nor for before 1992, so constructing an individual’s exposure history was not possible. Production workers are likely to be more exposed than Maintenance or Administration workers, and exposures are likely to have been higher, on average, for underground workers than for open-cut workers. Exposure data from the Queensland mines were reviewed by Cliff et al. [12]. The average exposure to respirable coal mine dust in the four Queensland Longwall mines in 1992–1994 varied between 1.3 and 3.5 mg/m3 [12]. Data from 11 Queensland underground mines from 1996 to 2001 identified mean 8 hour TWAs of between 1.59 and 3.24 mg/m3 (overall average 2.06 mg/m3). However, the data had a skewed distribution, with between 0 and 45% of the data from each mine exceeding the occupational exposure limit of 3 mg/m3 and reaching 15 mg/m3 [12]. Cliff pointed out that exposures were lower in New South Wales (NSW) coal mines during this period [12] and a cohort study of 23,630 male NSW coal miners found an all-cancer SIR of 82 (95%CI 73–92) [13], which was lower than that in this study. Between 2000 and 2017, the average yearly respirable coal mine dust (RCMD) exposure of Queensland underground production workers was between 0.75 and 2.75 mg/m3 [13]. It is likely that the average RCMD exposure was well below the occupational exposure limit of 3 mg/m3 for production workers who commenced work after 2000, but an increased incidence of lung cancer was still observed.
Between 2000 and 2017, the average yearly RCS exposure for Queensland underground production workers was usually between 0.01 and 0.06 mg/m3 [12]. Data from 11 of the 14 mines showed that annual exposures were usually below 0.025 mg/m3 between 2002 and 2017 [12]. Australian coal mines are thought to have thicker seams than many US mines, so the rock is less likely to be disturbed, leading to lower silica exposure [14]. Between 1999 and 2017, the average yearly RCS exposure for most Queensland open-cut production workers was somewhat lower than that for underground workers, between 0.01 and 0.015 mg/m3 [12]. Blast crew and dragline operators had an average exposure of approximately 0.02 mg/m3 RCS.
As the majority of the sites were open-cut, radon exposure is unlikely to be significant.
The risks of melanoma [3] and lip cancer [15] risks are likely related to sun exposure, particularly in Queensland. Other risk factors for lip cancer include age and male gender, poorer socio-economic circumstances, smoking and alcohol, sunlight exposure early in life and cumulatively, viral infections and immunosuppression [16]. In an earlier analysis [8] it was noted that the excess melanoma cases observed when comparing cohort rates to the Australian population were attenuated when the cohort rates were compared with the Queensland rates, that is, the elevated melanoma risks are related to the state of residence rather than occupation. Brown et al. found comparable risks of malignant melanoma between New South Wales (NSW) coal mine workers and the general population; however, for workers who started working in an open-cut mine, the risk was significantly increased. There was no increased risk of lip cancer in NSW coal miners [13].
The elevated prostate cancer incidence could be a result of diagnostic bias following increased screening in the working population, increased survival of patients with better general health, or earlier access to treatment. However, the within-cohort comparisons suggest that there is a real increase in the risk for Production workers.
Gallbladder cancer is a rare cancer that usually occurs in people over 80 years of age and is more common in women. There is an increase in gallbladder cancer among women and male maintenance workers. A recent systematic review identified possible associations of cholangiocarcinoma (the predominant type of gallbladder cancer) with the solvent 1,2-dichloropropane, asbestos, endocrine-disrupting compounds, and rotating shift work. [16} It is more likely that maintenance workers would be exposed to 1,2-dichloropropane and asbestos than would other coal mine workers. A meta analysis of 26 studies did not find a convincing association between gallbladder cancer and smoking or alcohol consumption [17].
Lymphoid leukaemia was increased for men in several Work Categories; Production, Truck drivers and Labourers. Chronic lymphocytic leukaemias, the largest group of lymphoid leukaemias, are now grouped with Non Hodgkin lymphoma (NHL) [18]. About 98% of the lymphoid leukaemias in this study were chronic lymphocytic leukaemias. The environmental causes of CLL are uncertain but may relate to living or working on a farm [19]. Large case control studies of NHL in Canada [20] and USA [21] did not identified an association with work as a miner. Brown et al. did not find an increased risk of lymphohaematopoietic cancers in NSW coal miners despite concern about an NHL cluster in a specific coal mine [13]. Gilman et al. [22] identified an increased odds ratio for leukaemia associated with more than 25 years working as an underground miner (as a proxy for higher electromagnetic field exposure). No other mine worker studies were identified that examined this outcome.
The study included multiple comparisons across eight job categories and several cancer types, for men and women (where possible) increasing the possibility of chance findings. In some cancer categories the numbers of cases were small. Repeating the findings in the future when more cases may have accumulated would be of interest. The results should be examined as a whole and considered in the context of findings from other cohorts [5].
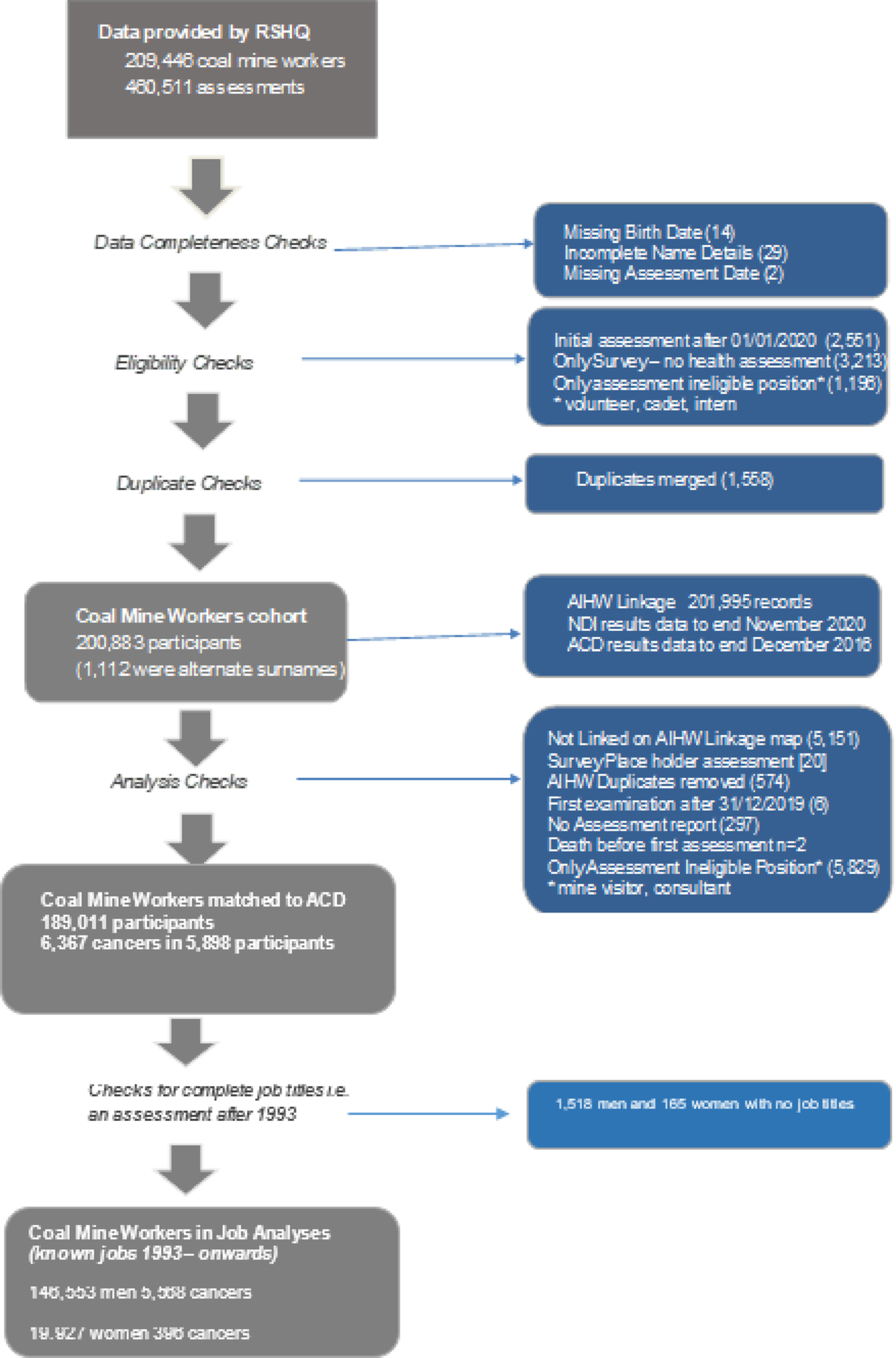
The strength of this study is the complete enumeration of Queensland coal mine workers employed since 1993, including almost 20,000 women. Smoking data from at least one assessment were included in over 99% of the participants.
Cancer registration is mandatory in all Australian States and Territories, and registration, including for cancer, is virtually complete [23]. The cohort names were matched to those in the ACD, although the National Linkage Map is a probabilistic process. The availability of quality identifiers routinely collected over time by RSHQ records improves the probability of a correct match between cohort members and the ACD. Matching to the Australian national data was necessary because approximately 20% of the matches were identified in states other than Queensland. Coal mine workers may be Fly -in Fly-out from other states or retire to states other than Queensland, so matching only to the Queensland data would miss cancers.
The limitations of the study include the relative youth of the cohort and the short follow-up period, starting in or after 2003, for the majority of workers. The study was sufficiently powered to identify a significantly increased risk of overall cancer for female workers and major cancer categories for men in most Work Categories. There was a short period of follow-up for women, with small numbers of cancers reported, so caution should be used in interpreting these results. The latent period for cancers varies e.g. perhaps 10 years for leukaemia [24], around 10–15 years for many solid tumours [25] but can be 30–40 years for mesotheliomas [26]. The first assessment for half the cohort was in or after 2010 (Table 2), so it is probably too soon for many of the work-related cancers to manifest as the ACD data was only complete to the end of 2016.
The precise dates of employment as a coal mine worker were not known, only the dates of their first assessment and any subsequent assessments. Complete job histories were not accessible to the participants, the medical assessments did not include dates of change for jobs. Employment as a coal miner in other states or overseas has not been captured. Furthermore, it was not clear whether some individuals were underground workers, so there may be some misclassification of underground workers to open-cut. However, the classification as an underground worker is likely to be correct.
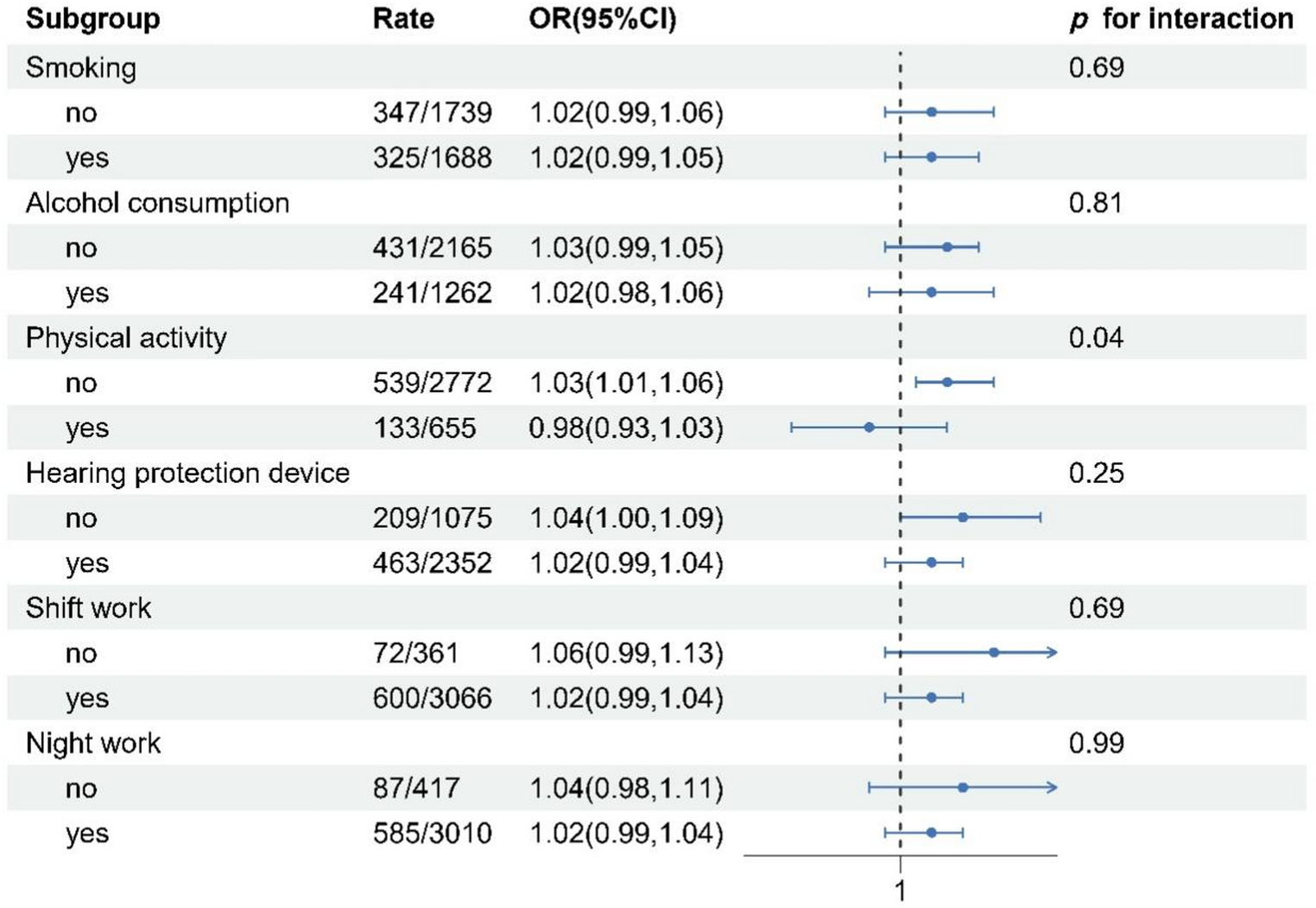
Additionally, the study could not consider individual genetic or lifestyle factors such as ethnicity, alcohol consumption, diet, non-occupational exposures, or occupational exposures experienced, for example, in previous jobs.

Comments (0)