
Remember me

This retrospective, single-center cohort study was conducted at Sun Yat-sen Memorial Hospital. The study protocol was reviewed and approved by the Medical Ethics Committee of Sun Yat-sen Memorial Hospital(No: SYSKY-2025-1052-01), which waived the requirement for informed consent due to the retrospective nature of the study. All procedures were performed in accordance with the ethical standards of the institutional and with the 1964 Helsinki declaration and its later amendments.
We retrospectively screened the medical records of all patients diagnosed with Kawasaki disease (KD) complicated by coronary artery aneurysms (CAAs) who were admitted to our center between January 2018 and December 2023. The diagnosis of KD and CAA was based on the American Heart Association (AHA) diagnostic criteria and guidelines for echocardiographic assessment of coronary arteries [19]. Coronary artery lesions were classified according to the result of echocardiography: small aneurysm (Z-score ≥ 2.5 to < 5, or internal diameter 3–4 mm in children < 5 years; 4–5 mm in children ≥ 5 years), medium aneurysm (Z-score ≥ 5 to < 10, or internal diameter 4–8 mm), and giant aneurysm (Z-score ≥ 10, or internal diameter ≥ 8 mm) [20].
Inclusion criteria were: (1) confirmed diagnosis of KD; (2) confirmed presence of CAA by echocardiography at the time of KD diagnosis or before IVIG treatment and coronary CT angiography (CCTA) within one week; (3) availability of complete clinical, laboratory, and echocardiography follow-up data for at least 12 months after the acute phase. Exclusion criteria were: (1) presence of congenital heart disease or other acquired cardiovascular diseases; (2) incomplete medical records or loss to follow-up; (3) poor-quality CCTA images precluding quantitative analysis. The clinical indications for coronary CT angiography (CCTA) in our cohort were: (1) follow-up evaluation of known coronary artery aneurysms (CAAs) after Kawasaki disease (KD), (2) assessment of coronary artery morphology when echocardiography provided suboptimal visualization, and (3) pre-interventional planning for patients with giant aneurysms or stenotic lesions. The decision to proceed with CCTA was made by the attending pediatric cardiologist based on clinical need, patient cooperation, and renal function.
For each patient, the most severe coronary aneurysm was selected as the criterion for determining whether the coronary aneurysm was regressed or not at follow-up. Based on the evolution of CAAs on follow-up imaging, patients were divided into two groups: the Regression (R) group and the Non-Regression (NR) group. Aneurysm Regression meets either of the following conditions: Z-score < 2.0 or aneurysm maximum diameter < 3.0 mm (for younger children, Z-score reference value is limited). The judgement time point is as follows: comparison of baseline and follow-up echocardiography (interval ≥ 12 months), the above criteria continuously meet ≥ 2 consecutive follow-up visits [1, 9]. Given that follow-up data are unavailable for some lesions due to limited compliance with examinations in pediatric patients, we analyzed lesion evolution on a per-patient basis for the largest coronary aneurysm, rather than on a per-lesion basis.
Data collectionDemographic, clinical, and laboratory data were systematically extracted from electronic medical records using a standardized data collection form. The following baseline variables were collected: Age, sex, body mass index (BMI), duration of illness before intravenous immunoglobulin (IVIG) administration, presence of IVIG resistance (defined as persistent or recrudescent fever ≥ 36 h after completion of initial IVIG therapy), diagnosis of incomplete KD, duration of fever (≥ 7 days vs. <7 days), and presence of specific cardiac findings on initial echocardiography (left ventricular dysfunction, mitral regurgitation, pericardial effusion), Hemoglobin (anemia defined as Hb < 80 g/L), platelet count (thrombocytopenia), serum albumin level (hypoalbuminemia), C-reactive protein (CRP; dichotomized at > 100 mg/L), erythrocyte sedimentation rate (ESR), procalcitonin (PCT), and white blood cell (WBC) count (dichotomized at ≥ 30 × 10⁹/L vs. <30 × 10⁹/L).
Coronary artery lesion characteristics: assessed via initial echocardiographyVariables assessed included: the number of aneurysms, their location (proximal, mid, or distal segments of the left anterior descending, left main, or right coronary arteries), the maximal diameter of the coronary artery aneurysm (CAA), the corresponding Z-score, and the presence of complications (such as thrombus formation, calcification, stenosis, or coronary wall thickening). CAA size was classified as small, medium, or giant according to the criteria specified earlier. Echocardiographic findings of children at the initial stage of Kawasaki disease and during follow-up for one year or more were analyzed.
CCTA imaging analysis and pericoronary fat attenuation index measurementAll patients underwent electrocardiogram-gated coronary CT angiography (CCTA) using a CT scanner (Discovery CT750 HD, GE Healthcare, Milwaukee, Wisconsin) during the subacute phase (within one week of initial echocardiography).
After breath-holding training, ECG-gated coronary angiography was performed in elderly children using the following scan parameters: Tube voltage 80 kV, Tube current 60–100 mAs. The non-breath-holding little children underwent conventional spiral CT scanning under calm breathing conditions (during sleep or after training) with Tube voltage 80 kV, Tube current 18–45 mAs. The scanning parameters were delay 15–18 s, slice thickness 3.0 mm, scan time 5–8 s, reconstruction kernel B 31 f medium smooth+, reconstructed slice thickness 1.0 mm, and interval 0.4–0.8 mm.
The contrast medium used was Iohexol (350 mg I/mL), administered at an injection rate of 1–2 mL/s with a dose of 2 mL/kg body weight. Scanning was performed from the head side to the foot side, covering a range from 1 cm below the tracheal bifurcation to the basal plane.
In accordance with the ALARA principle, a low-dose scanning protocol was selected to minimize radiation exposure. The mean radiation dose was 0.46 ± 0.24 mSv.
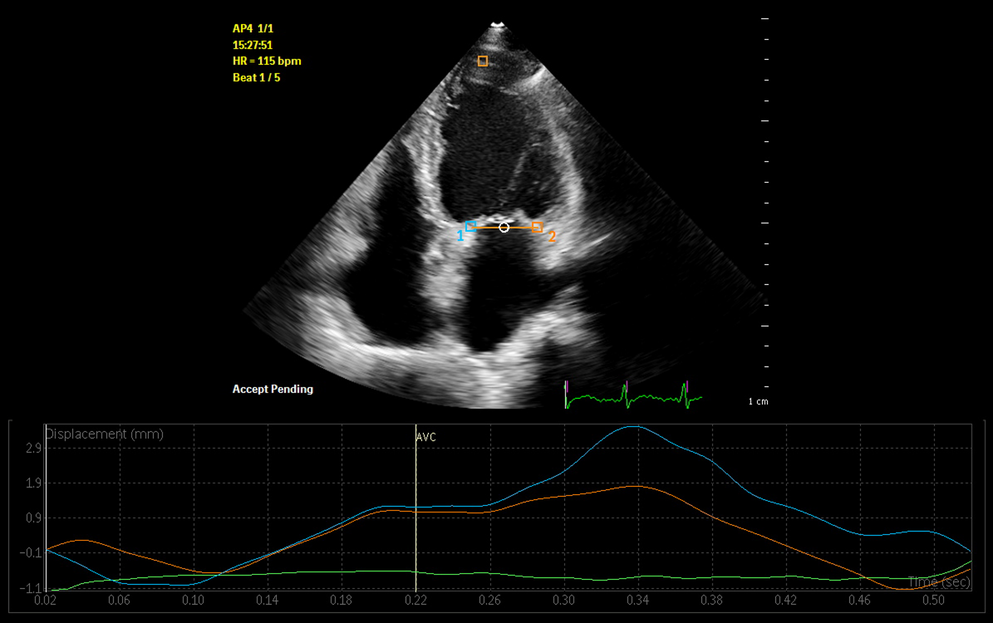
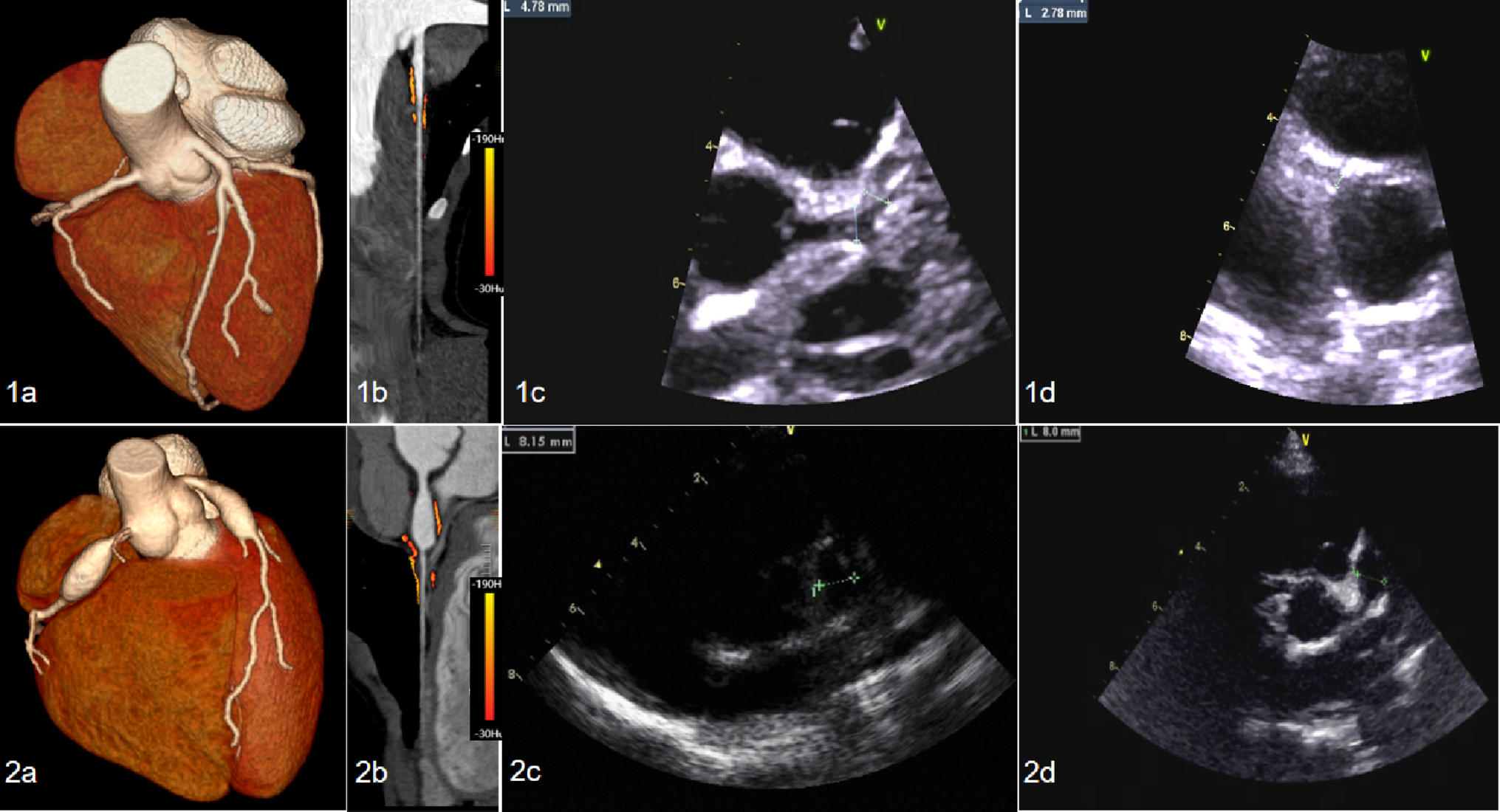
The pericoronary fat attenuation index (FAI) was quantitatively assessed as a marker of pericoronary inflammation, following a validated methodology [21, 22]. Briefly, CCTA images were analyzed using specialized research software (uAI-CoronaryCTA, United Imaging). For each patient, the most severe coronary artery aneurysm detected both in initial CCTA and cardiac ultrasound examination was selected for subsequent follow-up via cardiac ultrasound. The ROI was defined as the segment of the coronary artery lumen with the largest diameter, extending 20 mm proximally and distally from the center of a fusiform aneurysm as the reference point. For fat attenuation index (FAI) measurement, a radial ROI was manually traced, extending 5 mm outward from the outer vessel wall (epicardial border) along the entire length of the aneurysm, while excluding areas adjacent to myocardium, pericardium, or large epicardial fat depots. This approach is consistent with methods previously described by Antonopoulos et al. and Oikonomou et al. [21, 22]. The mean attenuation (Hounsfield Units, HU) of all adipose tissue voxels within this ROI (defined as -190 HU to -30 HU) was calculated, yielding the perivascular FAI. Lower (more negative) FAI values indicate less inflamed pericoronary adipose tissue. The measurement process is shown in Fig. 1. The analysis was performed by two radiologists with > 5 years of experience in cardiovascular imaging, who was blinded to all clinical data and patient outcomes.
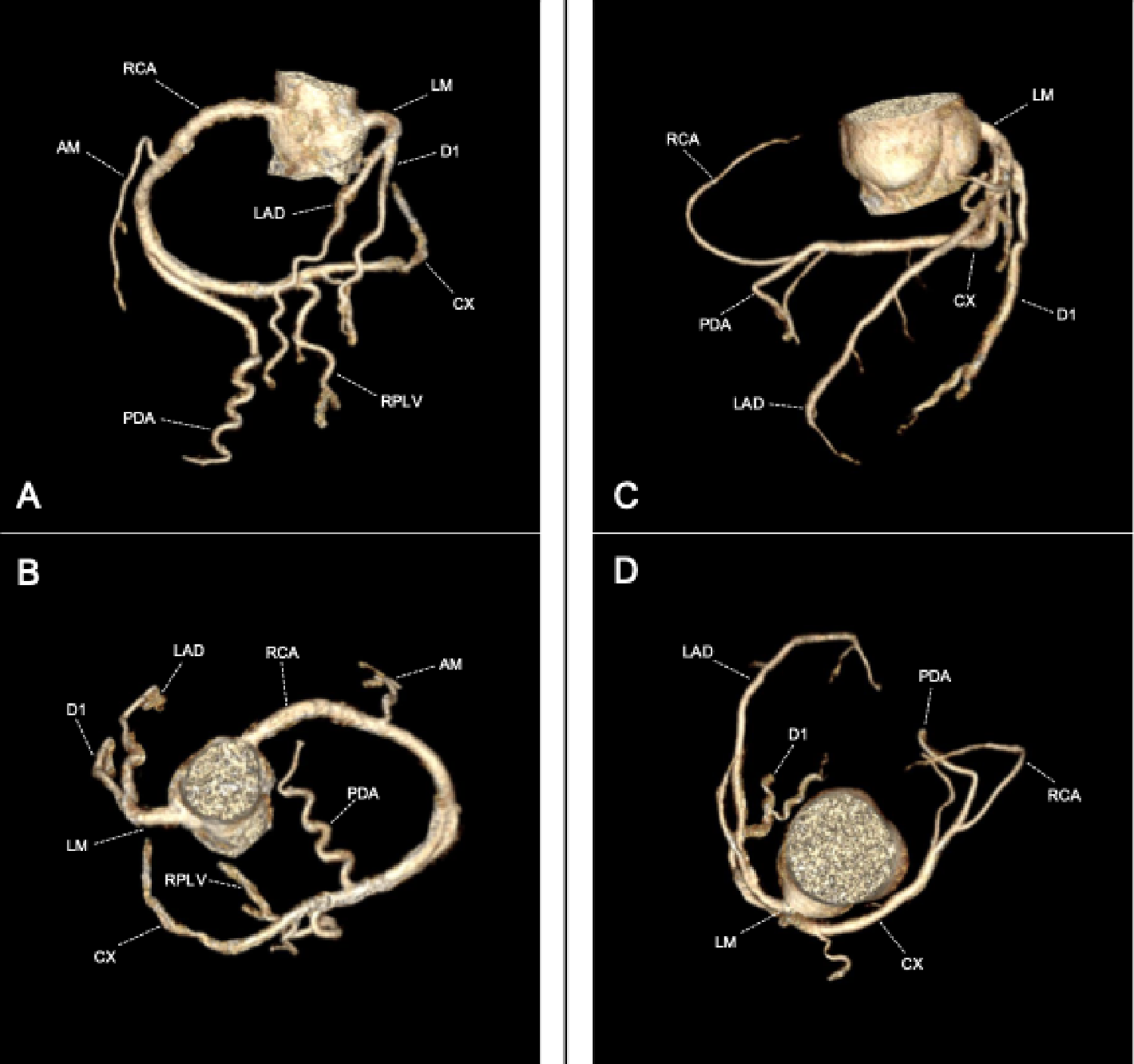
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Comparison of a KD case with CAA regression and a KD case with CAA non-regression. CCTA and echocardiography images obtained during follow-up for a year-old boy with CAA regression (1a-1d) and for a 10-year-old girl with CAA non-regression (2a-2d). 1a, 2a The images of coronary artery obtained by the volume rendering technique show small aneurysms(1a) and large aneurysms(1b) in the LAD and RCA respectively. 1b, 2b The images of coronary artery obtained by the multi-Planar reconstruction technique show FAIs of left anterior descending coronary artery, the values of FAI in the small CAAs is lower than that in the large CAAs. 1c Echocardiography within 1 week of onset showed a aneurysm of the proximal left anterior descending coronary artery, with a maximum diameter about 4.78 mm and wall thickening. 1d Echocardiography performed one year later showed regression of the proximal left anterior descending coronary artery aneurysm, with maximum diameter about 2.78 mm, and less wall thickening than before. 2c Echocardiography within 1 week of onset showed a aneurysm of the proximal left anterior descending coronary artery, with a maximum diameter about 8.15 mm and wall thickening. 2d Echocardiography performed one year later showed non-regression of the proximal left anterior descending coronary artery aneurysm, with maximum diameter about 8.0 mm. KD, Kawasaki disease; CAA, coronary artery aneurysms; CCTA, coronary computed tomography angiography, LAD, left anterior descending; RCA, right coronary artery; FAI, fat attenuation index
Statistical analysisStatistical analysis was performed using SPSS software (version 26.0, IBM Corp.) and R software (version 4.2.1). Continuous variables were tested for normality using the Shapiro-Wilk test. Normally distributed data are presented as mean ± standard deviation (SD) and compared using the independent samples t-test. Non-normally distributed data are presented as median with interquartile range [Q1, Q3] and compared using the Mann-Whitney U test. Categorical variables are presented as counts and percentages and compared using the Chi-square test or Fisher’s exact test, as appropriate. A two-tailed p-value < 0.05 was considered statistically significant. Variables with a p-value < 0.10 in univariate analysis or deemed clinically relevant based on prior literature were entered into a multivariate binary logistic regression model (forward stepwise likelihood ratio method) to identify independent predictors associated with CAA regression. Results are expressed as odds ratios (OR) with corresponding 95% confidence intervals (CI).
Comments (0)