Explanation for the choice of comparators
These two teams will be chosen because of their proximity to the area where the study will be carried out and because they are two teams that record a large number of knee injuries and, specifically, ACL injuries.
Intervention description
First, an invitation will be made to all the players who are part of the teams mentioned above during the 2025–2026 preseason with the aim of starting the intervention during that same season. All respondents will receive a Google survey via WhatsApp. This questionnaire will include questions about the inclusion and exclusion criteria to select the study sample of interest as well as questions about their sports background (position, dominant limb, and sports experience); anthropometric measurements (age, height, BMI, and weight), which will be provided by the coaches of the selected teams; and aspects related to training (frequency of weekly training and rest period). After completing the survey, 3 weeks prior to the start of the clinical trial, all players who agree to participate must undergo a final screening to be included in the study. This screening will consist of undergoing a qualitative analysis of the DVJ (Annex VIII), so that, through a simple visual examination, the inclusion of those players who do not present DKV can be ruled out and only those who test positive for DKV can be registered. After selecting the final number of players, a joint talk will be given to both teams to expose the dynamics of the study and the confidentiality of the data. Subsequently, pre-intervention measurements will be carried out by the evaluating physiotherapists to record the initial state of the players. These measures will be: the quantitative analysis of the DVJ, the LESS score, the initial score in the SF-12 scale, the biomechanics of the lower extremities, the muscular activation of the lumbo-pelvic complex, and the lower extremity.
During the 12 weeks that the intervention will last, periodic measurements will be made. The last one will take place 1 month after the end of it. In addition, the players will be asked to refrain from consuming performance stimulants, tobacco or alcohol, non-steroidal anti-inflammatory drugs (NSAIDs), or analgesics 24 h before each session, as well as strenuous exercise. As a reminder, a WhatsApp will be sent to each athlete the day before each session, indicating the time at which they will be scheduled for training the next day. The appearance of pain during the sessions will not be allowed and, if at any time it appears, the training of the player in question will be stopped immediately and recorded for further analysis.
The intervention will consist of performing 3 weekly training sessions for 12 weeks to reach a total of 36 sessions of 30–60 min each. The days that will be set for training will be Mondays, Wednesdays, and Fridays, leaving a rest day between sessions to ensure adequate recovery and quality training. The physical trainers will have to agree so that the training load in both groups is very similar.
Next, we will proceed to detail the intervention that will be carried out in each of the two groups of this clinical trial:
Conventional fitness training group
The players who belong to this group will maintain the usual practice of football training, so no new intervention will be applied.
Training group with a specific ACL injury prevention protocol
This protocol is based on prevention programs that use a multifaceted approach, effective in reducing the risk of ACL injuries compared to those who used only one type of exercise [14, 21, 34]. A wide variety of studies defend the importance of working the muscles of the trunk, hip, and knee to prevent DKV [23, 28, 30]. Therefore, lumbo-pelvic stabilization training (core stability) that includes motor stability and strengthening of the gluteal muscles, in addition to strengthening the lower limb itself, will lead to a significant improvement in neuromuscular control of the lower extremities and trunk in addition to producing a significant decrease in DKV and valgus moments [10, 18, 20, 24, 29, 30, 32].
The proposed exercise protocol will be designed taking into account the inclusion of three main components (Annex IX):
Lumbo-pelvic stabilization exercises.
Lower limb strengthening exercises.
Integration exercises (plyometrics and balance).
The exercises integrated into the program will be organized into three phases of implementation:
The exercises integrated into the program will be organized into three phases of implementation:
Phase 1 (adaptation—1st month): Its objective is that the players learn and integrate new patterns while they train.
Phase 2 (proficiency—2nd month): Aims for players to master new patterns in a controlled environment.
Phase 3 (performance—3rd month): Its objective is to perform exercises in situations as specific as possible and close to the demand and explosiveness of movements typical of the pitch.
During the execution of all the exercises, verbal and visual imputs will be received, such as the presence of a full-body mirror so that they can correct positions and verbal indications focused on lumbo-pelvic stability and the biomechanics of the lower limb to improve the concentration and motivation of the players during the execution of the scheduled exercises [9, 12, 17, 21, 33].
The progression of the exercises will be established by increasing the speed of execution of the same, increasing the complexity of the task to be performed, and by promoting neurocognitive implications (for example, counting backwards from 10 to 0 during the execution of the exercises). In addition, compliance with the proposed protocol will be verified through weekly self-reported questionnaires that will be sent via WhatsApp and will be part of the records to be analyzed later by the evaluators.
Criteria for discontinuing or modifying allocated interventions
The trial may be interrupted at the request of each participating subject due to the appearance of pain or injury during the intervention. On the other hand, an Excel table will be used to record the number of injuries produced, among the players who remain in both groups until the end of the study, and the weekly training frequency.
Strategies to improve adherence to interventions
To improve adherence to the exercise program, each participant will complete an exercise diary during the intervention process in order to analyze the progress of each participant [39, 40, 41].
Relevant concomitant care permitted or prohibited during the trial
The players will be asked to refrain from consuming performance stimulants, tobacco or alcohol, non-steroidal anti-inflammatory drugs (NSAIDs), or analgesics 24 h before each session, as well as strenuous exercise.
Provisions for post-trial care
The protocol does not involve any risks for participants beyond the sporting practice that is not a part of it, since it involves controlled exercises and no dangerous interventions are applied.
Outcomes
The main outcome we expect to obtain from the intervention group is to reduce the incidence of any ACL injury during the application of a specific and comprehensive training protocol focused on players with DKV by recording the presence/absence of injury 6 months after the end of the intervention. Moreover, we expect to obtain a modification of risk factors such as the one mentioned above (DKV) and improve proprioception, body balance, and motor control, not only of the lower extremities, but of the entire lumbo-pelvic complex. In addition, it is expected to improve sports performance and ball control on the pitch.
All changes that occur between the players in the intervention group will be measured and recorded. Changes in the neuromuscular control of the knee and the mechanical behavior of the joints proximal and distal to it [23, 28] will be analyzed with a jump-landing test (DVJ) [19, 27, 28, 32]. Taking advantage of the previous test, the biomechanics of the jump landing will be evaluated and the risk of non-contact injuries will be identified using the LESS scoring system. In addition, during the execution of the DVJ, the data obtained from the activation of the different pre- and post-intervention muscle groups (gluteus maximus and medius of both lower limbs) will be collected and processed with an EMG system [19, 27, 29, 30]. This system will record the maximum contraction of the mentioned muscles in percentages. All these positive changes would imply a lower incidence of injury for the players in the intervention group, as well as higher levels of satisfaction compared to the control group.
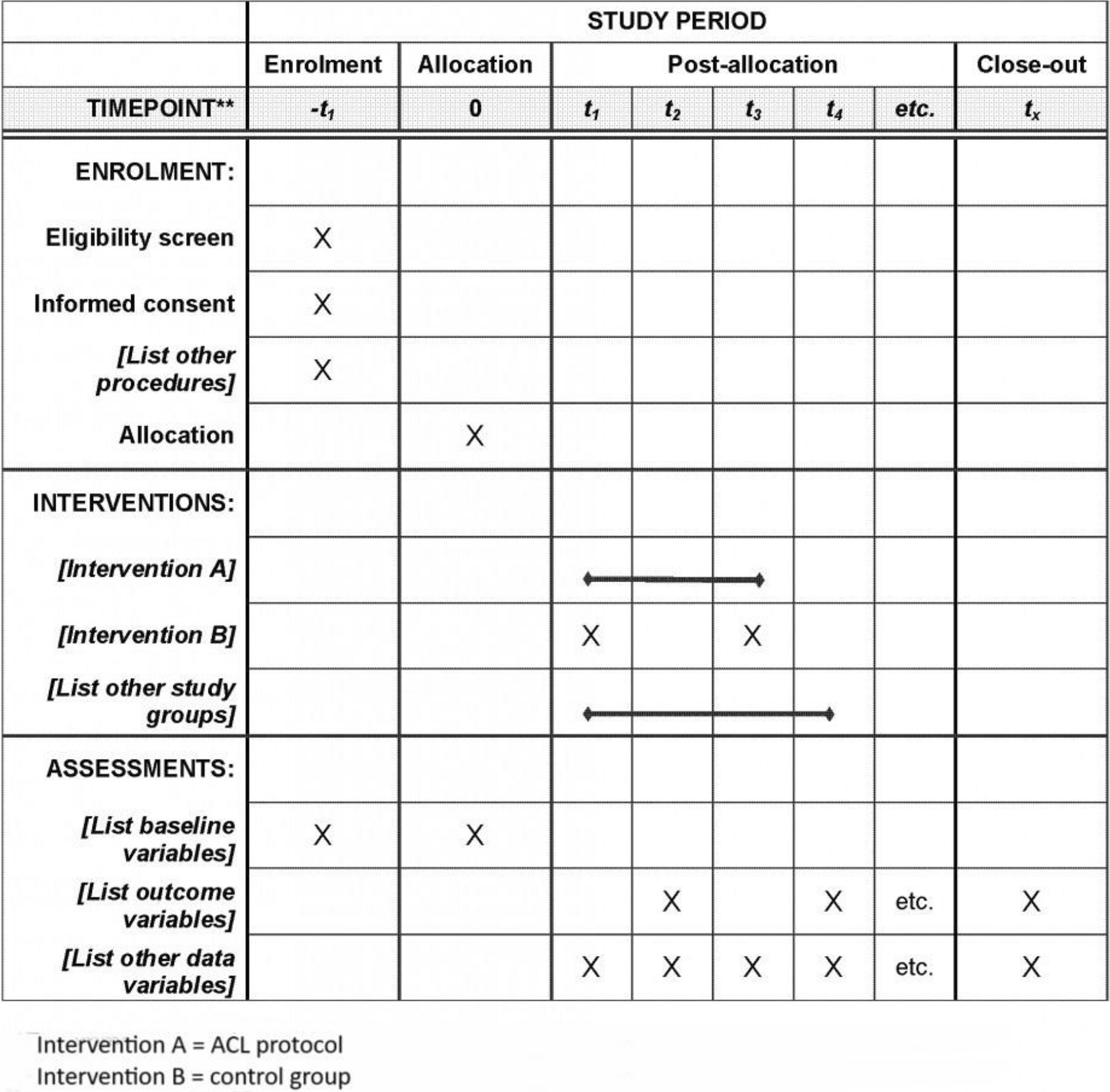
Participant timeline
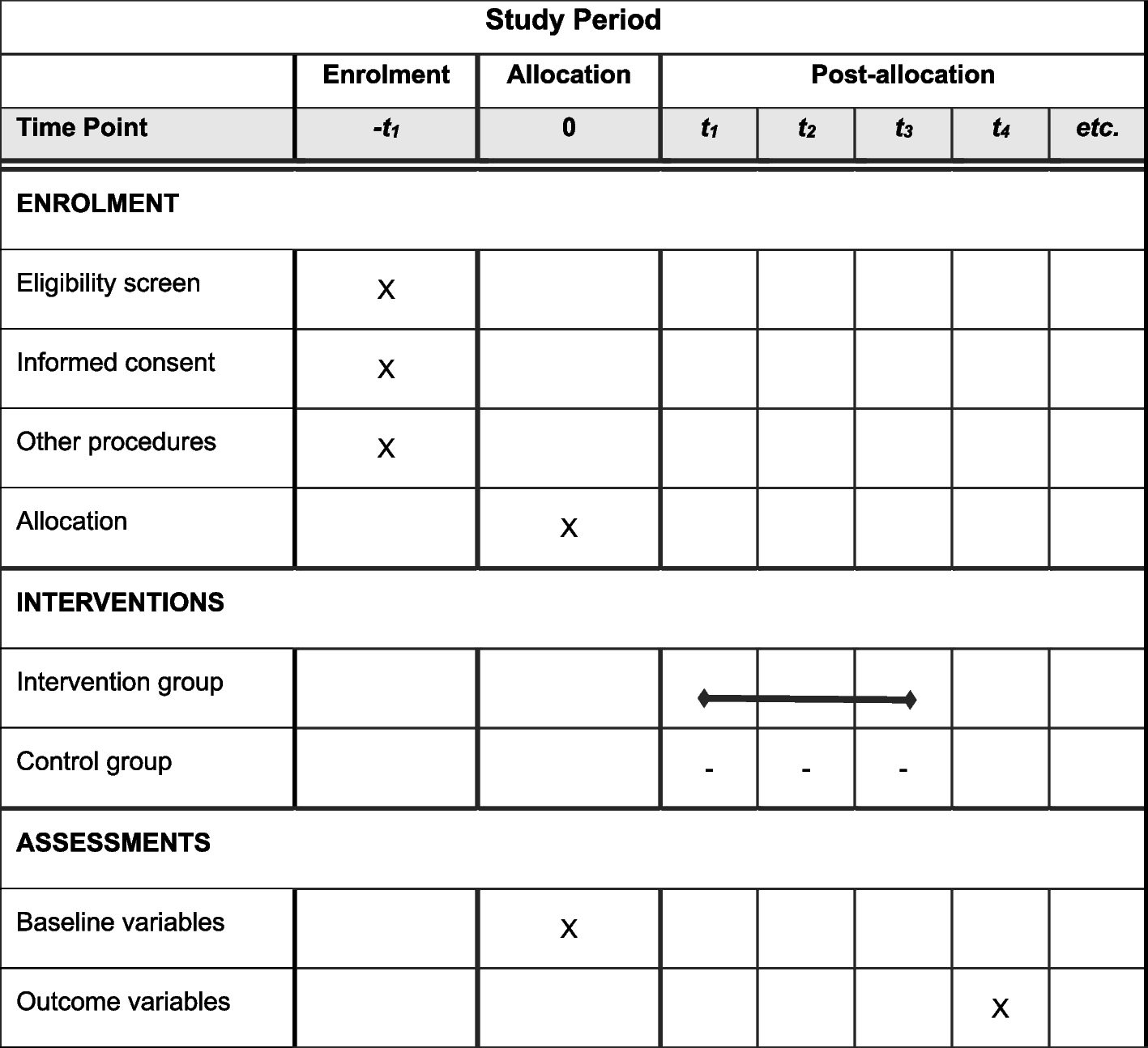
This study will consist of 3 time measurement points, the first prior to the intervention, the second at the end of the 6-week period of intervention, and the last at 6 months after its completion. The study schedule and flowchart are in Annex III and IV, respectively.
Sample size
An analysis was performed with Epidat 4.2 software to calculate the sample size required in the present study. A comparison of independent means will be performed and a standardized mean difference of 1, a significance level of 0.05, a 95% CI, and a power of 90% will be considered, which determines a total sample size of 44 subjects, 22 in each group. It is necessary to consider an abandonment rate, so we will increase the sample by 10%. Therefore, the total sample size will be 48 women, 24 in each study group (Annex VII).
Recruitment
Prior to the collection of data, permission will be requested from the Club and the coach of both teams to carry out the study at the Martínez Valero Stadium in Elche. In the same way, the recruitment will be carried out through a direct contact, such as an interview, with the coach, the physiotherapist, and the physical trainer of the participating teams.

Comments (0)