
Remember me
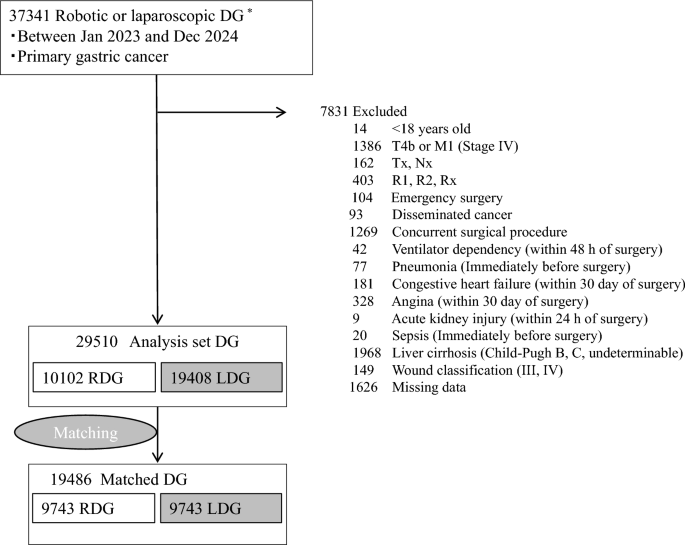
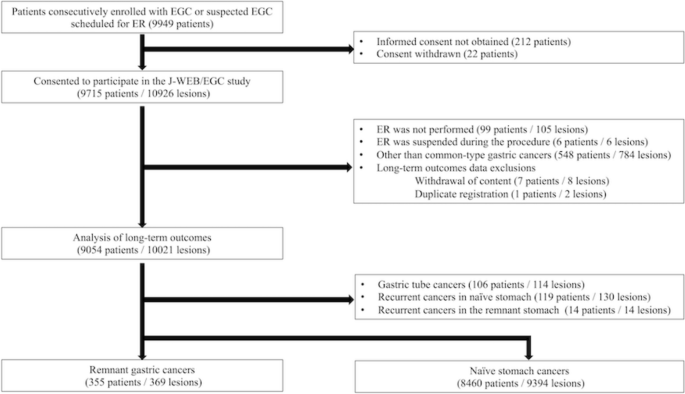
Between December 2018 and March 2022, 47 patients, including 20 patients with BN involvement only, 17 patients with PAN metastasis only, and 10 patients with both BN and PAN involvement, were enrolled in the trial (Fig. 1). One patient was deemed ineligible due to adenocarcinoma with enteroblastic differentiation. The baseline characteristics of the 46 eligible patients are summarized in Table 1. One eligible patient declined protocol treatment before initiation. Among the remaining 45 eligible patients who initiated preoperative DOS chemotherapy, 44 (97.7%) completed three cycles, 43 (95.6%) proceeded to surgery, and 42 (93.3%) underwent R0 resection. Among the 43 patients who underwent surgical resection, the pathological responses of the primary tumor were JCGC grade 3, 2b, 2a, 1b, and 1a in 11 (25.6%), 7 (16.3%), 8 (18.6%), 4 (9.3%), and 13 (30.2%) patients, respectively. Adverse events during preoperative chemotherapy and surgery were previously reported [13]. Among the 42 patients who underwent R0 resection, 40 (95.2%) patients initiated postoperative chemotherapy with S-1, and 30 (71.4%) patients completed postoperative S-1 for 1 year after surgery. Grade 3 or 4 adverse events occurring in more than 5% of patients during postoperative chemotherapy included leukopenia, neutropenia, lymphopenia, and fatigue in 2 (5%), 2 (5%), 4 (10%), and 2 (5%) patients, respectively. No treatment-related deaths were observed during the 3-year follow-up period.
Fig. 1 The alternative text for this image may have been generated using AI.Table 1 Baseline characteristics of the 46 eligible patients
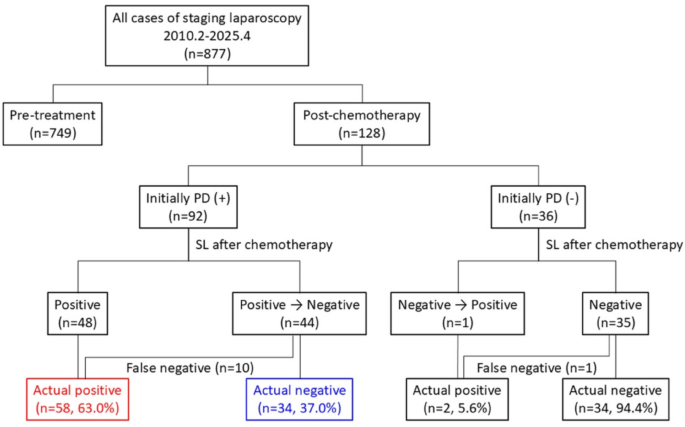
The alternative text for this image may have been generated using AI.Table 1 Baseline characteristics of the 46 eligible patientsAt the data cutoff date of May 2025, the median follow-up duration for OS analysis was 4.2 years (interquartile range, 3.3–5.2 years). Among the 46 eligible patients, the 2- and 3-year OS were 91.1% (95% confidence interval [CI], 78.0–96.6%) and 86.7% (95% CI 72.7–93.8%), respectively (Fig. 2a). Among the 46 eligible patients, the 2- and 3-year PFS were 82.2% (95% CI 67.6–90.7%) and 75.6% (95% CI 60.2–85.6%), respectively (Fig. 2b). Causes of death included disease progression and other causes in 9 and 2 patients, respectively. Among the 42 patients who underwent R0 resection, the 2- and 3-year RFS were 85.7% (95% CI 70.9–93.3%) and 78.6% (95% CI 62.9–88.2%), respectively (Fig. 2c). Recurrence, which was observed in 12 patients, most commonly involved lymph nodes (n = 6), followed by liver (n = 5), and peritoneum (n = 4). Among the 26 patients diagnosed as PAN-positive at enrollment, only three patients were pathologically confirmed to have PAN metastasis after preoperative DOS chemotherapy. In contrast, none of the 20 patients diagnosed as PAN-negative at enrollment were found to have pathological PAN metastasis. One of three pathologically PAN-positive patients developed liver and lymph node recurrence 2.7 months after surgery and died 6.5 months after surgery, another was developed kidney, peritoneal, liver and PAN recurrence 3.9 months after surgery and died 5.5 months, whereas the other patient was alive without recurrence at the last follow-up evaluation 5 years after surgery.
Fig. 2 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Kaplan–Meier curves for overall survival (a) and progression-free survival (b) in eligible patients and relapse-free survival (c) in patients who underwent R0 resection
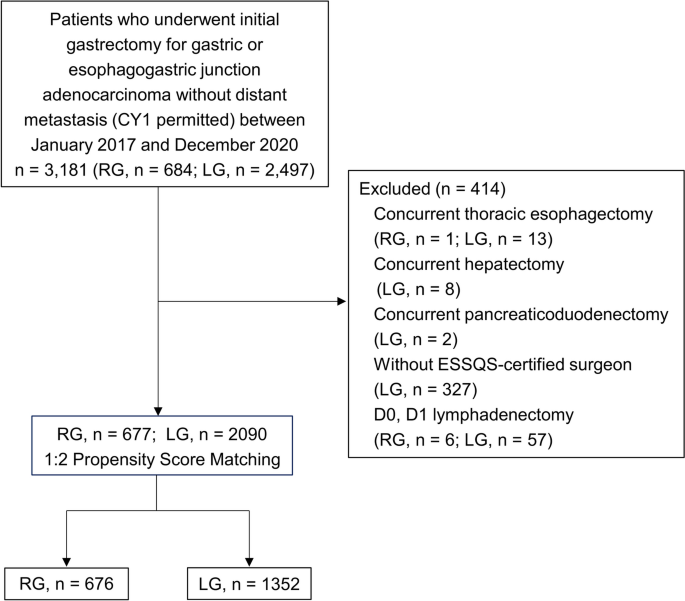
In subgroup analysis of the patients categorized according to the nodal status, the 3-year OS, PFS, and RFS were 85.0% (95% CI 60.4–94.9%), 75.0% (95% CI 50.0–88.7%), and 77.8% (95% CI 51.1–91.0%), respectively, in patients with only BN metastasis; 93.8% (95% CI 63.2–99.1%), 81.3% (95% CI 52.5–93.5%), and 86.7% (95% CI 56.4–96.5%), respectively, in those with only PAN metastasis; and 77.8% (95% CI 36.5–93.9%), 66.7% (95% CI 28.2–87.8%), and 66.7% (95% CI 28.2–87.8%), respectively, in patients with both BN and PAN metastases (Fig. 3).
Fig. 3 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Kaplan–Meier curves for overall survival (a), progression-free survival (b), and relapse-free survival (c) according to clinical lymph node status BN, bulky node; PAN, para-aortic node
In subgroup analysis of the patients categorized stratified by ypN status, the 3-year OS, PFS, and RFS were 94.7% (95% CI 68.1–99.2%), 89.5% (95% CI 64.1–97.3%), and 89.5% (95% CI 64.1–97.3%), respectively, in patients with ypN0; 90.0% (95% CI 47.3–98.5%), 80.0% (95% CI 40.9–94.6%), and 80.0% (95% CI 40.9–94.6%), respectively, in those with ypN1; and 71.4% (95% CI 40.6–88.2%), 57.1% (95% CI 28.4–78.0%), and 61.5% (95% CI 30.8–81.8%), respectively, in those with ypN2-3 (Fig. 4).
Fig. 4 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Kaplan–Meier curves for overall survival (a), progression-free survival (b), and relapse-free survival (c) stratified by ypN status
In subgroup analysis of the patients categorized according to the pathological response based on the JCGC, the 3-year OS, PFS, and RFS were 100% (95% CI 100–100%), 100% (95% CI 100–100%), and 100% (95% CI 100–100%), respectively, in patients with JCGC grade 3 response; 86.7% (95% CI 56.4–96.5%), 73.3% (95% CI 43.6–89.1%), and 73.3% (95% CI 43.6–89.1%), respectively, in those with JCGC grade 2 response; and 76.5% (95% CI 48.8–90.4%), 64.7% (95% CI 37.7–82.3%), and 68.8% (95% CI 40.5–85.6%), respectively, in those with JCGC grade 1 response (Fig. 5).
Fig. 5 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Kaplan–Meier curves for overall survival (a), progression-free survival (b), and relapse-free survival (c) according to pathological response Gr., grade based on the Japanese Classification of Gastric Carcinoma
Comments (0)