Introduction
Small-cell lung cancer (SCLC) accounts for 13–15% of lung-cancer diagnoses but nearly one quarter of lung-cancer-related deaths. Until 2015, the combination of platinum–etoposide chemotherapy, thoracic radiotherapy and prophylactic cranial irradiation (PCI) had kept median overall survival broadly stable at ≈ 12 months in extensive-stage (ES-SCLC) and ≈ 24 months in limited-stage (LS-SCLC) disease. We summarise the key therapeutic advances of the last decade.
Materials and methods
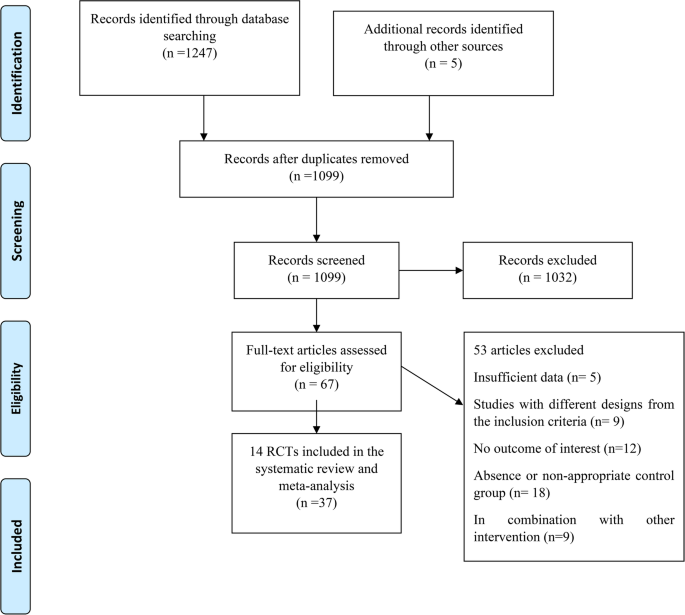
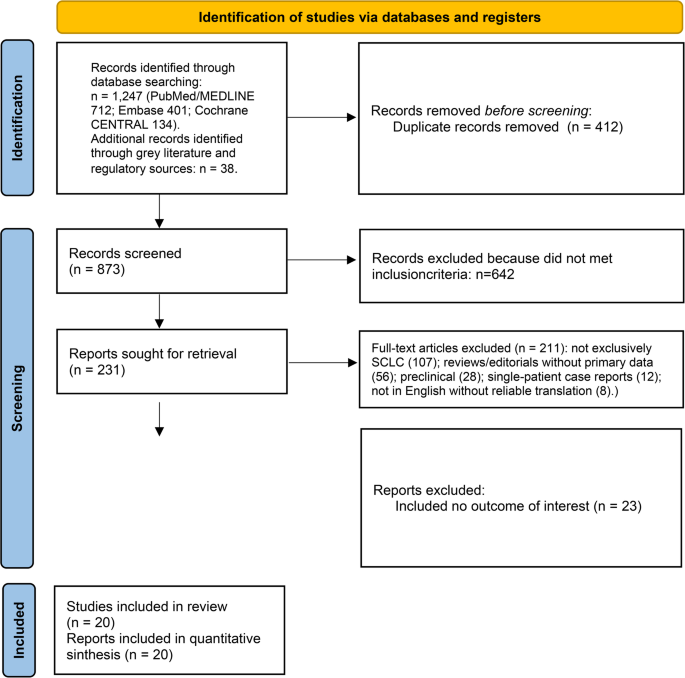
This is a curated narrative review. PubMed/MEDLINE, Embase, ClinicalTrials.gov, FDA and EMA releases and ASCO/ESMO/WCLC abstracts published between January 2015 and May 2025 were searched for phase II/III trials, regulatory approvals and biomarker studies in SCLC. Quantitative pooling was not performed. Practice-changing trials, selected pivotal phase II studies that led to regulatory approval, translational papers that re-defined the molecular taxonomy and informative negative trials were prioritised for in-depth discussion. A PRISMA-style flow diagram (Fig. 1) summarises the selection process.
Results
Consolidative thoracic radiotherapy improved 2-year OS in ES-SCLC responders (CREST: 13% vs. 3%; HR 0.84, 95% CI 0.69–1.01) and brain-MRI surveillance preserved cognition while replacing routine PCI in patients with ES-SCLC who had access to neuro-imaging. IMpower133 and CASPIAN established first-line chemo-immunotherapy: adding atezolizumab or durvalumab to platinum–etoposide extended median OS by ≈ 2–3 months (IMpower133: 12.3 vs. 10.3 months, HR 0.70, 95% CI 0.54–0.91; CASPIAN: 13.0 vs. 10.3 months, HR 0.73, 95% CI 0.59–0.91) and approximately doubled 18-month survival; 5-year OS now reaches 12–13%. Lurbinectedin produced a 35% response rate in platinum-sensitive relapse in a single-arm phase II study; the confirmatory phase III ATLANTIS trial was negative. Trilaciclib reduced severe chemotherapy-induced myelosuppression. Molecular profiling re-segregated SCLC into ASCL1- (SCLC-A), NEUROD1- (SCLC-N), POU2F3- (SCLC-P) and YAP1/inflamed-defined (SCLC-I) subtypes, supporting the development of subtype-directed trials. DLL3 has re-emerged as a target via the bispecific engager tarlatamab (DeLLphi-301: ORR 40%, mDOR 12 months) and next-generation antibody–drug conjugates. In LS-SCLC, durvalumab consolidation up to 24 months after chemoradiotherapy improved median OS from 33.4 to 55.9 months (ADRIATIC; HR 0.73, 95% CI 0.57–0.93). Maintenance lurbinectedin plus atezolizumab more than doubled median PFS after induction chemo-immunotherapy in IMforte (5.4 vs. 2.1 months; HR 0.54, 95% CI 0.43–0.67) and improved median OS (13.2 vs. 10.6 months; HR 0.73, 95% CI 0.57–0.95). Several phase III trials in this period were negative (KEYNOTE-604, CheckMate-451, CheckMate-331, SKYSCRAPER-02, ATLANTIS, TAHOE, MERU).
Conclusions
SCLC therapy has shifted from uniform cytotoxic treatment to a tiered, mechanism-driven algorithm that incorporates PD-L1 blockade, targeted cytotoxics, myeloprotection and refined radiotherapy, raising long-term survival above 20% in selected populations. From a European-practice perspective, current best practice is platinum–etoposide plus a PD-L1 inhibitor for treatment-naïve ES-SCLC, thoracic consolidation radiotherapy in selected responders, lurbinectedin or DLL3-directed clinical trials at relapse, and durvalumab consolidation after chemoradiation in LS-SCLC. Outstanding challenges include a low absolute survival gain from chemo-IO, the absence of validated predictive biomarkers, lineage plasticity, and unequal global access to new agents.

Comments (0)