
Remember me


A total of 119 female surgeons completed the survey. Thirty-nine respondents were younger than 35 years, 45 were between 35 and 45 years, and 35 were older than 45 years. Twenty-four participants were trainees. Most respondents were general surgeons with a colorectal emphasis (74) followed by colorectal specialists (17), colorectal/proctologic surgeons (20) and proctologists (8). The majority were employed in public hospitals (104). Regarding employment status, 86 participants held fixed-term contracts, 23 reported precarious contracts, and 10 were self-employed. In most surgical units, fewer than five women were present (83 units), and 14 respondents reported being the only woman in their team. In 78 units, the female-to-male ratio was approximately 30%. (Table 1).
Table 1 Demographic and professional characteristics of the participantsWorkload and exposure to operationsNight and holiday duties were commonly reported. Thirty-three respondents spent more than 60% of their working time in the operating room, whereas 36 spent less than 30%. In 60 respondents, non-operative activities accounted for 30–60% of working time. Institutional surgical volumes varied widely. Twenty-four centers reported performing more than five major colorectal procedures per week, whereas 91 reported fewer than five, including 37 centers performing fewer than two. At an individual level, 52 respondents acted as first or second surgeon in fewer than 30% of cases, and 82 were first surgeon in fewer than 10% of major colorectal procedures (Table 2).
Table 2 Workload and surgical activity in the ORCareer satisfaction and assignment of casesSixty respondents reported partial satisfaction with their surgical activity, while 27 were dissatisfied. The remaining respondents reported full satisfaction or did not provide a definite answer. Limited operative opportunities and lack of protected surgical time were the most frequently cited reasons for dissatisfaction. Case assignment was perceived to be influenced by technical competence, personal relationships with senior staff, and availability. Several respondents also reported experiences of sexism, hazing, or restricted access to the operating room. Teaching involvement was limited, with 102 participants spending less than 30% of their working time on tutoring or mentoring activities.
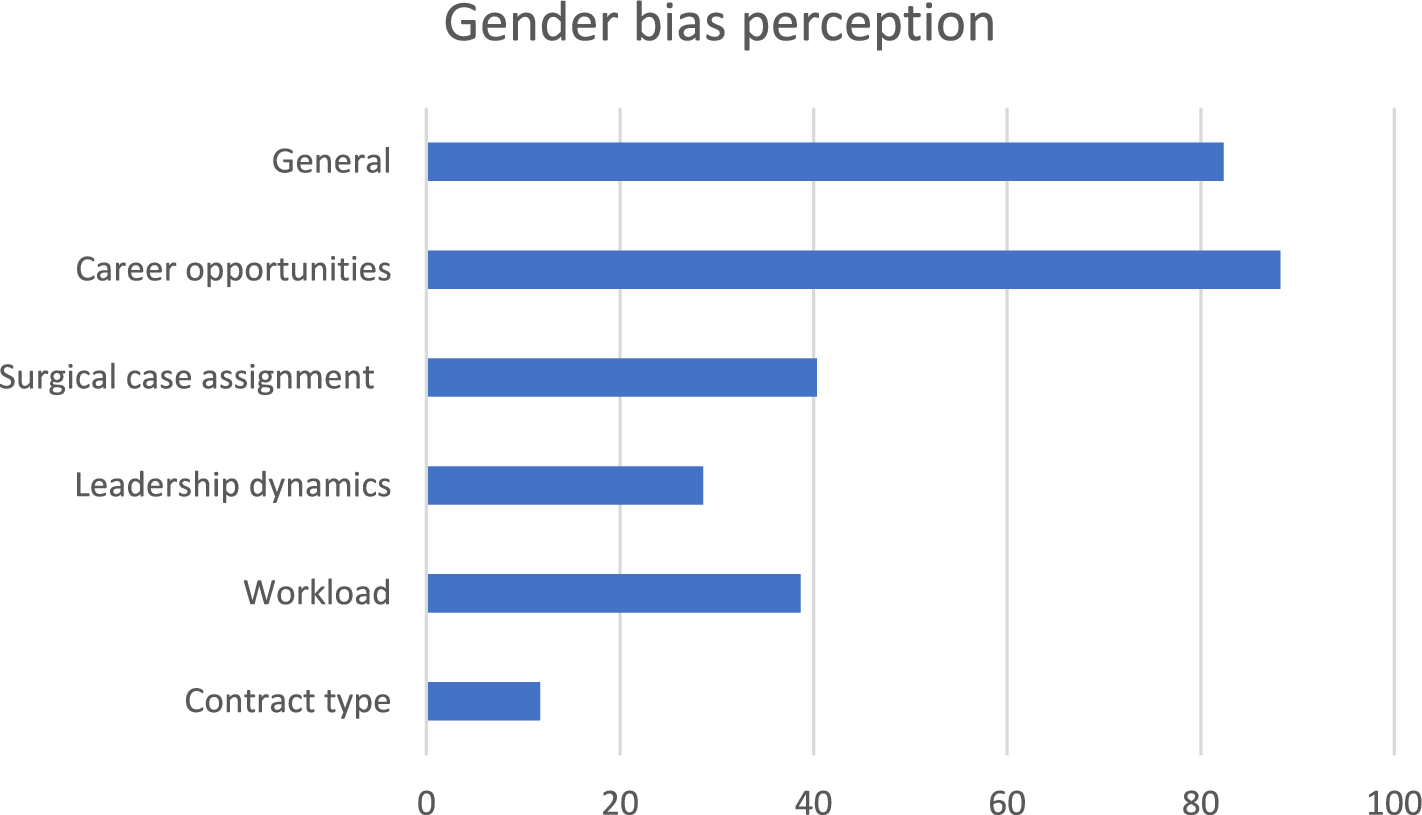
Perceived gender bias and microaggressionsGender-based contractual differences were reported by 14 respondents. A total of 109 participants believed that gender influenced career advancement. (Fig. 1) Differential treatment compared with male colleagues was reported by 92 respondents, particularly regarding access to complex cases, training opportunities, career advancement, and workload distribution. Microaggressions were common. Twenty respondents reported never experiencing them, whereas 19 reported frequent episodes. Most respondents described occasional experiences. (Fig. 2) Common examples included: doubts about technical ability, comments related to gender roles, paternalistic behaviour, exclusion from opportunities, occasional sexual innuendo. Overall, 92 participants reported that these behaviours negatively affected the work environment.
Fig. 1 Fig. 2
Fig. 2
Heatmap: Microaggressions vs Seniority
Workplace infrastructure and ergonomicsInadequate rest facilities were reported by 67 respondents. Ergonomic discomfort with standard surgical instruments was widespread: only 21 respondents felt instruments were adequately sized, while 109 reported difficulties related to ergonomics.
Parenthood and reintegrationSeventy-five respondents had never been pregnant. Among the 44 who had experienced pregnancy, 26 reported delayed return to full duties after maternity leave, and 5 reported no structured or progressive reintegration.
Suggested interventionsRespondents most frequently indicated the need for improved work–life balance (86), leadership opportunities (76), maternity and career policies (68), transparent promotion criteria (67), anti-sexism initiatives (52), and increased visibility at scientific meetings (48). (Table 3).
Table 3 Needs and suggested interventionsStratified analyses by age, career stage, contract type, hospital setting, and surgical involvement revealed significant differences in workload distribution, operative roles, perception of gender bias, and childbearing. (Fig. 3a and b).
Fig. 3
a Stratified analysis by age, career stage, contract type, hospital setting, and surgical involvement. b Stratified analysis by age, career stage, contract type, hospital setting and surgical involvement
Participation as first or second surgeon increased with age (p = 0.002). Satisfaction increased with greater surgical involvement (p < 0.001). Higher operative exposure was associated with lower perceived gender bias in the assignment of surgical cases (p < 0.001) and a reduced impact of harassment on work experience (p = 0.006). Childbearing increased with age and was inversely associated with operative involvement (p = 0.043).
Comments (0)