
Remember me



A prospective RCT involving parallel treatment groups, was carried out in the Physical Therapy/Rehabilitation Department, Banlueam Hospital, Nakhon Ratchasima, Thailand. The study was approved by the Human Research Ethics Committee of Khon Kaen University, Thailand (protocol number HE 602332), was conducted in accordance with the Declaration of Helsinki and each patient gave fully informed written consent of their willingness to participate. The study protocol adheres to the CONSORT 2010 guidelines and the trial is registered with the Thai Clinical Trials Registry (TCTR20210909001).
Participants recruitment/ sample size calculationThe patients who all had PHP were aged between 18 and 60 years and recruited during October 2021 to -September 2022 by a general practitioner working in the outpatient department at Banlueam Hospital, Nakhon Ratchasima, Thailand. Sample size was calculated based on a previous study of morning pain intensity in patients with PHP in which the pooled standard deviation of a numeric pain-rating scale (NPRS) was 2.80 and the mean difference of 2 was considered to be clinically significant. A total of 60 participants (30 per group) would need to be recruited to detect a difference in the effect of the two treatments (active vs. shame US) with a 2-sided t-test, power of 0.8, and α = 0.05 [11].
Inclusion criteria were (i) tender point on the plantar aspect of the heel at the medial calcaneal tuberosity, (ii) history of the pain being worse in the morning when the patient takes the first few steps after waking up or after long period sitting, (iii) tightness or limited ankle dorsiflexion range of motion (evaluated by passive stretching), (iv) active or latent MTrPs in the gastrocnemius or soleus muscle of the calf identified by manual palpation. Exclusion criteria were (i) red flag to manual therapy such as tumor, fracture, rheumatoid arthritis, severe vascular disease or thrombophlebitis, (ii) evidence of neurologic deficit, bilateral plantar heel pain, prior surgery in the lower extremity, diagnosis of fibromyalgia syndrome and (iii) if the patient had received any therapy for their foot pain within the past month. A total of 60 patients were recruited who had PHP affecting either one or both legs.
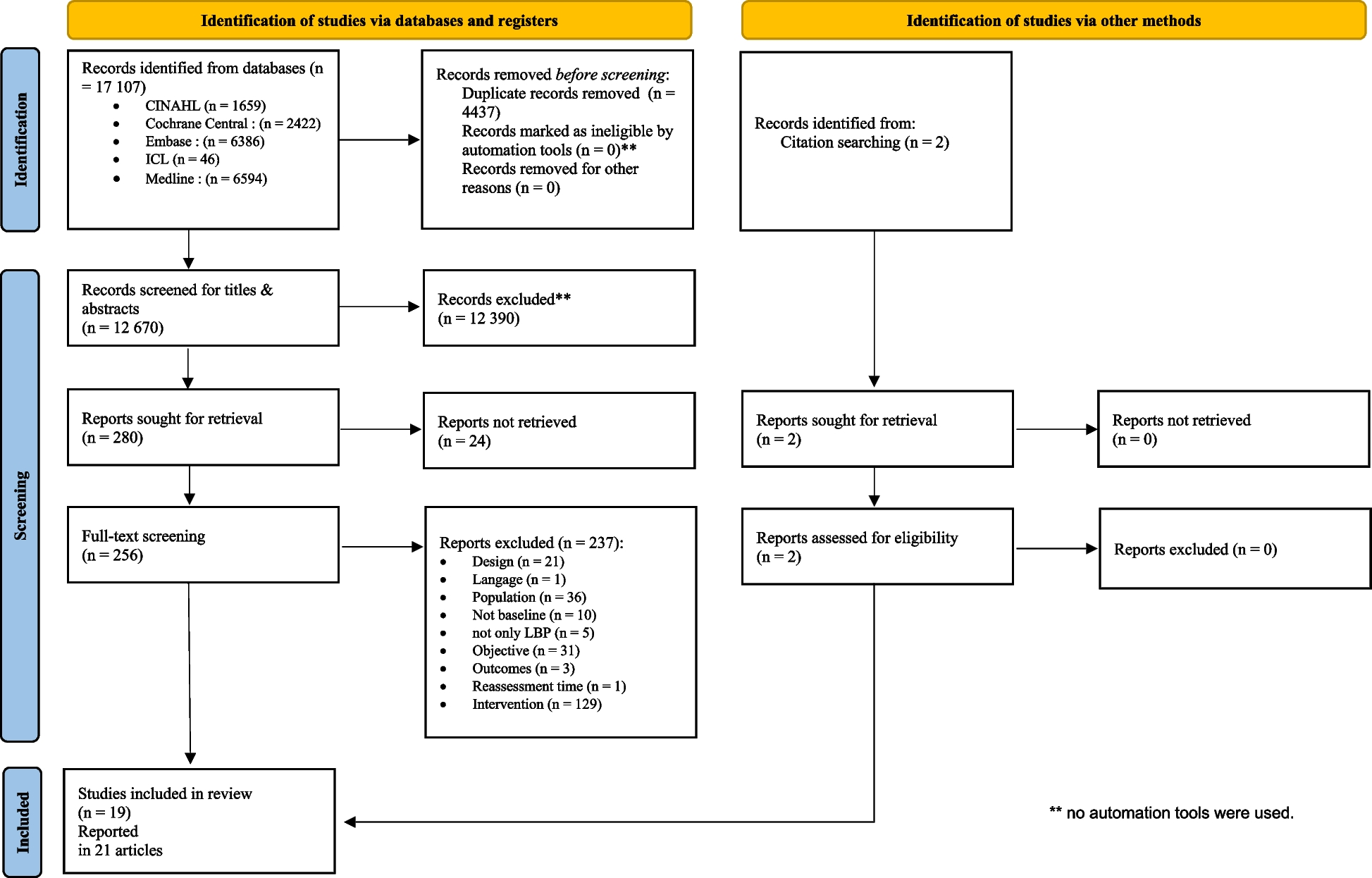
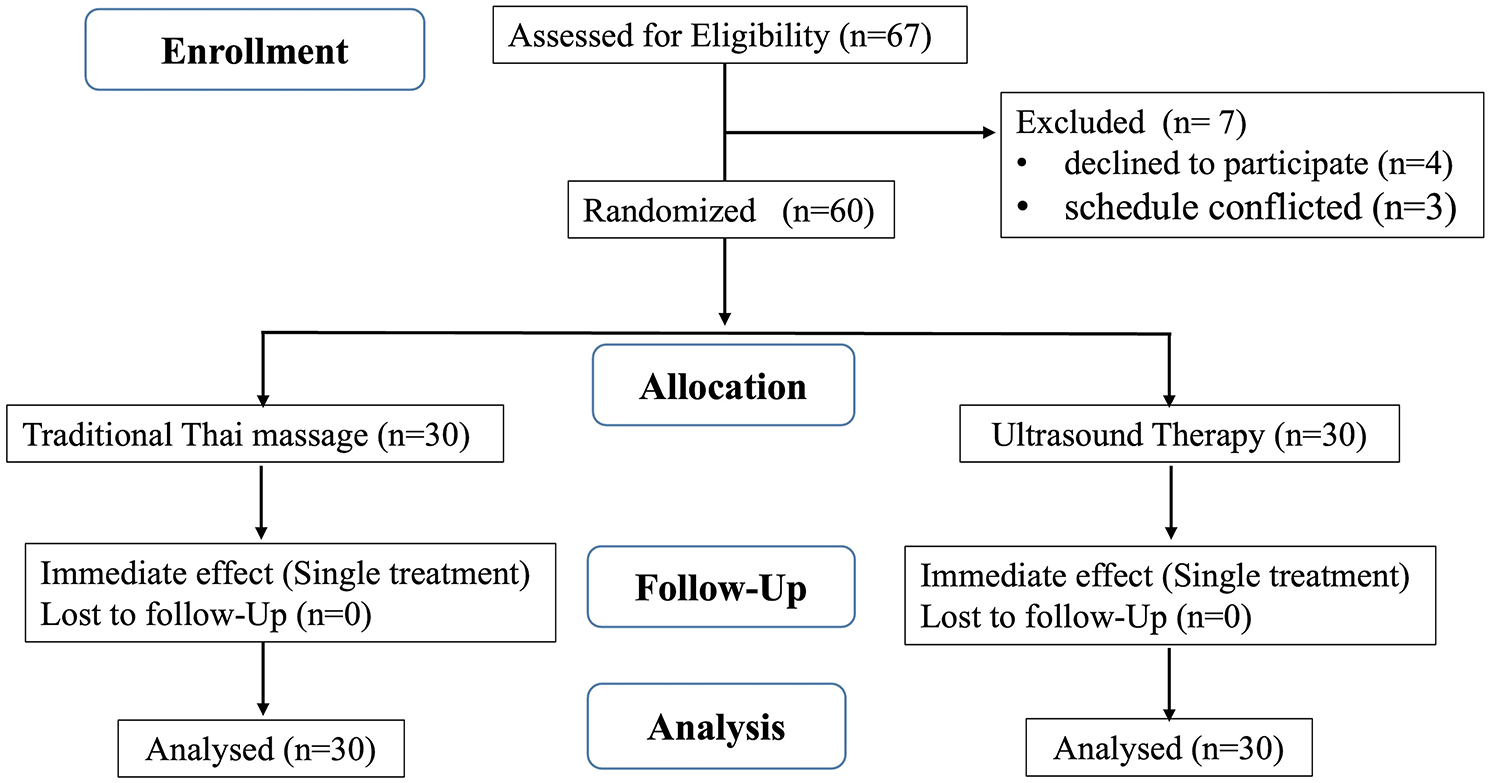
Protocol for study, randomization, and allocation concealmentFigure 1 shows the protocol of this study, after screening the demographic characteristics of the recruited participants were recorded by a general practitioner together with baseline values of the outcome measures. A stratified block randomization approach, with three age groups (18 to 30 years, 31 to 45 years and 46 to 60 years) of both female and male participants, was used to ensure that there were no biases in terms of age or sex when patients were allocated to either US or TTM treatment groups. Random assignment was based on a scheme using sealed envelopes (http://www.sealedenvelope.com) which were prepared by a researcher who assistant but was not directly involved in the study.
Fig. 1
Flow diagram of participant recruitment
InterventionsUltrasound (US) treatment groupThe US treatment which lasted 40 min administered by a physical therapist with over 7 years of work experience. The treatment comprised ultrasound followed by passive stretching (Fig. 2; US1-4). Ultrasound therapy was performed using a Sonopuls 492 system (Enraf-Nonius, Rotterdam, The Netherlands) set to operate in continuous mode, with a frequency of 1 Hz and intensity of 1.5 W per cm2. The ultrasound probe was positioned on the skin directly above the MTrP which had been identified as being located in either gastrocnemius or soleus muscle of the calf and which was likely to produce the referred pain in the heel during standing and walking. After an interval of 5 to 10 min the system was changed to intermittent mode, frequency of 1 MHz and intensity of between 0.5 and 1.0 W per cm2 and the treatment was applied with the new settings to the painful site on the heel for 3 min [18]. After resting for 5 min the patient lay down in a supine position and passive stretching of the calf muscle was performed with the knee in both non-flexed (i.e. leg extended) and flexed positions for a total of 15 min. The static stretching was similar to that used in TTM (see below) and comprised 15 s of stretching followed by 20 s rest with 5 repetitions per set for 2 sets, and with a 10-minute break between the two-stretching positions [14, 19].
Fig. 2
Ultrasound and Tradition Thai Massage treatment protocols. The US protocol comprised four steps. With the patient in prone position (A) US was administered to the calf (US1) and heel (US2) and then with the patient in supine position (B) passive stretching of the calf was performed with the knee in extension (US3) and flexion (US4). The TTM protocol comprised nine steps. Four steps (TTM1-4) were performed with the patient in supine position (A), two (TTM5-6) in side lying (B), two (TTM7-8) in prone position (C), and finally stretching (TTM9) of the calf and foot muscles was performed with the patient in supine position (D). Sen Seb lines are denoted by (---> ). TTM1 = Close-open wind gate (Femoral artery occlusion) denoted by (o); TTM2 = Anterior of upper/lower leg; TTM3 = outer lines of upper/lower leg; TTM4 = Inner lines of upper/lower leg; TTM5-6 = The signal points of leg or “San-yan points” at outer and inner sides of a painful leg denoted by (•); TTM7 = Plantar surface of foot; TTM8 = Back lines of upper/lower leg; and TTM9 = Calf or gastrocnemius-soleus muscle stretching
Traditional Thai massage (TTM) treatment groupTraditional Thai Massage (TTM) treatment was also given in a single 40 min session by a certified and licensed massage therapist. The TTM protocol comprised 9 steps (see Fig. 2; TTM1-9) and was applied specifically to the painful foot and leg, with 35 min devoted to manual massage and 5 min to passive stretching. The massage began with femoral artery occlusion, sometimes referred to as opening the wind gate, lasting 30 to 45 s (Fig. 2; TTM1), and which was followed by gentle massage using thumb and palm with pressure applied at sub-pain levels for 5 to 10 s at points regularly spaced along the relevant Sen Sib lines (Fig. 2; TTM2-4, TTM7-8), with the massage of each line repeated 3 to 5 times [14]. A number of major signal points (San Yan points) were encountered on each line and in these places the pressure was applied for an increased time of 30 to 45 s (Fig. 2; TTM5-6) [20]. Finally, passive stretching of the calf muscle was performed with the leg in an extended position for a total of 5 min (Fig. 2; TTM9), and comprised static stretching for 15 s follow by 20 s rest with 5 repetitions per set for 2 sets [19].
Outcome measures / recording / blindingThe following outcome measures were recorded by a physical therapist with work experience of 10 years and who was blinded to the treatment that the participant received.
Primary outcomeCurrent pain intensity (CVAS)Current pain intensity (CVAS) is the pain patients reported experiencing when asked during the assessment and was measured by using a 10 cm Visual Analogue Scale (VAS) divided into 10 equal intervals and with 0 corresponding to no pain and 10 to the worst pain imaginable. In previous studies this method of measuring pain (CVAS) has been reported to have high intra-rater repeatability with ICC of 0.99 [21] and high concurrent validity [22].
First-step pain intensity (MVAS24)Patients were additionally asked to rate the pain intensity they experienced when taking their first steps after waking or rising from bed in the morning (MVAS24).
Pressure pain threshold (PPT)Pressure Pain Threshold (PPT) was measured by using a Commander TM Algometer and Digi Track (JTECH Medical, Salt Lake City, Utah, USA). The algometer comprises a rubber tipped plunger with area of 1 cm2 which was placed against the skin at the recording site and participants reported when the applied force which increased at a rate of 1 kg per second changed to a feeling of pain. The procedure was repeated three times at 2-minute intervals and the average value was recorded in units of pounds per cm2. The recording sites corresponding to the tender point on the heel of the affected foot and a prominent MTrP in the calf of the same leg were identified by manual palpation and were marked on the body using an ink pen. In previous studies the algometer has been shown to have high repeatability (r = 0.99) [23].
Secondary outcomeAnkle dorsiflexion range of motion (DROM)In order to measure ankle Dorsiflexion Range of Motion (DROM) the participant stood next to a wall and made a weight bearing lunge movement with the leg on the same side as the affected foot. The distance from the wall to the big toe (cm) was recorded using a tape measure. This procedure was repeated three times at 10 s intervals and the mean value was recorded. Intra-rater repeatability of the measurement of DROM has been studied with ICC reported as 0.99 for the left and 0.98 for the right leg [24].
Foot skin temperature (FST)Measurements of Foot Skin Temperatures (FST) were obtained by using Infrared (IR) Thermography. The camera that was used was a Ti10 Fluke Thermal Imaging Camera (Fluke Corporation, Washington, USA) set to operate in the spectral band of 7.5–14.0 μm. Imaging was performed in a quiet room with the temperature set to 25 °C and with an average relative humidity of 38%. Participants lay in a supine position on the examination table with their feet placed on a pillow, and prior to taking the measurements the affected foot was cleaned with a dry towel. The camera was positioned at a distance of 80 cm from the foot and three images were obtained and the average value of FST in the painful area of the heel was recorded. IR Thermography has been reported to have high intra-rater repeatability with ICC of between 0.62 and 0.92 [25].
All outcome measures were recorded at baseline, immediately after treatment, and 24 h after treatment, with the exception of pain intensity, which was measured only at baseline (CVAS) and 24 h after treatment (MVAS24), for the side of the body corresponding to the painful heel. In addition, the pain intensity that each patient experienced when taking their first steps after rising from bed in the morning of the day following treatment was recorded (MVAS24).
Statistical analysisStatistical analysis was performed by using SPSS Version 26 (IBM, Armonk, New York, USA). Intra-rater repeatability of the PPT and DROM outcome measures was assessed. by using the Intra-class Correlation Coefficient (ICC). A two-way repeated measures Analysis of Variance (ANOVA) was performed to evaluate the main effect and potential interaction effects (3 times x 2 treatment groups). If there was an interaction effect, pair-wise comparisons were performed by using post-hoc tests (Bonferroni) to determine the within group effects in each treatment group. In addition, an analysis of co-variance (ANCOVA) was performed to compare post-treatment data between groups using the baseline value as a covariate [26]. Partial Eta square (η2) for ANCOVA, 0.01 (small effects), 0.06 (medium effects) and 0.14 (large effects) were measured [27]. The study followed an intention-to-treat rule which meant that from the beginning until the end of the study, all patients remained in the group to which they were originally assigned.
Comments (0)