Risk of Bias Within Studies According to Design
Of the 26 included studies, two were categorized as qualitative, three as mixed methods studies, 12 as RCTs, and nine as quantitative non-RCTs. Table 1 summarises the Mixed-Methods Appraisal Tool ratings of each study and the percentage fulfilment of the quality criteria.
Table 1 Characteristics of included studiesThe two qualitative studies met 60% of the quality criteria (Farias et al., 2023; Harris et al., 2012). While the qualitative approach was adequate to address the research questions in both studies, common methodological issues included a lack of sufficient quotations to support the interpretations of results.
Of the three mixed-methods studies, one met seven of the 15 criteria (Saez et al., 2018), one met two (Kennedy et al., 2021), and one met zero (Bukhari et al., 2011). Thus, the quality of these studies was relatively low. All three studies failed to address divergences and inconsistencies between quantitative and qualitative results and did not adhere to the quality criteria of each tradition of the methods involved. Still, the rationale for choosing a mixed-methods design to address the research question was adequate in two of the studies (Kennedy et al., 2021; Saez et al., 2018).
Among the 12 RCTs evaluated, all fell short of blinding assessors and ensuring sufficient participant adherence (follow-up rates below 80% (Hong, 2020)), except for one study (Dohnke et al., 2018). Six of the studies met 40% of the five criteria (Collins et al., 2014; Dowling et al., 2019; Lubans et al., 2012; McCabe et al., 2015; Morgan et al., 2012; Smith et al., 2018). In five of the studies, the randomization was performed adequately (Christensen et al., 2019; Dowling et al., 2019; Kennedy et al., 2018; Lubans et al., 2012; Smith et al., 2018), but seven studies did not describe the randomization sequence generation (Ariza et al., 2013; Casey et al., 2014; Collins et al., 2014; Dewar et al., 2013; Dohnke et al., 2018; McCabe et al., 2015; Morgan et al., 2012). A few studies met only one criterion, and all of these were lacking complete outcome data (Christensen et al., 2019; Dewar et al., 2013; Dohnke et al., 2018; Kennedy et al., 2018).
In none of the nine non-randomized studies, participants were described as representative of the target population (Alliott et al., 2023; Bast et al., 2021; Bishop et al., 2018; D’Adamo et al., 2016; Foley et al., 2017; Geria & Beitz, 2018; Harrington et al., 2020; Mikkelsen et al., 2021; Shifts & Townsend, 2012), and all studies except one (Harrington et al., 2020) reported complete outcome data. Four studies fulfilled two out of five quality criteria (40%) (Bast et al., 2021; D’Adamo et al., 2016; Foley et al., 2017; Harrington et al., 2020), and three fulfilled one criterion (20%) (Alliott et al., 2023; Bishop et al., 2018; Shifts & Townsend, 2012). Two studies met zero criteria (Geria & Beitz, 2018; Mikkelsen et al., 2021). Only three studies accounted for confounders in the design and analysis of the study (Bishop et al., 2018; Dewar et al., 2013; Foley et al., 2017).
Risk of Bias Across Studies
Overall, the studies included varied widely in quality, as assessed according to the MMAT criteria. Of the 26 included studies, none were of high quality (80–100% criteria met) and low risk of bias, 13 studies (42%) were of moderate quality (40–60% criteria met) (Bast et al., 2021; Collins et al., 2014; D’Adamo et al., 2016; Dowling et al., 2019; Farias et al., 2023; Foley et al., 2017; Harrington et al., 2020; Harris et al., 2012; Lubans et al., 2012; McCabe et al., 2015; Morgan et al., 2012; Saez et al., 2018; Smith et al., 2018), and 13 (57,69%) were of low quality (below 40% criteria met) and high risk of bias (Alliott et al., 2023; Ariza et al., 2013; Bishop et al., 2018; Bukhari et al., 2011; Casey et al., 2014; Christensen et al., 2019; Dewar et al., 2013; Dohnke et al., 2018; Geria & Beitz, 2018; Kennedy et al., 2021; Mikkelsen et al., 2021; Shifts & Townsend, 2012; Smith et al., 2018).
Due to the inconsistent reporting and lack of adherence to key methodological components across the qualitative, quantitative, and mixed-methods studies, the overall risk of bias, such as selection bias, was high, limiting the studies’ internal validity.
Synthesis of the EvidenceCharacteristics of Studies
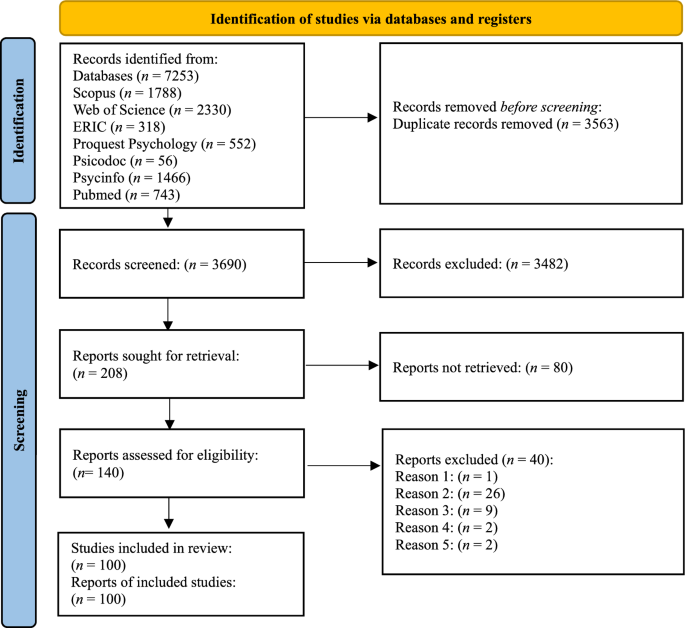
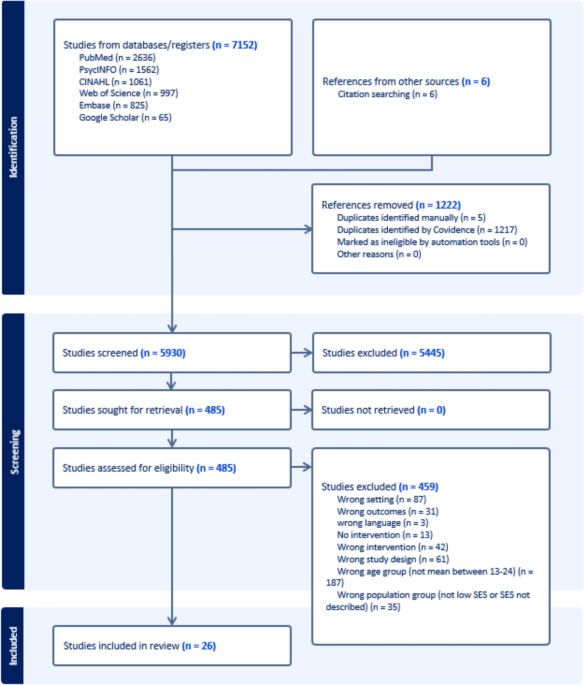
This review included 26 interventions conducted in school settings that targeted socioeconomically disadvantaged adolescents across various countries (one in the UK, one in Spain, three in Denmark, six in the USA, 11 in Australia, one in France, one in Germany, one in Ireland, and one in Sweden). A total of 11,009 students were included in the studies, and the sample sizes varied from 16 to 2,995 students, with 45.6% being male across studies, ranging from 0 to 100% (Table 1). Most studies targeted 13–16-year-olds, however, a few studies included participants extending into emerging adulthood. School types included mainly high schools, secondary schools, and post-primary schools, with only four studies (15.38%) conducted in middle school (1), college (1), and vocational schools (2). Students were commonly enrolled in grades 8, 9, or 10.
Intervention Characteristics and Outcomes
The interventions varied widely in terms of duration (two weeks to two years), content, and aims (Table 2), and targeted a range of health behaviors:
Physical activity: Four studies (15.4%) (Alliott et al., 2023; Kennedy et al., 2018, 2021; Morgan et al., 2012).
Dietary behavior: Seven studies (26,9%) (Bukhari et al., 2011; Christensen et al., 2019; Collins et al., 2014; D’Adamo et al., 2016; Dohnke et al., 2018; Harrington et al., 2020; McCabe et al., 2015).
Mental health and well-being: Two studies (7.7%) (Dowling et al., 2019; Smith et al., 2018).
Substance use: Two studies (7.7%) (Ariza et al., 2013; Bast et al., 2021).
Physical activity and dietary behavior: Seven studies (26,9%) (Bishop et al., 2018; Dewar et al., 2013; Foley et al., 2017; Geria & Beitz, 2018; Lubans et al., 2012; Saez et al., 2018; Shifts & Townsend, 2012).
Physical activity and mental health: Three studies (11.5%) (Casey et al., 2014; Farias et al., 2023; Harris et al., 2012).
Physical activity, dietary behavior, and substance (ab)use: One study (3.9%) (Mikkelsen et al., 2021).
Table 2 Overview of school-based interventions and their health literacy domains (functional, interactive and critical)While the health behaviors are highly relevant to adolescents from socioeconomically disadvantaged backgrounds—who face a higher lifetime risk of non-communicable diseases—the interventions rarely engaged explicitly with health literacy as a relational construct shaped by social, cultural, and economic contexts (Frech, 2012; World Health Organization, 2023). None used validated health literacy instruments, and few described how the intervention was tailored to the needs of adolescents with limited socioeconomic resources.
Several interventions addressed health literacy components such as knowledge and behavioral skills related to dietary behavior or physical activity. Examples include improvements in motivation and self-efficacy regarding physical activity behavior (Kennedy et al., 2018), physical self-worth (Morgan et al., 2012), and food knowledge and attitudes (Geria & Beitz, 2018; Harrington et al., 2020). A smaller subset also incorporated elements of interactive health literacy, such as communication skills and peer engagement, particularly in peer-led models like the ‘SALSA’-intervention (Foley et al., 2017). However, critical health literacy—involving the capacity to reflect on and act upon health information and its broader determinants—was almost entirely absent.
Many interventions employed multi-component strategies, combining educational content with practical, hands-on learning. For example, the Spice MyPlate intervention combined cooking classes and nutrition education to improve dietary behaviors and attitudes (D’Adamo et al., 2016).
The most frequently cited theoretical framework was Bandura’s Social Cognitive Theory (Collins et al., 2014; Dewar et al., 2013; Foley et al., 2017; Kennedy et al., 2018; Lubans et al., 2012; McCabe et al., 2015; Mikkelsen et al., 2021; Morgan et al., 2012; Shifts & Townsend, 2012). Other common frameworks included the Social Ecological Model (Bukhari et al., 2011; Casey et al., 2014; Farias et al., 2023) and Self-Determination Theory (Farias et al., 2023; Kennedy et al., 2018, 2021). The theories were mainly utilized in the development process of the interventions, with limited attention to the implementation among low-SES adolescents.
Fifteen quantitative studies reported statistically significant associations between at least one exposure and one health outcome (Alliott et al., 2023; Ariza et al., 2013; Bukhari et al., 2011; Christensen et al., 2019; D’Adamo et al., 2016; Dowling et al., 2019; Foley et al., 2017; Geria & Beitz, 2018; Harrington et al., 2020; Kennedy et al., 2018, 2021; Lubans et al., 2012; McCabe et al., 2015; Morgan et al., 2012; Shifts & Townsend, 2012). However, these results must be interpreted with caution. Methodological quality was generally low, health outcomes were inconsistently defined, and follow-up periods were short. Critically, no study directly assessed health literacy or examined whether outcomes varied by socioeconomic status.
Qualitative studies indicated that schools are appropriate settings for reaching disadvantaged adolescents (Farias et al., 2023; Harris et al., 2012). However, one study reported that while low-SES students participated more actively, they primarily used the intervention space for socializing rather than for its intended purpose of homework support—highlighting how contextual factors shape adolescents’ engagement with intervention content (Farias et al., 2023).
Mixed-methods studies generally reported success in improving dietary and physical activity behaviors (Bukhari et al., 2011; Kennedy et al., 2021; Saez et al., 2018). However, implementation challenges were also identified. For example, one study found that only 60% of lessons delivered included at least five of the recommended components (Kennedy et al., 2021), while another highlighted logistical issues and low motivation among participants as barriers to effective delivery (Saez et al., 2018).
Participatory Approaches in School-Based Health Literacy Interventions
Participatory approaches were present in 22 of 26 interventions (84.62%) (Table 3), typically involving teachers, students, or other school staff at various stages of the intervention process. Methods to involve participants included intervention delivery, data collection, recruitment, peer leadership, development of content, and management of logistics.
Table 3 Roles and responsibilities of participants in interventions using participatory approachesIn most interventions, the teachers facilitated the delivery of activities, e.g., leading physical education lessons, conducting workshops, or coordinating lunch or breakfast events (Alliott et al., 2023; Ariza et al., 2013; Bast et al., 2021; Bukhari et al., 2011; Casey et al., 2014; Collins et al., 2014; Dowling et al., 2019; Farias et al., 2023; Kennedy et al., 2018, 2021; Lubans et al., 2012; Mikkelsen et al., 2021; Smith et al., 2018). Teachers were sometimes involved in the evaluation processes, such as handling data collection among students (Bast et al., 2021; Mikkelsen et al., 2021) or providing weekly feedback on the feasibility of sessions (Bukhari et al., 2011). Peer-to-peer approaches were often utilized in the implementation phase across the interventions included in this review (Alliott et al., 2023; Bishop et al., 2018; Collins et al., 2014; Foley et al., 2017; Harrington et al., 2020; Lubans et al., 2012; Saez et al., 2018). However, only a few interventions involved school staff or students in adapting content to local needs and contexts (Bishop et al., 2018; D’Adamo et al., 2016; Dohnke et al., 2018; Dowling et al., 2019).


Comments (0)