Robotic surgical management of gallbladder cancer: comparing outcomes and feasibility of hepatectomy with or without bile duct resection and reconstruction
Introduction
Gallbladder cancer (GBC) is an aggressive malignancy, with surgery being the only curative option for resectable cases. Surgical approaches vary based on disease stage, ranging from cholecystectomy to extended liver resection and lymphadenectomy, with or without biliary resection. This study presents our experience of robotic surgery for GBC with and without biliary resection/reconstruction.
Methods
A retrospective analysis was conducted on 38 patients who underwent robotic resection for GBC between February 2016 and November 2024. Beyond the standard partial segment 4B/5 resection and portal lymphadenectomy, the cohort was divided into two groups: common bile duct (CBD) resection and non-CBD resection group. Data are presented as median (mean ± SD).
Results
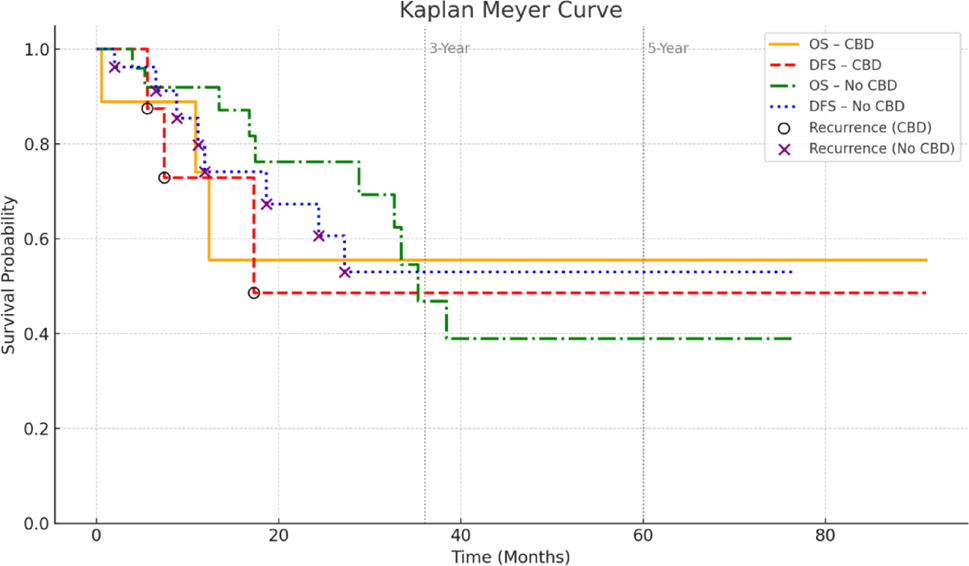
The median age was 68 years (68 ± 11.49), with 71% women. Nineteen patients (50%) were diagnosed incidentally and required subsequent liver resection. Bile duct resection and Roux-en-Y hepaticojejunostomy were performed in 9 patients (23.7%), due to positive cystic duct margins. No conversions to open surgery occurred. Operative time was longer in the CBD resection group (470 vs. 219 min), which also had higher rates of vascular resection (33% vs. 3%), lymphovascular invasion (67% vs. 28%), and node-positive disease (67% vs. 24%), though the latter was not statistically significant. No differences were found in lymph node retrieval [6 (6.21 ± 4.58)], R0 resection rates (95%) or postoperative morbidity.
Conclusion
The higher rates of lymphovascular invasion, vascular resections, and node-positive disease in the CBD resection group likely reflect more advanced disease. Robotic approach for GBC resection is feasible and safe, even when biliary and vascular resections are needed, offering an alternative minimally invasive technique to conventional open surgery.



Comments (0)