Ethical considerations and selection and preparation of teeth
This study was approved by the Local Ethics Committee from Faculdade São Leopoldo Mandic under protocol number: 67181823.2.0000.5374. Thirty single-rooted maxillary and mandibular premolars extracted for periodontal or orthodontic reasons were selected. The teeth were stored in a 0.1% aqueous thymol solution at 4 ºC for no longer than 6 months. Exclusion criteria included teeth with cervical root lesions (e.g., caries, abrasion, or erosion), root fractures, misshapen or elliptical root canals, or previous endodontic treatment. All specimens exhibited a Type I configuration, according to Vertucci’s classification [13]. Root lengths were standardized to approximately 14 mm and checked with a plastic caliper (Starfer, São Paulo, SP, Brazil).
Next, biomechanical preparation of the root canals was performed. Initial instrumentation was conducted manually using #15 and #20 files (Dentsply, Petrópolis, RJ, Brazil) under irrigation with 2.5% sodium hypochlorite (Rioquímica, São José do Rio Preto, SP, Brazil), and rinsing with 0.9% sterile saline (Eurofarma, São Paulo, SP, Brazil). Using the same disinfection and irrigation protocol, rotary instrumentation was performed with 25.05, 30.06, and 40.01 files (Easy Equipamentos Odontológicas, Belo Horizonte, Brazil) [14]. The working length was determined by subtracting 1 mm from the actual tooth length. After biomechanical preparation, the canals were treated filled using M-sized gutta-percha cones (Meta® Biomed Co, London, UK), FM accessory cones (Meta® Biomed, London, UK), and AH Plus Jet cement (Dentsply, Petrópolis, RJ, Brazil). The roots were then stored at 100% relative humidity at 37ºC in a dental oven (Nova Técnica, Piracicaba, SP, Brazil) for 24 h to allow complete cement setting.
Root canal unobstruction and scanning of resin patterns and silicone molds
The root canals were unobstructed using #3 to #5 Largo Peeso Reamer drills (Dentsply/Maillefer, Petrópolis, RJ, Brazil) attached to a contra-angle handpiece. The roots were then embedded in a 19 × 20 mm PVC connection (Tigre, Joinville, SC, Brazil) with high-performance addition silicone (Scan Putty, Yller Biomaterials, Pelotas, RS, Brazil), leaving 1 mm of the cervical third exposed. Subsequently, the root canals were enlarged using #4137 and #4138 diamond burs (KG Sorensen, São Paulo, SP, Brazil), attached to a contra-angle handpiece under water cooling, achieving a standardized length of 10 mm. A graphite demarcation was made on the drill to ensure precise unobstruction length, and verification was performed using a straight probe and rubber stopper.
After unobstruction, the roots were randomly assigned to two experimental groups according to the root canal molding method: acrylic resin pattern or silicone molding. The main materials used in this study are summarized in Table 1.
Table 1 Description of materials used in this studyAcrylic resin pattern group and silicone molding group
Resin patterns were fabricated using prefabricated plastic posts (PinJet; Angelus, Londrina, PR, Brazil) relined with self-curing acrylic resin (Duralay, Reliance Dental Brazil, São Paulo, SP, Brazil). The completed resin patterns (n = 15) were stored in sealed plastic containers without moisture for 24 h. After storage, the resin patterns were affixed to a wax sprue and scanned using an intraoral scanner (Trios, 3Shape, Copenhagen, Denmark).
A high-performance addition silicone (Scan Putty, Yller Biomaterials, Pelotas, RS, Brazil) was manipulated and inserted into the root canal using a spatula until the canal was completely filled. A prefabricated plastic pin (PinJet; Angelus, Londrina, PR, Brazil) was then passively inserted, allowing excess silicone to extrude from the root canal and accumulate around the plastic pin. After polymerization, excess material from the coronal portion was removed using a #11 surgical scalpel blade, and the silicone replica was carefully extracted from the tooth. Storage and scanning procedures were performed following the same protocol described for the acrylic resin pattern group. The number of teeth was also proportional to the previous group (n = 15).
Milling and cementation of FGPs
After scanning, the milling process was performed using a Motion 2 milling machine (Amann Girrbach, Austria) with a Fiber Cad-Post & Core block (Angelus, Londrina, PR, Brazil). The milling procedure followed the standard protocol of the machine, and was conducted in three stages, each using a different bur. Cementation was performed by a single operator using a dual-cure resin cement (RelyX U200, 3 M ESPE) in accordance with the manufacturer’s instructions. The samples were then stored at 100% relative humidity at 37 °C for 48 h to allow complete polymerization.
Analysis of apical gaps
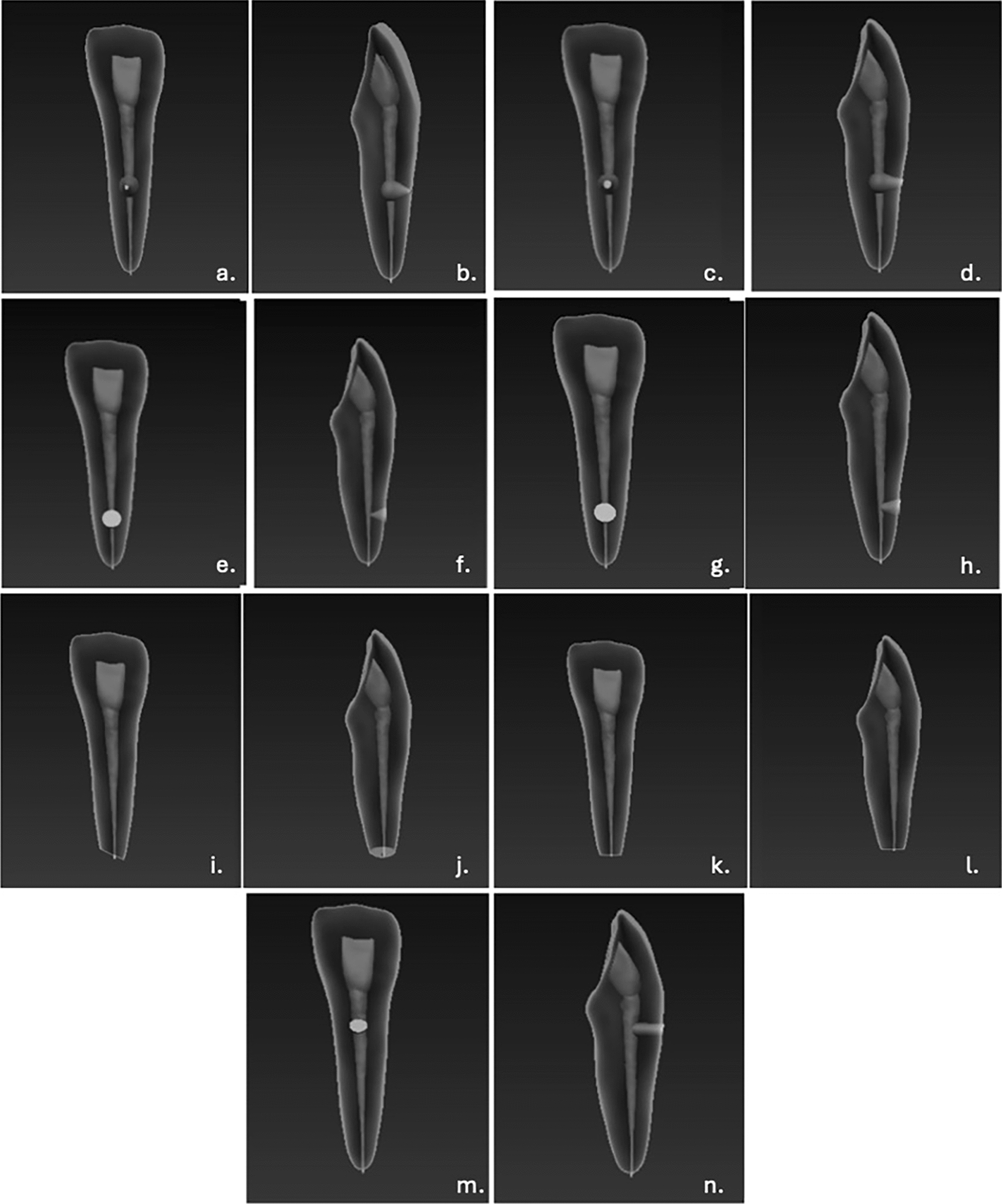
Radiographs were taken to assess the presence of apical gaps and any remaining gutta-percha. All radiographs were captured using an intraoral dental X-ray machine (Procion ION 70X, Brazil) and adult periapical wireless sensors (Vistascan, Dürr Dental, Bietigheim-Bissingen, Germany). To ensure that X-rays struck the tooth surface perpendicularly, the distance between the X-ray tube and the sensor was standardized at 30 cm. A standard adult periapical film with a width of 40 mm was used. Measurements were conducted using the ruler tool in the ImageJ graphics analysis program (Version 1.54, National Institutes of Health, Bethesda, MD, USA). Prior to the measurements, image calibration was conducted as required. A straight line corresponding to the known length was drawn using the Shift key, and the “Analyze” menu was accessed, followed by “Set Scale,” where the reference value of 40 mm was entered. After calibration, all linear measurements were automatically converted from pixels to millimeters. The digital ruler of the ImageJ software was used to measure the distance between the last visible pixel of the fiberglass post and the gutta-percha.
Push-out bond strength test
Each sample was individually and parallelly affixed to an acrylic resin plate using utility wax, and then transversally sectioned with a high-concentration diamond disk (Series 15 HC, Buehler, Lake Bluff, IL, USA) attached to a metallographic cutter (Isomet 1000 Precision Saw, Buehler, IL, USA) at 300 rpm under constant water cooling. Slices corresponding to the apical, middle, and cervical root thirds were obtained. Two 1-mm-thick slices were obtained per root third from each tooth, with only one slice randomly selected for the push-out bond strength test and the other for the scanning electron microscope (SEM) evaluation.
For the push-out bond strength test, one slice from each root third (apical, middle, and cervical) was placed in a universal testing machine (EMIC DL2000, São José dos Pinhais, SP, Brazil). The force required to displace the fiberglass post cement was recorded in kgF, and converted into stress values (MPa), using the following formula: A = π (R + r) √h2 + (R – r)2, where π = 3.1416, R = fiber post radius measured on the cervical side of the slice, r = fiber post radius measured on the apical side of the slice, and h = height of the root slice.
Mode of failure
After the push-out test, the samples were analyzed using a stereoscopic microscope (SQF Tecnival, São Paulo, SP, Brazil) at 40 × magnification to determine the failure mode. Failures were categorized as follows: Adhesive failure between resin cement (CR) and dentin (D), Adhesive failure between resin cement and fiberglass post (FGP), Cohesive failure of the FGP, Cohesive failure of the CR, Cohesive failure of the dentin (D), and Mixed failure (M), when two failure types occurred simultaneously [14].
Measurement of resin cement thickness using scanning electron microscopy (SEM)
Slices not used in the push-out bond strength test were analyzed using an SEM (Carl Zeiss AG, EVO® 40 series) to measure cement thickness (µm) and quantify voids. After testing different magnification fields, 70 × was selected for its optimal field of view, allowing for the measurement of cement thickness at four predefined points per sample: top, bottom, left, and right. All SEM images were exported to ImageJ software (Version 1.54, National Institutes of Health, Bethesda, MD, USA). The ruler function in ImageJ was calibrated using the scale bar embedded in each SEM image to ensure measurement accuracy. After calibration, four measurements per slice were taken, and the average cement thickness (µm) was calculated.
Void quantification using scanning electron microscopy (SEM)
Void analysis was conducted using scanning electron microscopy (SEM). Dark regions were considered indicative of either the absence of restorative material or the presence of interfacial gaps at the tooth–restoration interface. Void detection was performed qualitatively (presence/absence) in cross-sectional images corresponding to the apical, middle, and cervical thirds, and the results were expressed as percentages. Digital images were analyzed using ImageJ software (NIH, Bethesda, MD, USA). Prior to analysis, images were converted to 8-bit grayscale, and automatic threshold segmentation was performed using Otsu’s method (Otsu, 1979) to enable objective discrimination between void areas and filling material [15].
Statistical analysis
Descriptive and exploratory analyses indicated that apical gaps, bond strength, and cement thickness data did not meet the assumptions required for a parametric analysis. Therefore, apical gaps were analyzed using the Mann–Whitney test. The effects of the molding technique, root third, and the interaction between these factors were investigated using a generalized linear model, considering a split-plot design to account for the dependency structure among the three root thirds evaluated within the same sample. The association between the presence of voids and the molding technique was analyzed using the Chi-square test and Fisher’s exact test, according to the suitability of each situation.
Statistical analyses were performed using R software (R Core Team, 2025) and SAS software (SAS Institute, Cary, NC, USA). The significance level was set at 5% [16].



Comments (0)