
Remember me
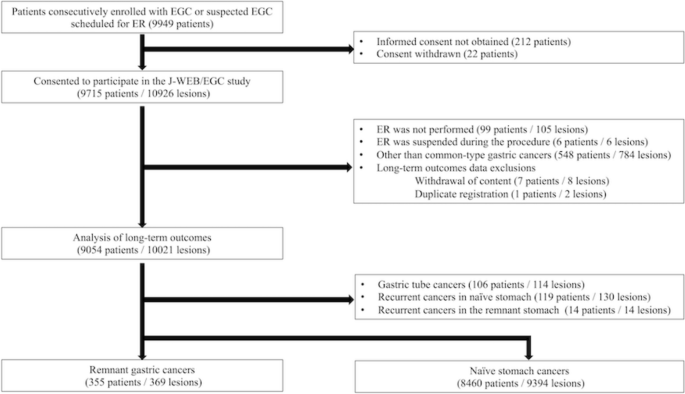
The initial search yielded 2266 records. After removal of duplicates, 1664 titles and abstracts were screened. Of these, 16 full-text articles were assessed for eligibility. The main reasons for exclusion at full-text stage were: focus on subtotal gastrectomy, exclusive use of parenteral supplementation, and lack of clinical outcomes. Studies that did not allow for separate analysis for patients taking oral B12 supplementation were also excluded. The search identified 7 studies that met the eligibility criteria and were included in the analysis. The selection process is illustrated in Fig. 1 (PRISMA-ScR flow diagram).
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.PRISMA-ScR flow diagram showing the study selection process
Characteristics of sources of evidenceSeven studies were included in the review: three retrospective controlled studies, one randomized controlled trial, one prospective controlled study, one prospective observational study, and one retrospective case series, conducted between 2000 and 2025. Sample sizes ranged from 26 to 133 patients, with the study by Aoyama et al. [15] including the highest number of participants receiving oral vitamin B12 (n = 74). Most studies administered mecobalamin daily in doses ranging from 500 µg to 1500 µg, while in the studies by Moleiro et al. and Pimiento the type of cobalamin was not specified [16, 17]. Follow-up duration varied from 3 months to 36 months, with only three studies providing data beyond 12 months. Outcomes were primarily biochemical (serum vitamin B12 levels); however, several studies also assessed hematologic parameters and clinical symptom resolution. Table 1 summarizes the key characteristics of the included studies.
Table 1 Key characteristics of studies on oral vitamin B12 supplementation after total gastrectomyResults of individual sources of evidenceAdachi et al. conducted a retrospective cohort study involving 31 patients with B12 deficiency, who received treatment upon diagnosis. The cohort included 23 men and 8 women, with average age of 57.2 years. Of them, 18 received daily oral mecobalamin in doses ranging from 500 to 1500 µg, while the remaining were treated with intramuscular cyanocobalamin. At the start of the treatment, 78% (24/31) of patients reported deficiency-related symptoms, including fatigue (39%), cold feet or legs (32%), and numbness or dizziness (13% each). Serum B12 levels increased significantly in both groups. No substantial differences were observed between treatment routes. The authors concluded that enteral vitamin B12 supplementation should be prescribed routinely after total gastrectomy, as it rapidly increases serum B12 levels and resolves deficiency-related symptoms [18].
Kim et al. [19] conducted an open-label, single-center, prospective controlled study comparing the efficacy and safety of 1500 µg of oral mecobalamin daily for 3 months with a standard intramuscular protocol in groups with 30 patients with B12 deficiency each, irrespective of deficiency-related symptoms. In all patients, serum B12 levels normalized by day 90. In the oral group, the authors observed a continued increase of serum B12 levels, while in the intramuscular group, B12 concentration peaked after the weekly boosting injection period, decreased at 2 months and stabilized at day 90. In both groups, homocysteine concentrations decreased, and no adverse effects were reported. Interestingly, in the oral B12 group, serum folate level decreased but remained in the normal reference range. At the start of the treatment, 29 of 30 patients had deficiency-related symptoms, all of which resolved after 1 month of oral vitamin B12 replacement. The authors concluded that oral vitamin B12 replacement is an effective and safe treatment for vitamin B12 deficiency after total gastrectomy.
In a retrospective cohort study, Rino et al. [11] evaluated various routes of vitamin B12 supplementation in 73 patients after total gastrectomy. Among them, 28 received daily oral mecobalamin (500–1500 µg), 42 received intramuscular cyanocobalamin (500 µg) every 1–3 months, and 3 received intravenous cyanocobalamin (500 µg) every 1–3 months. Serum vitamin B12 levels normalized in 85.7% (24/28) of patients in the oral group, compared to 76.2% (32/42) in the intramuscular group and 66.7% (2/3) in the intravenous group, with no statistically significant differences between administration routes. After switching all patients to oral supplementation, B12 levels remained subnormal in only 4 patients (5.5%) and subsequently normalized in all after continued therapy. The authors concluded that daily oral vitamin B12 supplementation, typically at 500 µg, may be sufficient and effective for preventing deficiency after total gastrectomy, although they emphasized that replacement therapy is necessary and should be continued long term.
The prospective observational study by Moleiro et al. [16] followed 26 patients, aged 29–79, who received 1000 µg of oral cobalamin daily. At baseline, all patients had normal B12 levels, 17 had previously received intramuscular B12, while 9 had not started treatment. After switching to oral supplementation, B12 levels remained within the reference range throughout the 20 month follow-up in all patients, with no need for intramuscular supplementation. Interestingly, B12 levels increased steadily during the first 12 months and stabilized thereafter. No patient experienced deficiency-related symptoms or supplementation-related adverse events. The authors concluded that oral supplementation is effective and safe after total gastrectomy and should be considered the preferred route in long-term care.
Namikawa et al. [20] retrospective study included 133 Japanese post-gastrectomy patients who underwent Roux-en-Y or double tract reconstruction. B12 deficiency was present in 71.4% (95/133), among whom 46 received oral mecobalamin (500 µg) daily and 23 were supplemented with intramuscular mecobalamin (500 µg) every 3 months. After supplementation, serum B12 levels increased in all patients, irrespective of the administration route. At 3, 6, and 12 months, B12 levels were significantly higher in the oral group than in the intramuscular group. The authors reported significant improvement in anemia parameters following the start of oral B12 and noted no significant differences regarding the red blood cell count, hematocrit and hemoglobin concentration between the two group. The authors concluded that enteral vitamin B12 supplementation might be effective in improving anemia in this patient group.
Aoyama et al. [15] conducted the only randomized, open-label, multicenter, controlled phase II study comparing the efficacy of 500 µg versus 1500 µg of oral methylcobalamin daily in 74 patients with B12 deficiency after total gastrectomy. Of them, 36 were assigned to the 500 µg/day group and 38 to the 1500 µg/day group. After 3 months, serum B12 levels increased in all patients and reached normal levels in 91.7% of patients in the 500 µg group and in 100% of those receiving 1500 µg. Baseline clinical symptoms included primarily tiredness, memory problems, and tingling sensation in the hands or feet. The frequency of deficiency-related symptoms decreased following the supplementation, with no statistically significant differences between groups. Two grade 2 adverse events were reported in the lower-dose group (ileus and anemia), while none occurred in the high-dose group. The authors concluded that, although the primary endpoint was not met, oral vitamin B12 at 500 µg/day appeared as effective and safe as the 1500 µg/day regimen, and noted that the study was prematurely closed due to poor accrual.
In a recent retrospective analysis, Pimiento assessed the efficacy of oral cobalamin 52 patients who underwent total gastrectomy. Initially, oral supplementation alone was started in 43 patients, while two received a combination of oral and intramuscular supplementation, six received intramuscular B12, and one preferred subcutaneous injections. The specific dosages used for oral and parenteral supplementation were not reported. All patients maintained normal or above-normal serum B12 levels, with minimal fluctuation observed between follow-up visits. While oral B12 remained the most common form of supplementation (n = 8/16), some patients were transitioned to other routes by their local providers. There was also no association between the initial B12 administration route, hematocrit, and serum hemoglobin concentration. The authors were unable to report on peripheral neuropathy as a consequence of vitamin deficiency, since most patients received systemic therapy. However, among the nine patients who did not receive chemotherapy, symptoms of peripheral neuropathy did not occur. The authors concluded that oral vitamin B12 administration is a safe, feasible, and convenient long-term supplementation route after total gastrectomy, while emphasizing the need for continued monitoring of B12 levels [17].
Synthesis of resultsDespite notable heterogeneity in study design, population size, and follow-up duration, the studies consistently reported biochemical improvement with oral vitamin B12 supplementation as feasible long-term approach for preventing and managing post-gastrectomy vitamin B12 deficiency (Table 1). Across all seven studies, daily administration of mecobalamin in doses ranging from 500 to 1500 µg consistently led to normalization of serum B12 levels and resolution of clinical symptoms in the vast majority of patients. Early evidence from Adachi and Kim challenged the long-standing view that only parenteral routes were effective, demonstrating that enteral absorption can be sufficient even in the absence of intrinsic factor. Subsequent prospective data (e.g., Moleiro) and long-term retrospective analyses (e.g., Pimiento) confirmed these results in more heterogenous populations. The only randomized study to compare 500 µg versus 1500 µg daily [15] demonstrated a dose-dependent trend favoring 1500 µg, although the difference was not statistically significant. Although 500 µg/day was effective in most cases, the optimal dose remains to be defined in adequately powered trials.
Serum B12 levels generally normalized within 3 months, and adherence, rather than dose, emerged as the primary determinant of success. In comparative studies, oral supplementation was at least non-inferior to parenteral administration, with higher mean B12 concentrations reported in the oral arm (Namikawa et al.). There were no statistically significant differences in biochemical response (e.g. Adachi et al., Kim et al., Rino et al.).
Across the included studies, biochemical deficiency did not always correlate with symptom burden. This was particularly evident in studies by Adachi et al., Kim et al., and Aoyama et al., where baseline symptom burden did not consistently align with serum B12 concentrations. Several patients remained asymptomatic despite low serum B12 levels, whereas others reported fatigue, paresthesia, or cognitive complaints despite biochemical normalization. This inconsistency reflects the well-described clinical-biochemical gap in vitamin B12 monitoring and underscores the need for standardized assessment of both laboratory and symptom-based outcomes. However, clinical outcomes were reported heterogeneously and often descriptively, which limits direct comparison across studies.
Although symptom reporting was inconsistent across studies, improvement was observed when formally assessed. In studies by Adachi, Kim, and Aoyama, fatigue, paresthesia, or cognitive complaints improved following oral therapy, with full resolution in most cases. Hematologic parameters also improved in studies that included such endpoints, particularly in Namikawa et al., where oral B12 was associated with normalization of anemia markers. Importantly, the therapy was well tolerated and no related serious adverse events were reported; only two adverse events occurred in the Aoyama et al. study.
Follow-up duration varied from 3 to 36 months, with sustained normalization of serum B12 observed in long-term studies (e.g., Moleiro, Pimiento). However, several studies lacked detailed symptom tracking, quality-of-life data, or standardized definitions of response. Additionally, the specific form and dose of oral B12 were not always reported, limiting interpretability. Although the included studies consistently reported biochemical improvement with high-dose oral vitamin B12 supplementation after total gastrectomy, the certainty of this evidence is limited. These findings should be interpreted with caution given the methodological constraints of the available studies, including small sample sizes, short follow-up, inconsistent reporting of clinical endpoints, and the predominance of East Asian populations. Further well-designed, long-term studies are required to clarify the role of oral supplementation in routine practice.
Comments (0)