The manuscript of this laboratory study has been written according to the Preferred Reporting Items for Laboratory Studies in Endodontology (PRILE) 2021 guidelines [16] (Figure S1).
Ethical approval
This study was approved by Institutional Research Ethics Committee of the (protocol #61206522.4.0000.5419).
Experimental design
This study was conducted in two phases. First, the mechanical properties of the five nickel–titanium (NiTi) systems (Blue Shaper, VDW Rotate, ProTaper Ultimate, ProTaper Next, and WaveOne Gold) were evaluated through cyclic fatigue, torsional resistance, and bending resistance tests.
Subsequently, fifty mandibular first molars (n = 10 per system) were instrumented to assess the biomechanical shaping performance of each system. Micro-CT was used to obtain quantitative 2D (area, circularity, diameters, and transportation) and 3D parameters (volume, surface area, SMI, and prepared wall percentage), as well as qualitative 3D reconstructions of dentin thickness before and after preparation.
The study is designed to compare whole commercial systems (system-level contrasts); therefore, reported outcomes reflect the integrated effect of design variables (taper, cross-sectional geometry, heat treatment, kinematics, and sequence) and do not represent isolation of single device attributes.
Mechanical properties’ evaluationCyclic and torsional fatigue tests
One hundred and fifty new nickel–titanium instruments, 25 mm in length, were used: 50 instruments allocated to the cyclic fatigue test, 50 instruments allocated to the torsional test, and 50 instruments allocated to the bending resistance test (n = 10 per group per test). The instruments tested were Blue Shaper 25.06 (Zarc4Endo, Asturias, Spain), VDW Rotate 25.06 (VDW, Munich, Germany), ProTaper Ultimate 25.08 (Dentsply Sirona, Charlotte, NC, USA), ProTaper Next 25.06 (Dentsply Sirona, Charlotte, NC, USA), and WaveOne Gold 25.07 (Dentsply Sirona, Charlotte, NC, USA). All instruments were inspected under a stereomicroscope (Carl Zeiss, Oberkochen, Germany) at 16 × magnification to detect manufacturing defects or deformations prior to testing; none were excluded.
The evaluated systems differ intrinsically in final taper, cross-sectional mass, and kinematic mode: PTU (25.08) presents a final taper of 0.08, WOG (25.07) presents 0.07 in a reciprocating single-file format, while BS, RT, and PTN present 0.06 final tapers with varying sequence sizes. These design differences (taper, section geometry, and number of instruments per sequence) inherently influence metallic mass, stiffness, and contact patterns with canal walls; consequently, comparisons are presented at the system level rather than as isolation of single variables.
Cyclic fatigue testing was performed in a previously described custom-made device using a stainless-steel artificial canal with a 60-degree curvature and a 5 mm radius, maintained at 35 degrees Celsius ± 1 °C. The stainless-steel artificial canal was selected to provide a standardized and reproducible curvature geometry, radius, temperature control, and lubrication conditions, allowing reliable intergroup comparison of cyclic fatigue resistance under strictly controlled experimental parameters. We acknowledge that the stainless-steel canal does not reproduce the tribological properties of dentin (hardness, organic content, microstructure, and smear formation); therefore, cyclic fatigue lifetimes obtained in this model should be interpreted as standardized comparative metrics and not as direct surrogates of in vivo performance in dentin. To address translational relevance, mechanical testing was complemented by shaping assessments performed in extracted human teeth using high-resolution micro-CT, which provide the clinically relevant morphological outcomes.
Each instrument was used according to the manufacturer’s recommended parameters on a VDW Silver engine (VDW, Munich, Germany) as follows: Blue Shaper 25.06 (400 rpm, 4 N•cm); VDW Rotate 25.06 (350 rpm, 2.3 N•cm); ProTaper Ultimate 25.08 (400 rpm, 4 N•cm); ProTaper Next 25.06 (350 rpm, 4 N•cm); WaveOne Gold 25.07 (WaveOne Gold Primary mode; manufacturer's reciprocation settings, nominally corresponding to the WaveOne mode). The artificial canal was continuously lubricated with synthetic oil (Super Oil, Singer Co. Ltd., Elizabethport, NJ, USA) to minimize friction. Instruments were activated until fracture, which was detected visually and audibly. Time to fracture was recorded in seconds and the number of cycles to failure (NCF) was calculated as.
$$}\, = \,\left( }\left[ } \right]\, \times \,}} \right)/0$$
Torsional resistance testing was carried out according to ISO 3630-1 specifications using a custom torsion device (Analógica, Belo Horizonte, Brazil) as previously described [1]. The apical 3 mm of each instrument was clamped in a chuck connected to the torsion shaft after removal of the handle at the fixation point. A computer-controlled gear motor (Analógica, Belo Horizonte, Brazil) operating clockwise at 2 rpm was used for all groups. Torque and angular rotation were automatically recorded by the MicroTorque software (Analógica, Belo Horizonte, Brazil) until fracture. The maximum torque and angular deflection at fracture were obtained from the recorded data.
Bending resistance test
Bending resistance was evaluated on the third set of 50 instruments (n = 10 per group). The test used a custom-built device designed in accordance with ISO 3630–1 standards [1]. Instruments were clamped 5 mm from the tip and positioned perpendicular to the motor axis. A resistive angular transducer connected to a process controller monitored the bending angle until a 60° deflection was reached. The torque required to achieve the prescribed deflection was automatically measured by a load cell and recorded by the testing system. Flexibility was expressed as the torque (N•cm) at 60° deflection.
For the cyclic fatigue test, the time to fracture (seconds) and number of cycles to failure (NCF) were recorded. The maximum torque (N•cm) and angular deflection (°) were measured in the torsional resistance test, whereas the torque required for deflection (N•cm) was obtained from the bending resistance test.
Scanning electron microscopy (SEM) analysis
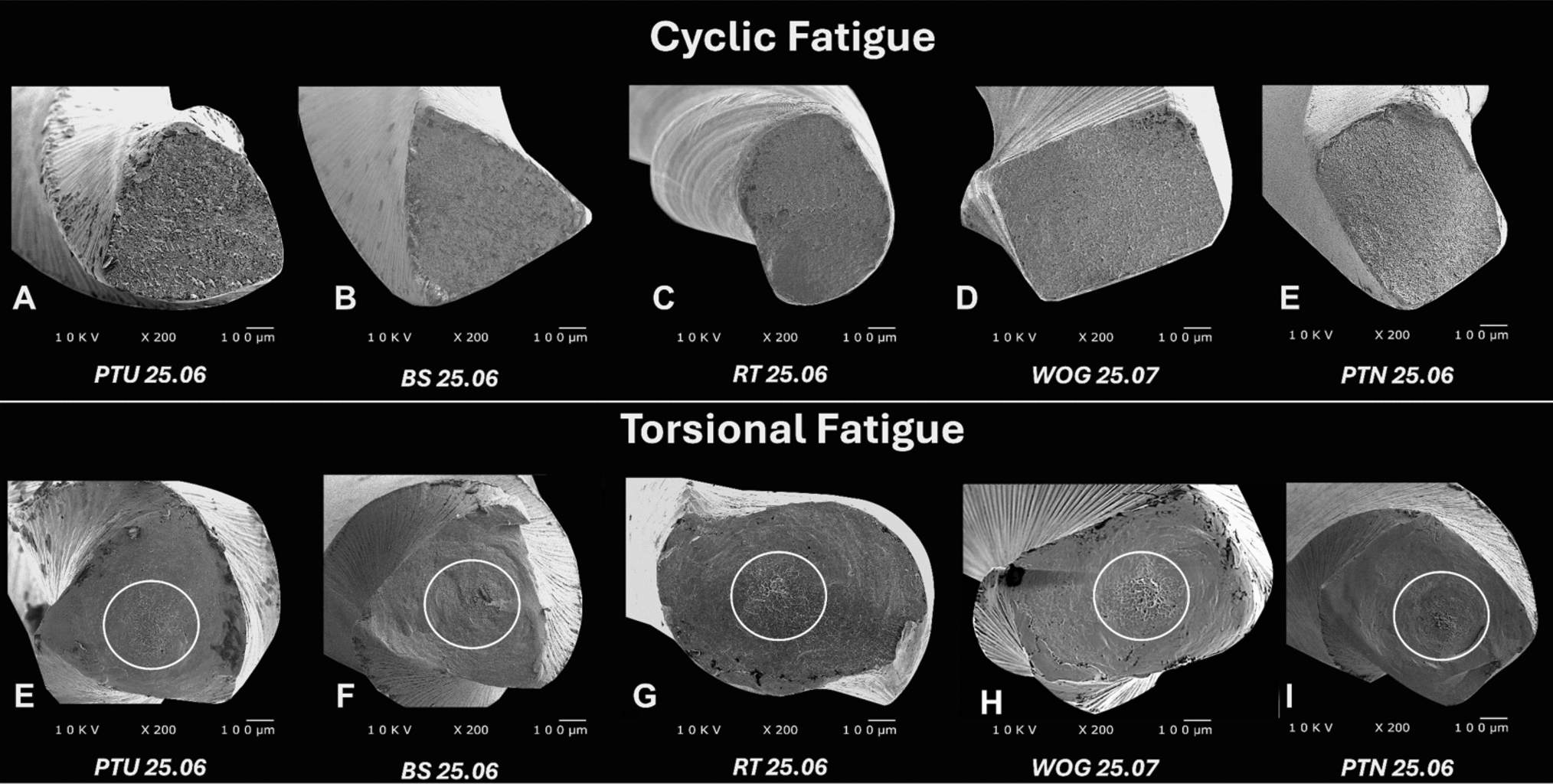
After the cyclic and torsional fatigue tests, the fractured fragments of the instruments were examined under scanning electron microscopy (SEM) (JEOL, JSM-TLLOA, Tokyo, Japan) to characterize the topographical features of the fracture surfaces.
Prior to SEM evaluation, the fragments were ultrasonically cleaned (Gnatus, Ribeirão Preto, São Paulo, Brazil) in distilled water for 3 min to remove debris and metallic residues generated during mechanical testing.
Fracture surfaces were examined at 200 × magnification to identify typical failure patterns. Fractures resulting from cyclic fatigue exhibited dimples and crack initiation areas, consistent with fatigue crack propagation, whereas torsional failures displayed concentric abrasion marks and central microcavities, characteristic of localized plastic deformation before final rupture.
Shaping ability evaluationInitial sample selection
Specimens were obtained from the Human Tooth Biobank of the School of Dentistry of Ribeirão Preto, University of São Paulo (FORP–USP) (CONEP Registry B-002). Initially, 125 extracted human mandibular first molars were retrieved and examined under a stereomicroscope (Nikon, Melville, NY, USA) for eligibility. Selection criteria comprised birooted teeth with intact root structure, fully developed apices, and straight or moderately curved canals.
The sample size calculation was performed based on data obtained from a previous study, considering the difference between group means of the morphometric parameters assessed by micro-computed tomography (micro-CT) as the primary outcome [13]. The calculation assumed a minimum detectable difference between means of 0.40, a coefficient of variation of 0.20, a significance level (α) of 0.05, and a statistical power (1 − β) of 0.80. Under these parameters, the minimum estimated sample size was 8 specimens per group. To account for potential specimen loss during preparation, scanning, or image processing, and to increase the robustness of the statistical analysis, the final sample size was set at 10 specimens per group (n = 10). This sample size is also consistent with previous high-resolution micro-CT studies evaluating the shaping ability of endodontic instruments, in which group sizes ranging from 8 to 12 specimens are commonly used, balancing effect detection, specimen availability, and the operational demands associated with scanning and image processing [8, 28].
Later, 50 teeth that met the inclusion criteria were selected, randomly assigned to the five instrumentation groups (n = 10 per group), and were stored individually in 0.1% thymol solution until use. Prior to testing, specimens were rinsed under running water for 24 h and their external root surfaces were cleaned by ultrasonic scaling (Profi II Ceramic, Dabi Atlante Ltda., Ribeirão Preto, SP, Brazil) to remove debris and calculus. Subsequently, each tooth was placed individually in a plastic container with 1 mL of distilled water and incubated at 37 °C for 72 h to ensure standardized rehydration before micro-CT scanning and biomechanical preparation.
CBCT screening for sample selection
Square Styrofoam plates (7 × 7 cm) were fabricated to stabilize the specimens during cone-beam computed tomography (CBCT) scanning. Small 1-mm-deep depressions were created at 1-cm intervals to position and align the teeth in rows, maintaining consistent buccolingual and mesiodistal orientations. The first and last teeth in each row were intentionally positioned differently to serve as positional reference markers during image analysis.
A total of eight plates were used, each containing 25 teeth arranged in five vertical and five horizontal rows. The plates were placed on the scanning table of a PreXion 3D cone-beam computed tomography unit (Prexion Co. Ltd., Tokyo, Japan) under an endodontic imaging protocol (90 kV, 4 mA, 37 s, isotropic voxel size of 0.10 mm, and 5 × 5 mm field of view [FOV]).
All images were exported in DICOM (Digital Imaging and Communication in Medicine) format and analyzed using OnDemand3D Dental software (Instrumentarium Dental, Finland).
A total of five scans were performed, yielding 125 teeth, which were evaluated by multiplanar navigation across sagittal, coronal, and axial planes. From this dataset, 50 mandibular first molars were selected, each exhibiting two mesial canals and one distal canal (Vertucci types II and I, respectively), and showing no perforations, pulp calcifications, or previous endodontic treatment.
Initial micro-computed tomography (micro-CT) evaluation
The selected samples were scanned using a high-resolution micro-computed tomography (micro-CT) system, SkyScan 1174 v.2 (Bruker microCT, Kontich, Belgium). Before scanning, the buccal surface of each crown was marked with a permanent pen to standardize specimen orientation.
Each specimen was individually fixed in utility wax No. 7 (Technew, Rio de Janeiro, Brazil) to stabilize it on a metallic micro-positioner that was firmly attached to the rotating stage of the scanner by a manual adjustment screw. Thus, each tooth was positioned perpendicular to the X-ray source, with the crown facing downward, minimizing potential image distortion.
Scanning parameters were optimized for mandibular molar anatomy: 50 kVp, 800 μA, 23.5 μm isotropic resolution (voxel size = 23.5 µm), 360° rotation around the vertical axis, 1.8° rotation step, two-frame averaging, and an aluminum filter of 0.5 mm thickness.
The two-dimensional projections were saved in Tagged Image File Format (TIFF). After scanning, specimens were immersed in distilled water and stored in an incubator at 37 °C and 95% relative humidity to preserve hydration until subsequent analyses.
The next stage consisted of reconstructing axial cross-sections from the acquired angular projections using the modified Feldkamp cone-beam reconstruction algorithm implemented in NRecon v.1.6.10.2 (Bruker microCT, Kontich, Belgium). This process resulted in a complete three-dimensional representation of the internal microstructure of each specimen.
Standardized artifact-correction parameters were applied to enhance image quality during reconstruction: Ring artifact correction: level 4 (scale 0–20), Beam hardening compensation: 30% (scale 0–100%), Smoothing: level 6 (scale 0–10), and Contrast histogram range: 0.02 (minimum) to 0.15 (maximum).
The reconstructed axial sections were saved in Bitmap (BMP) format, processed, and analyzed using CTAn v.1.18.8.0 + (Bruker microCT, Kontich, Belgium). Image segmentation was performed through an interactive thresholding procedure, converting grayscale values from the 3D reconstruction into a binary image, where black pixels represented the background and white pixels represented the object of interest. The threshold range was kept constant across specimens to ensure consistent binarization.
The image segmentation was applied to the region of interest (ROI) corresponding to the root canal system (RCS) and root dentin, extending from the cementoenamel junction (CEJ) to the anatomical apex. The Custom Processing tool, with a predefined task list of plug-ins, was used to ensure consistent processing across specimens.
For the RCS, three-dimensional morphometric parameters were obtained: volume (mm3) and surface area (mm2). Subsequently, 3D models were visualized using CTVol v.2.3.2.1 (Bruker microCT, Kontich, Belgium) to assess canal volume.
To enhance internal validity and to reduce the risk of bias, the experimental groups were formed through stratified sampling, ensuring balanced baseline canal volumes across groups and reducing potential bias [6, 25].
After that, specimens were distributed into five experimental groups (n = 10) that were statistically equivalent (p > 0.05), according to the instrumentation system (Table 1).
Table 1 Mean and standard deviation values of root canal volume (mm3) in the experimental groups after sample distributionBiomechanical preparation
A single experienced operator, strictly following the manufacturer’s instructions for each instrumentation system, performed biomechanical preparation of the roots.
All teeth were sound and presented intact coronal structure; therefore, crown sectioning was not required, ensuring standardization among groups.
Conventional endodontic access cavities were prepared using a spherical diamond bur (801L, Jota AG, Rüthi, Switzerland) and an Endo Z bur (Beavers Jet Burs, Morrisburg, Canada) in high-speed rotation (Dabi Atlante, Ribeirão Preto, SP, Brazil) under continuous water irrigation, as described by Ingle (1976).
Each root canal was explored with a #10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) up to the apical foramen to confirm canal patency. The working length (WL) was established at 1 mm short of the apical foramen, using the corresponding coronal cusp as the reference point for each canal: the distal cusp for distal canals, the mesiobuccal cusp for mesiobuccal canals, and the mesiolingual cusp for mesiolingual canals.
Instrumentation was performed with a 6:1 reduction handpiece (Sirona SN 25185, VDW GmbH, Munich, Germany) coupled to an SMR 114058 micromotor (VDW GmbH, Munich, Germany) and powered by a VDW Silver endodontic motor (VDW GmbH, Munich, Germany).
All files were operated with a bidirectional three-wave motion (three up-and-down strokes), maintaining a 5-s activation time per instrument.
Root canal preparation was performed according to the specific sequence recommended for each mechanized system. In BS group (Blue Shaper; Zarc4Endo, Asturias, Spain), instrumentation followed the sequence Z1 (14.02), Z2 (17.02), Z3 (19.05), and Z4 (25.06). In RT group (VDW Rotate; VDW GmbH, Munich, Germany), canals were prepared using instruments 15.04, 20.05, and 25.06. PTU group (ProTaper Ultimate; Dentsply Sirona, Charlotte, NC, USA) was instrumented with the Slider, 20.04, F1 (20.07), and F2 (25.08). In PTN group (ProTaper Next; Dentsply Sirona), the sequence consisted of X1 (17.04) followed by X2 (25.06). WOG group (WaveOne Gold; Dentsply Sirona) was prepared using the single-file technique with WaveOne Gold Primary (25.07).
For all groups, irrigation was performed with 5 mL of 2.5% sodium hypochlorite (NaOCl) between each instrument; for WOG, NaOCl was delivered throughout preparation.
Post-instrumentation micro-computed tomography (micro-CT) analysis
After biomechanical preparation, all canals were dried with absorbent paper points, and the specimens were rescanned and reconstructed using the same acquisition and reconstruction parameters previously standardized (NRecon v.1.6.10.2; Bruker microCT, Kontich, Belgium).
Before qualitative and quantitative analyses, post-instrumentation micro-CT datasets were aligned (co-registered) with their respective pre-instrumentation scans using the co-registration tool in DataViewer v.1.5.1.2 (Bruker microCT, Kontich, Belgium).
Following alignment, image processing and post-instrumentation analysis were performed in CTAn following the same procedures described for baseline analysis. Both pre- and post-instrumentation datasets were binarized through interactive thresholding. From these datasets, two-dimensional morphometric parameters (area, circularity, major and minor diameters, and canal transportation) were obtained at 3, 6, and 9 mm from the anatomical apex.
Three-dimensional morphometric parameters including volume (mm3), surface area (mm2), Structural Model Index (SMI), and percentage of prepared canal walls were calculated for the entire root canal system (RCS). Image co-registration and prepared/unprepared surface computation followed the Bruker Method Note MN110 pipeline: after DataViewer 3D registration, canal masks were generated by interactive thresholding and cleaned with 2D despeckle and 3D morphological operations in CTAn. A one-voxel-thick (1-pixel) pre-instrumentation boundary and a three-voxel-thick (3-pixel) post-instrumentation boundary were used to accommodate potential registration error (± 1 voxel). Voxels of the 1-pixel pre-boundary that spatially overlapped the 3-pixel post-ROI were classified as unprepared surface, whereas voxels of the 1-pixel pre-boundary not included within the post-ROI were classified as prepared (instrumented) surface. Because the pre-instrumentation boundary is a single voxel thick, its voxel count is directly proportional to surface area; therefore, the percentage of unprepared surface was calculated as follows:
$$\% }\, = \,\left( }\_}/} - } - }} \right)\, \times \,00$$
Absolute unprepared area (mm2) was calculated as follows:
$$}\left( }^} } \right)\, = \,\left( }/00} \right)\, \times \,} - }\left( }^} } \right)$$
Image processing parameters (threshold values, despeckle size, and morphological operations) and co-registration settings were kept constant across specimens and logged for reproducibility. Image processing and outcome extraction were performed by operators blinded to the instrument group.
Examiner calibration and reproducibility
Two examiners (J.G.L. and J.V.R.) with experience in bi- and three-dimensional micro-computed tomography (micro-CT) analysis independently performed all image evaluations. Prior to the formal analysis, the examiners underwent a calibration process to standardize the procedures for image segmentation, region-of-interest (ROI) selection, and interpretation of the morphometric parameters derived from the micro-CT datasets. The calibration was conducted using a subset of specimens not included in the final sample. Intra- and inter-examiner reproducibility were subsequently assessed by reanalyzing 20% of the total sample after a 2-week interval. Agreement between examiners and within the same examiner over time was determined using the Cohen’s kappa coefficient.
Statistical analysis
Data from mechanical (cyclic fatigue, torsional, and bending resistance) and micro-computed tomography (micro-CT) analyses were tested for normality (Shapiro–Wilk) and homogeneity of variances (Levene). Intra- and inter-examiner reproducibility were evaluated using the Cohen’s kappa coefficient.
Mechanical data were compared using one-way ANOVA, whereas two-way ANOVA was applied to micro-CT parameters to evaluate the effects of the instrumentation system and section level (3, 6, and 9 mm from the apex). Tukey’s post hoc test was used for multiple comparisons, with the level of significance set at 5% (p < 0.05).
A correlation analysis was performed to evaluate whether the mechanical properties of the instruments influenced the percentage of prepared areas. For this purpose, cyclic fatigue data were correlated with the percentage of prepared canal areas. The Shapiro–Wilk test was applied to the cyclic fatigue and prepared area datasets, confirming the normal distribution of the data. Subsequently, the Pearson correlation test was performed to evaluate the possible interaction between the mechanical properties of the instruments and the percentage of prepared canal areas. All analyses were performed in GraphPad Prism 9.0 (GraphPad Software, San Diego, CA, USA).
The evaluated systems present inherent differences in taper, cross-sectional mass and kinematic mode (rotary vs reciprocating); these characteristics were recorded and are considered in the qualitative and quantitative interpretation of results. Given that taper, cross-sectional geometry and sequence are intrinsically linked to each commercial system in the present experimental design, multi-variable dissociation of these factors was not performed in this manuscript; results are presented as comparative whole-system outcomes. Therefore, the present manuscript intentionally reports comparative outcomes between full commercial systems and frames the interpretation in terms of interaction among design variables (taper, section mass, kinematics, and sequence) rather than asserting isolated causal effects attributable to a single design parameter.



Comments (0)