
Remember me




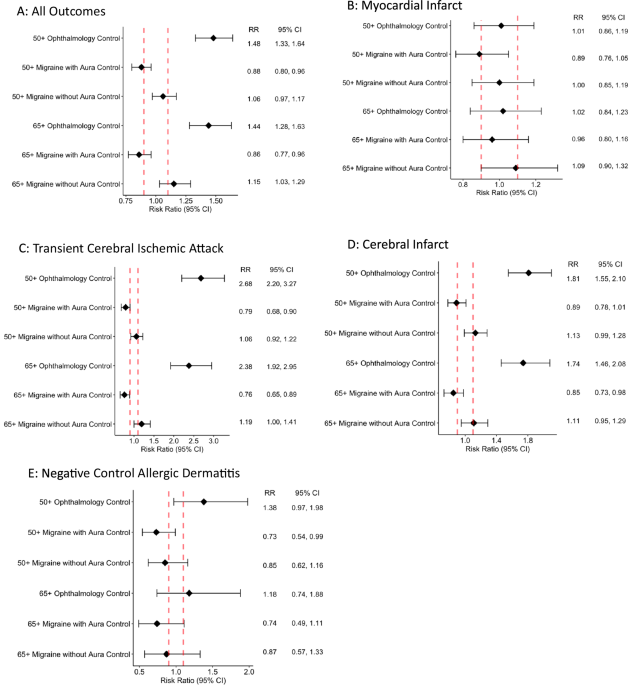
Among those 50 years or older, there were 21,949 patients coded for ocular migraine within TriNetX and 1,492,348 coded as ophthalmology controls. Cohort 1 compared individuals 50 years or older with an ICD code for ocular migraine to ophthalmology controls. After propensity score matching, patients had a mean age of 66.6 years (SD 11.1) with 67% being female. 71% of patients were white, and 6.4% identified as having a Black race. Overall, propensity matching was successful for all variables with standard differences < 0.1 (Table 1). Compared to ophthalmology controls, ICD coded ocular migraine patients had an increased risk of all outcomes with a risk ratio of 1.48 (95% CI 1.33, 1.64) (Fig. 1A). When stratified by outcome, patients with a diagnostic code for ocular migraine had an increased risk of transient cerebral ischemic attacks at 2.68 (2.20, 3.27) and cerebral infarcts at 1.81 (1.55, 2.10) (Fig. 1C, D). Patients with a diagnostic code for was comparable to ophthalmology controls for myocardial infarctions with a risk ratio of 1.01 (0.86, 1.19) (Fig. 1B).
Fig. 1: Risk of Cardiovascular Outcomes in Ocular Migraine Patients Compared to Controls. The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.A–E Risk of Cardiovascular Outcomes in Ocular Migraine Patients Compared to Controls. Forest Plots All Outcomes.
Table 1 Age 50+ Ocular Migraine Compared to Ophthalmology Controls.This analysis was run a second time for individual aged 65 years or older. Again, matching was deemed successful with all values having a standard difference of < 0.01 (Supplementary Table 2). These results were comparable to those of the 50 years + cohort where patients with a diagnostic code for ocular migraine had an increased risk of all outcomes at 1.44 (1.28, 1.63) (Fig. 1A), transient cerebral ischemic attacks at 2.38 (1.92, 2.95) (Fig. 1C) and cerebral infarcts at 1.74 (1.46, 2.08) (Fig. 1D). Overall, ICD coded ocular migraine patients had significantly increased risk of transient cerebral ischemic attacks and cerebral infarcts compared to ophthalmology controls (p < 0.05) (Fig. 1C, D).
Cohort 2 compared ICD-coded ocular migraine patients to patients with MA. For individuals 50 years and older, the average age after propensity matching was 66 (SD 11), with 66% identifying as female. Propensity matching continued to be successful with all comorbidities having a standard difference < 0.1 (Table 2). With all outcomes combined, patients with a diagnostic code for ocular migraine had a comparable risk to MA patients with a risk ratio of 0.88 (0.80, 0.96) (Fig. 1A). Even after stratifying by the different outcomes, ICD coded ocular migraine patients and ICD coded MA patients continued to have comparable risk (p > 0.05) (Fig. 1B–D).
Table 2 Age 50 + Ocular Migraine Compared to Migraine with Aura Controls.Cohort 2 was run a second time among those aged 65 and older. After determining this was a successful propensity match in Supplementary Table 3, the risk ratio of all combined outcomes was again comparable between both ICD coded ocular migraine patients and ICD coded MA patients with a risk of 0.86 (0.77, 0.96) (Fig. 1A). Even after stratifying by type of outcome, the ICD coded ocular migraine and MA groups continued to be comparable (p > 0.05) (Fig. 1B–D).
Cohort 3 compared ICD-coded patients with ocular migraine to patients with MO. Propensity matching was deemed successful with those aged 50 and over. The average age of the cohort was 66, and 67% were female (Table 3). After matching, ICD coded ocular migraine patients had comparable risk of all outcomes to those with MO with a risk of 1.06 (0.97, 1.17) (Fig. 1A). When stratifying by outcome type, there was no difference between groups (p > 0.05) meaning patients with a diagnostic code for ocular migraine had comparable risk to those with MO for all outcomes (Fig. 1B–D).
Table 3 Age 50 + Migraine without Aura Control.Cohort 3 was run among those aged 65 and older, and propensity matching was successful (Supplementary Table 4). When observing risk of all outcomes, ocular migraine patients had a risk of 1.15 (1.03, 1.29), which was deemed comparable to those with MO (Fig. 1A). When observing each outcome separately, patients with a diagnostic code for ocular migraine continued to have comparable risk to those with ICD coded MO (p > 0.05) (Fig. 1B–D).
Allergic dermatitis was the negative control for this study and showed no difference between groups for all cohort comparisons (Fig. 1E).
Comments (0)