
Remember me


A total of 10,019 hospitalized GTC patients (EC n = 2156; GC n = 3057; CRC n = 4806) were included in the analysis (Supplementary Table 2). The average follow-up of patients with esophageal cancer, gastric cancer and colorectal cancer was 31.3 ± 23.7 months, 38.4 ± 24.4 months and 39.0 ± 24.3 months, respectively. The average follow-up time of the total population was 37.2 ± 24.4 months (median 35 months), the longest follow-up was 97 months, and the most times of follow-up visits was seven. There were 2950 (29.4%) patients died during follow-up. The median age at diagnosis was 59 years, and 52.6% were diagnosed at < 60 years; 68.1% were male, and 48.8% underwent surgery. The 1-, 3-, 5-year survival rates of the overall population were 87.4%, 74.7%, and 65.7%.
Comorbidity classesAll models had Entropy > 0.8 and LMR p < 0.001, indicating that the classification accuracy of the models was greater than 90%. Then, we assessed the relative RF of the smallest class for each model and discovered that it was too small in 3-class model (RF = 0.0096) and 4-class model (RF = 0.0026), as detailed in Table 1. It meant that the population was too small to be representative, so we chose the 2-class model.
Table 1 Latent class Model Fit comparison (N = 10019)The median age was not different between the two classes. Class 1 included relatively healthy patients or with fewer comorbidities, accounting for 91.3% of the total population. Among Class 1 patients, 75.2% had no comorbidities, 23.1% had only one comorbidity, and 1.7% had two comorbidities. None of the patients in this group had stroke, myocardial infarction, chronic pancreatitis, osteoporosis, or renal disease. Class 2, although accounting for 8.7% of the total population (870 individuals), was mainly characterized by having multiple comorbidities (Supplementary Table 3 and Supplementary Table 4). Among Class 2 patients, 3.0% had only one comorbidity, 53.7% had two comorbidities, and 22.6% had three comorbidities, and 20.7% had four or more comorbidities. In addition, except for Tuberculosis and Hepatic disease, which were not discriminatory between the two categories, the incidence of comorbidities was much higher in Class 2 than in Class 1. Of these, the incidence of inflammatory bowel disease in Class 2 was 5.2 times higher than that in Class 1, COPD was 8.6 times, diabetes was 10.9 times, and coronary heart disease (CHD) was 23.8 times. KM survival curves showed that the survival of patients in Class 2 was significantly shorter than those in Class 1 (P < 0.001) (Supplementary Fig. 1). The 1-, 3-, 5-year survival rates in Class 1 were 87.6%, 75.0%, 66.6%, and in Class 2 were 85.1%, 71.3%, 55.7%.
To explore the potential differences between comorbidity classes, we conducted univariate analyses targeting other factors (Supplementary Table 5). We found that Class 1 had a significantly higher proportion of males, smokers, and alcohol drinkers, as well as patients with only a compulsory education, with a normal weight, without a family history, and residing in rural areas, compared to Class 2 (all P < 0.001). Class 1 tended to include younger patients, with more than half of the patients being under 60 years old, and only 13.9% were 70 years old or older. In contrast, Class 2 had 33.3% of patients under 60 years old, and a notably higher proportion of patients aged 70 years and older, accounting for 27.9% of the class. And the proportion of retired patients in Class 2 (45.7%) was significantly higher than that in Class 1 (25.6%), which could be explained by the higher proportion of older patients in Class 2. In addition, we found no significant difference in cancer staging between Class 1 and Class 2. And there were more patients with colorectal cancer in Class 2 (P = 0.002).
Training set and validation setThe proportions of training and validation sets were 70.0% (n = 7013) and 30.0% (n = 3006) in the patients. The mean follow-up for the training and validation sets were 37.4 ± 24.3 months and 36.5 ± 24.4 months. There were no significant differences in most baseline characteristics between two cohorts (P > 0.05), suggesting an equilibrium distribution for the two cohorts (Supplementary Table 2). The KM survival curves showed no significant difference in overall survival between the training and validation sets (P = 0.19) (Supplementary Fig. 2), indicating the even distribution between two sets and suitable for internal verification. In the training set, the 1-, 3- and 5-year survival rates for Class 1 were 87.7%, 75.4% and 67.1%, and for Class 2 were 85.3%, 71.4% and 55.3%. In the validation set, the 1-, 3- and 5-year survival rates for Class 1 were 87.4%, 74.1% and 65.4%, and for Class 2 were 84.6%, 71.2% and 56.8%.
Variable selectionThe Lasso method (Supplementary Fig. 3 and Supplementary Fig. 4) was initially employed to reduce the number of candidate variables, resulting in the selection of 10 from the original 25, including age, smoking, NRS2002, KPS, stage, cancer type, histological type, the number of metastatic organs, surgery, and comorbidity classes. The results of the Cox regression analysis of these factors, as illustrated in Table 2, indicated that comorbidity class was an independent risk factor for predicting patient outcomes.
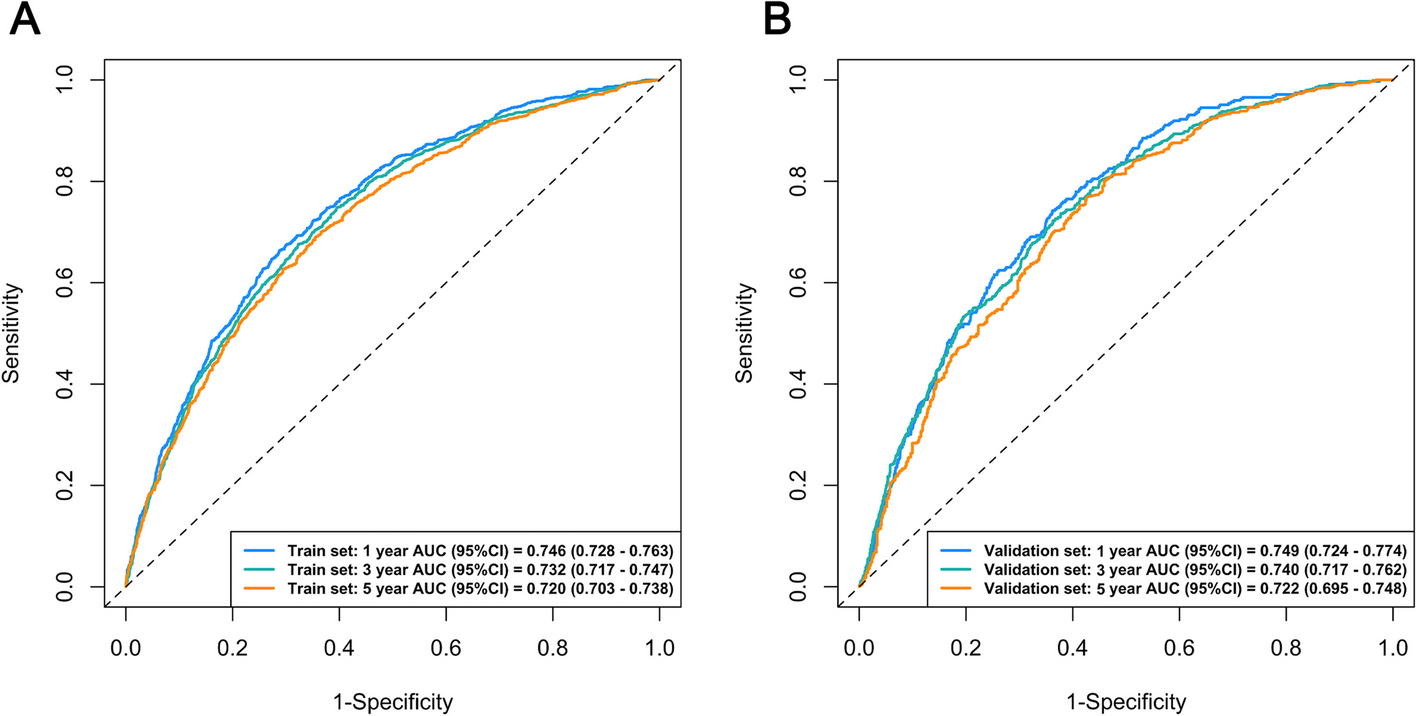
Table 2 Univariate and multivariate analysisComparison of comorbidities measuresWhether in the training or validation set, the final model has the highest AUC of the ROC curve, (Fig. 1), the lowest BIC, and the highest C-index (Table 3). These results suggest that the comorbidity classes offer a better performance than the basic measures.
Fig. 1
ROC for training set (A) and validation set (B)
Table 3 Comparison of different comorbidity measuresCharasteristics of final model with the comorbidity classesThe nomogram (Fig. 2) provides an integrated perspective to evaluate the impact of different factors on the survival of cancer patients, helping to guide clinical decision making and patient management. The points on the calibration plot generally fall along the 45-degree line, indicating that the predicted probability of survival closely matches the actual probability of survival, which suggests that the model predicts correctly (Fig. 3. A-C). The decision curve (Fig. 3. D-F) showed different net benefits of the model at different threshold probabilities at 1, 3 and 5 years, which helped clinicians to make decisions accordingly.
Fig. 2
Nomogram based on final model with the comorbidity classes Note: The steps on how to read and calculate the total integral of a nomogram: 1) Determine the specific value of each prognostic factor 2) Draw a vertical line for each prognostic factor, find the corresponding score on the Points line at the top of the Fig. 3) Add all corresponding scores to obtain the total score 4) The Total Points line at the bottom of the nomogram represents the relationship between total points and survival probability. Map the total score to this line, and obtain predicted survival probabilities for time points such as 1 year, 3 years, and 5 years
Fig. 3
Calibration curves for 1-year(A), 3-year(B), 5-year(C); Decision curves for 1-year(D), 3-year(E), 5-year(F)
Comments (0)