In recent years, the incidence of ITFs has surged dramatically, with epidemiological studies clearly indicating a significant rise in mortality rates associated with these fractures [11]. Despite numerous studies focusing on perioperative mortality and blood loss risk assessment in ITFs, there remains a notable lack of precise models specifically designed to predict perioperative blood loss risk in patients. Our study aims to fill this gap and facilitate clinical decision-making.
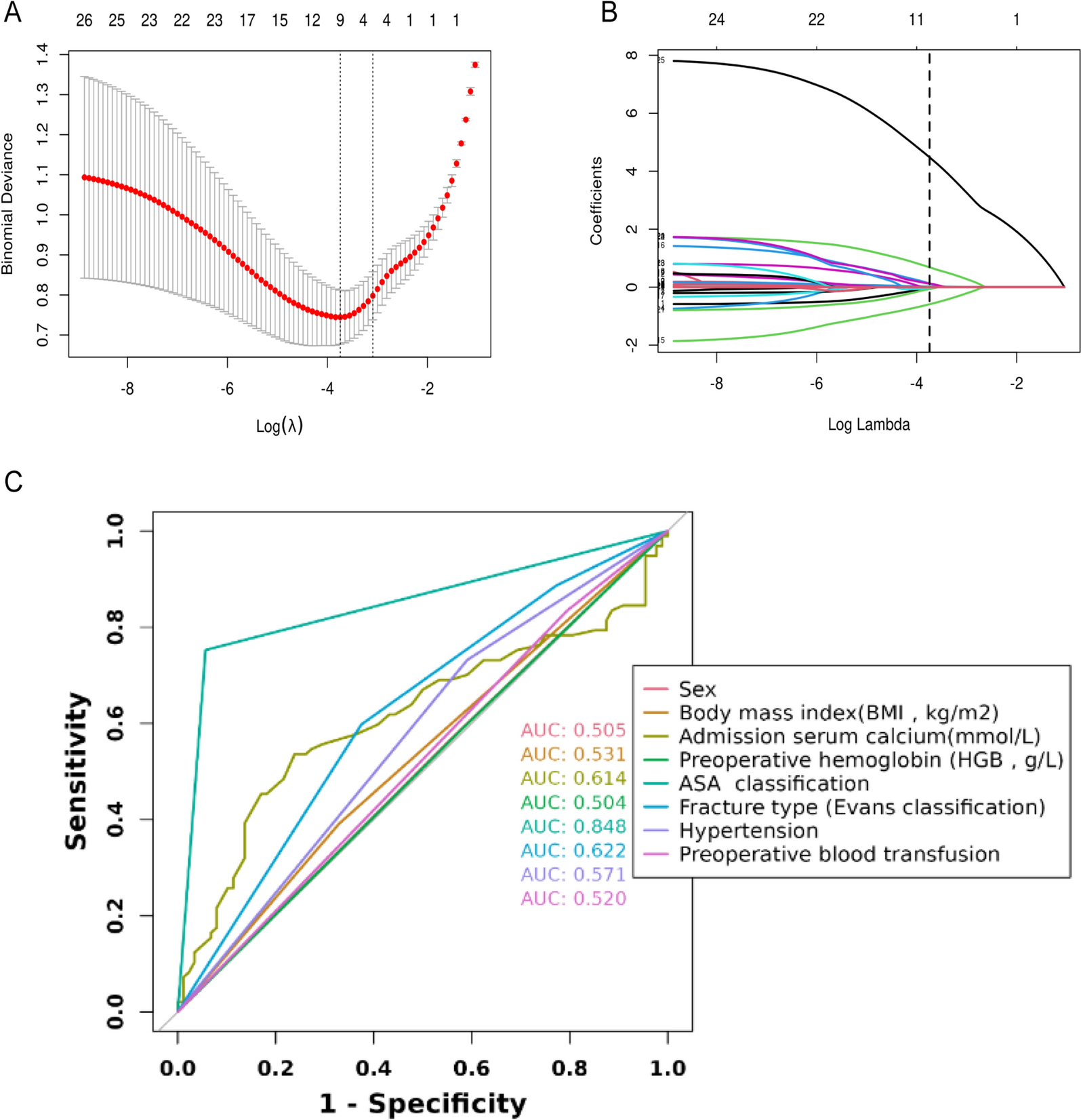
In this research, we meticulously developed a nomogram model comprising eight key predictive factors: sex, body mass index (BMI, kg/m2), admission serum calcium (mmol/L), ASA classification, fracture type (Evans classification), hypertension, preoperative blood transfusion, and preoperative hemoglobin (HGB, g/L). Unlike traditional models that solely incorporate variables with P values less than 0.05 in multivariate logistic regression, our approach comprehensively considered the clinical relevance and effect sizes of each variable. Some variables, although not statistically significant (P > 0.05), were included due to their important clinical implications and underwent rigorous internal validation. Comprehensive assessments using the area under the receiver operating characteristic curve (AUC), calibration curves, and decision curve analysis (DCA) revealed the superior predictive performance and significant clinical utility of our nomogram model. This model enables clinicians to accurately identify patients at high risk of perioperative blood loss, facilitating timely and effective early interventions.
Currently, there is disagreement in the literature regarding sex differences in perioperative hidden blood loss [12]. Our study findings indicate that females are at a higher risk of hidden blood loss compared to males (OR = 0.59; 95% CI 0.19–1.70; P = 0.339). Potential biological mechanisms underlying this gender disparity may include significant bone loss post-menopause in females, leading to increased hidden blood loss post-fracture surgery, and a higher prevalence of obesity among elderly females. BMI, a critical indicator of obesity, indirectly reflects the overall health status of patients. Higher BMI is associated with reduced surgical tolerance, potentially increasing surgical complexity, prolonging operative time, and exacerbating intraoperative soft tissue damage [13]. In our nomogram, patients with BMI ≥ 24 were assigned a higher weight (approximately 21), underscoring the importance of BMI in predicting perioperative blood loss. Therefore, when formulating perioperative blood management strategies, special consideration should be given to gender differences and patients with abnormal BMI.
The ASA physical status classification serves as an essential tool for assessing preoperative health status and surgical risk, providing a scientific basis for surgical decision-making [14, 15]. Patients with higher ASA scores often have multiple comorbidities and poorer prognoses, which may further exacerbate the risk of blood loss. In addition, fracture type (OR = 3.37, 95% CI 0.63–26.25; P = 0.166) and preoperative HGB levels (OR = 1.06; 95% CI 1.02–1.11; P < 0.004) have been established as strong independent predictors of ITFs [16, 17]. Intertrochanteric fractures, compared to other types of hip fractures, typically cause more significant hemoglobin decline due to the rich vascular supply in the intertrochanteric region and the containment effect of the joint capsule in femoral neck fractures [18]. Following intertrochanteric fractures, substantial blood from the fracture site infiltrates surrounding tissue spaces. Unstable fractures imply greater mobility of fracture fragments, complicating surgical procedures, such as intramedullary nailing, where pressure changes during reaming may lead to the release of fat particles from the bone marrow into the vascular system, triggering hemolysis [19, 20].
Notably, our study found that patients without hypertension were assigned a higher weight (approximately 7.5) in the final nomogram compared to those with hypertension, contrasting previous research findings. We hypothesize that this discrepancy may be attributed to structural changes in the vessel wall caused by prolonged hypertension, such as thickening, stiffening, and reduced elasticity, making the vessels less prone to rupture upon trauma. In addition, effective blood pressure control through medication or lifestyle modifications in hypertensive patients may mitigate the risk of tissue damage and bleeding [21,22,23]. Furthermore, serum calcium, a crucial regulator in the coagulation cascade, significantly influences bleeding risk. Calcium ions play a vital role in the timely formation and stabilization of fibrin polymerization sites. Altered calcium levels can impair platelet function and cause vasoconstriction dysfunction, leading to increased bleeding tendency and thrombosis promotion [24, 25]. Literature reports suggest an average increase of 166.5 ml in postoperative blood loss and a significant rise in transfusion requirements in hypocalcemic patients [26]. However, in our study, patients with serum calcium levels ≥ 2.25 mmol/l were assigned a higher weight (approximately 15), potentially related to increased bone resorption and abnormal calcium metabolism in intertrochanteric fracture patients due to immobilization and prolonged bed rest. Currently, research on the relationship between perioperative hypocalcemia, postoperative blood loss, and prognosis remains scarce, posing additional challenges in managing perioperative calcium levels.
However, our study also has limitations. First, being a retrospective study based on data from a single-center hospital system, potential selection bias cannot be fully eliminated. Future studies should include data from multiple institutions for multi-center and external validation to enhance the generalizability and reliability of the findings. Second, due to data accessibility constraints, certain variables potentially influential in perioperative blood loss among intertrochanteric fracture patients, such as dynamic changes in bone density and specific intramedullary nail sizes, were not included in this study. The inclusion of these variables would further refine the predictive model and improve its accuracy.


Comments (0)