
Remember me


We conducted a retrospective analysis of the clinical data from patients who underwent laparoscopic left hemicolectomy between 2013 and 2024. In this study, patients aged 18–90 years, regardless of sex, were preoperatively evaluated through colonoscopy and pathologic examination to confirm the diagnosis of malignant colon tumors. All surgeries were performed by the same group of surgeons. Patients who converted to open surgery, patients who underwent emergency surgery for intestinal obstruction or perforation, and patients who underwent palliative surgery were not included in the study. According to the surgical procedure used, all patients were categorized into either the C-shaped group or the Medial-to-lateral group. Our statistical analysis included patient demographic data, such as sex, age, BMI, tumor invasion status, tumor stage, and tumor location. In addition, we examined surgical safety indices, including total operative time, estimated blood loss, time to first flatus, time to first semi-fluid diet, length of postoperative hospital stay, and incidence of postoperative complications. Furthermore, we assessed surgical quality indices including the number of retrieved lymph nodes, the R0 resection rate, and the CME (complete mesocolic excision) rate. Finally, we analyzed the learning curve of the same surgeon performing these surgeries. Before surgery commenced for each patient, a detailed explanation of the surgical methods and associated risks was provided to ensure informed consent. The retrospective nature of our study has no impact on the treatment plan and outcomes for patients, and due to difficulties in contacting some patients, the exemption from informed consent was approved. This study received approval from the Ethics Committee of the First People’s Hospital of Foshan and adhered strictly to all requirements outlined in the Declaration of Helsinki.
Surgical techniquesC-shaped groupThe patient was placed in the supine position, with legs separated by 45–60°. After the induction of general anesthesia, carbon dioxide was utilized to establish pneumoperitoneum. The arrangement of the trocars and the positioning of the surgeons at different steps are illustrated in Fig. 1. Surgical procedure is illustrated in Fig. 2.
Fig. 1
Preparation for surgery. a Recommended surgical incision. b Recommended surgeons’ position during step 1,4,5,6. c Recommended surgeons’ position during step 2,3. d Recommended surgeons’ position during step 7
Fig. 2
Operation schematic diagram
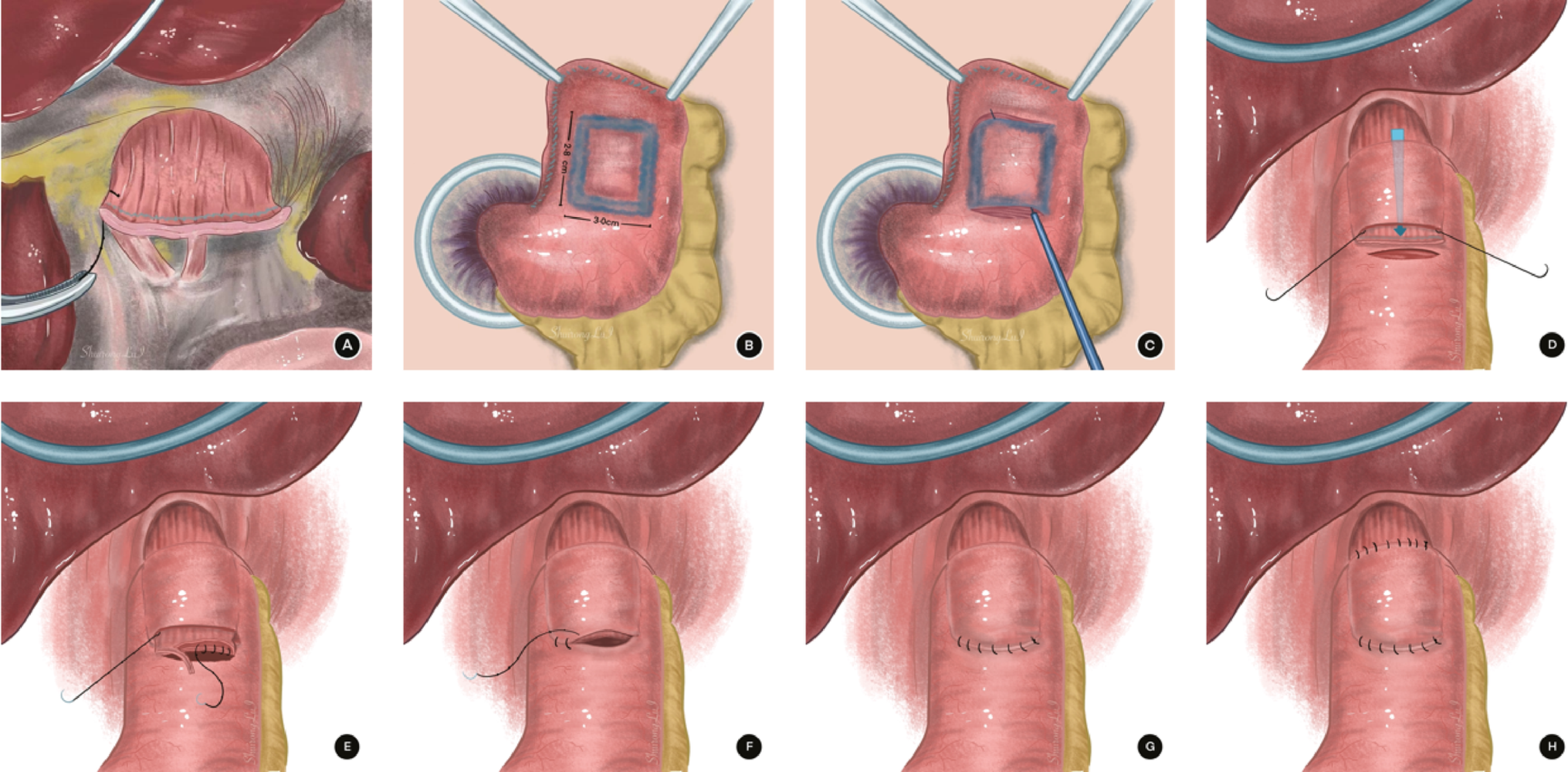
Step 1: The surgeon first exposed and located Treitz’s ligament and IMV first (Fig. 3A). The IMV was then transected, gaining access to Toldt’s space (Fig. 3B).
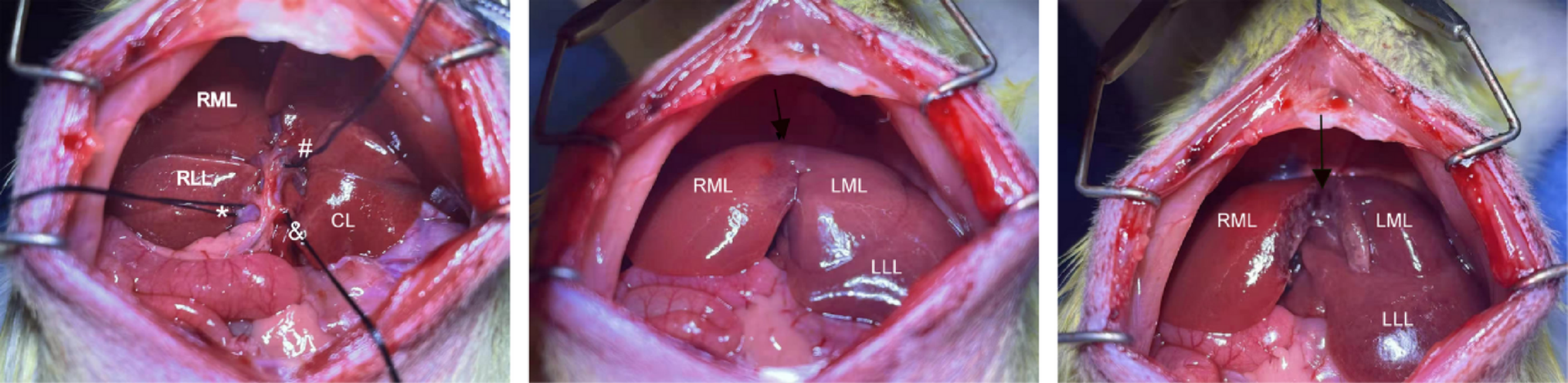
Fig. 3
Surgical Procedure of C-shaped Group. a Locating Treitz’s ligament and inferior mesenteric vein. b entering Toldt’s space. c Entering anterior pancreatic space. d Expanding Toldt’s space and opening lesser omentum. e Dissecting mesentery of the splenic flexure. f Continuing to expand Toldt’s space in the medial aspect of the descending colon. g Dissecting the No.253 lymph nodes and to cut off the blood supply arteries. h Dissecting peritoneum between the descending colon and the abdominal wall and splenocolonic ligament. i Dissecting ligamenta gastrocolicum
Step 2: Further expansion of Toldt’s space toward the cranial direction allowed visualization of the lower pancreatic edge, enabling deliberate dissection of the pancreatic dorsal membrane. Then, the endoscope was advanced through the anterior pancreatic space (Fig. 3C).
Step 3: The anterior pancreatic space was expanded, and the omental bursa was opened (Fig. 3D). Gauze was placed in the omental bursa for position indication. Toldt’s space was further expanded toward the splenic flexure until the mesocolon of the splenic flexure was dissected and exposed spleen (Fig. 3E). Gauze was then placed to indicate the position of the splenic flexure.
Step 4: Inferolateral expansion of Toldt’s space toward the caudal direction continued until the sigmoid colon was reached (Fig. 3F).
Step 5: Identified the root of the IMA (inferior mesenteric artery). In cases where the tumor was located in the splenic flexure, or upper segment of the descending colon, the LCA (left colic artery) was ligated. For tumors located in the middle or lower segment of the descending colon, both the LCA and SA (sigmoid artery) were ligated, or alternatively, the IMA was ligated at its origin. When lesions were located at the descending sigmoid colon junction, the LCA and SA were ligated (Fig. 3G).
Step 6: The left paracolic gutter peritoneum was incised upward toward the splenic flexure (Fig. 3H). For T4 patients, we excised the tumor-invaded portion of the peritoneum or mesentery to ensure radical resection of the tumor.
Step 7: The gastrocolic ligament was incised at the midpoint of the transverse colon, and the gastrocolic ligament, transverse mesocolon, and phrenicocolic ligament were dissected toward the splenic flexure of the colon (Fig. 3I). The splenic flexure and the resection area of the left hemicolon were completely dissected, achieving complete dissociation.
Detailed surgical procedures are shown in supplement files (Online Resource ESM_1).
Medial-to-lateral groupThe surgical procedure was conducted following the classic medial-to-lateral approach technique [16, 17], which can be summarized as follows: the mesentery of the sigmoid colon was opened to access Toldt’s space. The root of the IMA was identified and separated, and the lymph nodes at its base were dissected. Similar to the C-shaped approach, the feeding artery was cut depending on the tumor location. The IMV was then severed. Continuing upward through Toldt’s space, entry into the anterior pancreatic space occurred at the lower edge of the pancreas, followed by expansion along this space toward the spleen until the splenic flexure mesocolon was opened. Full dissociation of Toldt’s space beneath the descending mesocolon was achieved. The subsequent surgical procedure was consistent with step 6 and step 7 of the C-shaped group.
Reconstruction of the digestive tractIn both groups, digestive tract reconstruction was conducted extraperitoneally via isoperistaltic end-to-end, end-to-side or side-to-side anastomosis using the stapler (Table 1).
Table 1 Demographic data and baseline clinical characteristics of patientsPatients in both groups underwent identical postoperative treatment protocols.
Follow-upThe patients were followed up at regular intervals of 1 month for a duration of 3 months post-surgery to evaluate potential early complications. The patients were asked to complete regular examinations of serum tumor markers, chest and abdominal enhanced computed tomography scans, pelvic magnetic resonance imaging scans, endoscopies, and other related examinations.
Statistical methodsThe normality of continuous variables was initially assessed using the Shapiro‒Wilk test and histograms. For normally distributed data, the t test was employed, whereas for non-normally distributed data, the Mann‒Whitney test was utilized. Categorical variables or ranked data were analyzed via the Chi-square test. Specifically, Pearson’s Chi-square test was used when all cells had an expected count greater than 5; otherwise, Fisher’s exact test was used. In cases where multiple independent variables influenced the normal distribution of the dependent variable, multiple linear regression analysis was conducted to determine statistical significance. The intra-group differences among various subgroups within a unified population were analyzed through ANOVA and subsequent post hoc multiple comparisons, with LSD (Least Significant Difference Method) as the comparison method. An inspection level of α = 0.05 and p < 0.05 was considered statistically significant. SPSS 23.0 (IBM, Armonk, NY, USA) was used for statistical analysis of the data.
Comments (0)