This study examined the correlation between AKI, as identified using electronic alerts based on a relative rise in serum creatinine levels, and clinical coding within the electronic hospital record for a national cohort of children. Overall, sensitivity of coding within the hospital record was poor (19.7%), increasing with peak AKI severity. Higher odds of being coded for AKI within the electronic record were seen with older age, while being in the birth cohort conferred lower likelihood of coding, particularly for preterm infants. Children living in less deprived quintiles (quintiles 1 and 3) had higher odds of coding compared to those living in the most deprived quintile. No correlation was noted between proportion of AKI alert-episodes coded and 30-day mortality on a hospital level.
With the potential to improve AKI recognition and care, many healthcare providers, including the National Health Service, have now implemented clinical indicator alerts as part of routine practice [10,11,12,13]. Most research seeking to validate these systems are based on adult cohorts, using administrative records as the reference standard; UK-based studies demonstrate that clinical coding in the hospital record has low sensitivity for AKI detected using the ‘Think Kidneys’ e-alert algorithm, which improves with higher peak AKI stage [7, 14]. Systematic review findings support these observations among adult populations, demonstrating higher sensitivity of coding among patients with evidence of more severe AKI, irrespective of definition used. Specificity for coded AKI is, however, consistently high, indicating that while the incidence of AKI using administrative codes may be underestimated, the risk of misclassification is low [15]. Less is known, however, about the usefulness of e-alerts in the clinical recognition of AKI in children. This study, which benefits from its large sample size and data capture on a national level, found that the sensitivity of electronic hospital record coding for AKI e-alerts in children was much lower at any peak AKI stage than previously reported among adult patients [7], suggesting that, in its current form, alerts from the NHS England algorithm do not equate to clinical recognition of AKI in children. Overall, administrative coding of AKI identified using relative changes in serum creatinine (19.7%) is lower than previously reported among other studies with multi-centre coverage [16, 17] but higher than that reported for critically ill children [18]. As seen by D’Arienzo and colleagues, higher rates of coding were noted for moderate- to severe-AKI episodes, suggesting that markedly abnormal creatinine values compared to baseline are more likely to be recognised and coded as AKI. This is supported by clinical audit findings that cases of clinically recognised AKI tend to have a higher median serum creatinine value than those that are not [17].
AKI is associated with later adverse outcomes such as hypertension, proteinuria, and chronic kidney disease, for which there are treatments that can help reduce disease progression. As children stand to gain important long-term benefits from early detection, understanding how e-alerts can be used to facilitate AKI recognition is urgently needed. Among adult patients, e-alerts are variably implemented and rarely incorporate instructions for clinical care [11], however systematic review findings suggest they could modify processes of care, particularly when intermediate steps are incorporated [11]. This potential has been demonstrated among paediatric cohorts: Goldstein and colleagues successfully demonstrated a 64% reduction in AKI incidence and 38% decrease in nephrotoxin exposure for ‘at-risk’ children when an e-alert prompted follow-up blood test monitoring, suggesting that e-alerts, in conjunction with active management, may improve AKI rates [19]. At hospital level, marked variation in the percentage of AKI episodes coded in the clinical record was noted, which may be due in part to how alerts are implemented clinically at individual hospitals and whether there are services or personnel available to support to AKI recognition and management. Understanding differences in clinical and coding practices for hospitals with high and low coding rates is required to drive quality improvements in clinical care, which will aid future disease surveillance.
Patient characteristics associated with lower likelihood of AKI coding in adults include younger age, female sex and South Asian or Black ethnicity [7]. Within the paediatric population, this study demonstrated a similar relationship between age and likelihood of coding; we hypothesise this graded association may be related to perceived risk of AKI by age, which may be confounded by factors such as co-existing disease and polypharmacy. The observation that among adults, elderly patients with multiple comorbidities are more likely to be coded for AKI in the medical record [20] raises the suggestion that clinicians are predisposed to consider AKI in traditionally ‘high risk’ patients, with multiple and/or complex medical conditions who may be on a number of medications; in contrast, as the majority of children attending hospital do not have complex or chronic conditions [21, 22], they may perceived to be at lower risk. An alternative hypothesis is that smaller children have inherently lower creatinine values and therefore the relatively small changes which flag an alert may be considered insignificant and/or overlooked. This is supported by this study’s finding that children experiencing AKI episodes during their birth admission were less likely to be coded for AKI, and by a US study which found patients with AKI were younger, smaller for age and had lower baseline creatinine values compared to those without [23]. As younger children, in particular neonates, are at high risk of adverse outcomes associated with AKI, including prolonged length of stay and mortality [5, 24], it is imperative factors mediating this association are understood and addressed.
Compared to the UK general population [25], children of non-White ethnicity were over-represented in our study sample, however this fails to consider the ethnic distribution of the exposed hospitalised cohort, the data for which were unavailable. This study also noted a higher burden of AKI among children living in more socioeconomically deprived areas, which has been described for children in Wales; in the US, higher AKI rates are reported among children without medical insurance [26, 27]. Socioeconomic deprivation is associated with higher age-adjusted mortality in adults, which is due to more severe AKI and a higher prevalence of pre-existing kidney disease [28, 29]. This study has found some evidence to suggest that children from more socioeconomically deprived areas were less likely to be coded for AKI compared to children living in areas of relative affluence. This observation raises the possibility of clinical bias in AKI recognition and/or coding, which warrants further investigation. Whether this association correlates with worse outcomes also requires review.
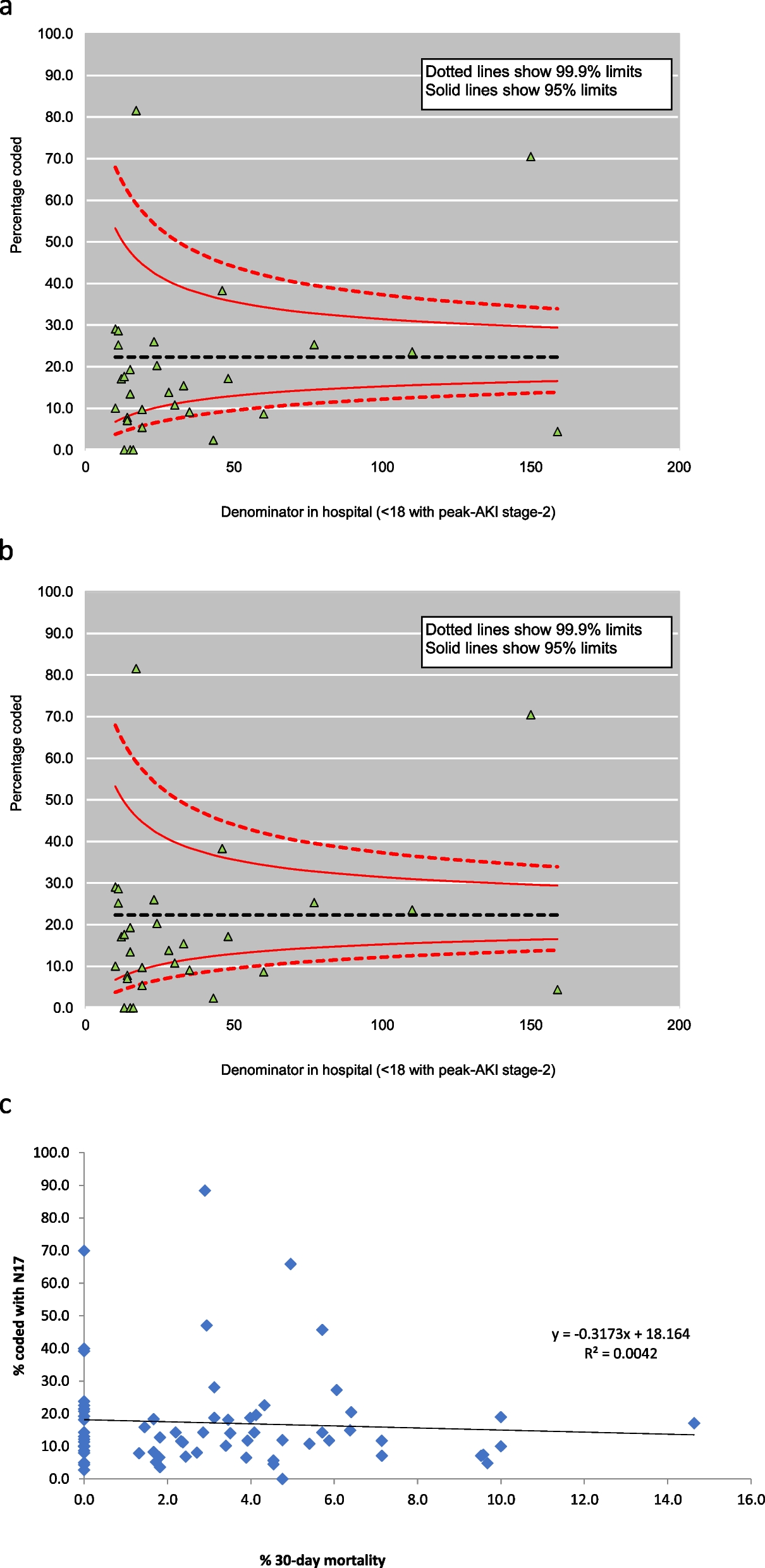
We failed to observe a correlation between clinical coding and 30-day mortality at a hospital level, which is in contrast to studies examining the association at patient-level [18]. As more severe cases of kidney disease, both acute and chronic, tend to be reported within the electronic health record [15, 30,31,32], the lack of association is encouraging. This result is a crude observation however and therefore must be interpreted cautiously. In a post hoc analysis, we noted children coded for AKI experienced generally higher lengths of stay in hospital than those who were not coded; as has been demonstrated in the adult CKD literature [32], this finding may suggest children who are more severely unwell (and thus have a longer length of stay) are captured more readily than those with milder disease.
This study examined the sensitivity of hospital records to reflect AKI episodes as identified using an electronic AKI alert algorithm which is standardised and implemented across NHS hospitals nationally, therefore it is anticipated these results will be generalisable to devolved UK nations. In their current form, electronic hospital records are likely to underestimate the incidence of AKI in children. This study has demonstrated the value of e-alerts in identifying where gaps occur in AKI coding, as a proxy for clinical recognition, and factors associated with coding in the clinical record. In the NHS, laboratory AKI alerts will not necessarily translate into the patient record without clinician recognition and documentation of AKI as a diagnosis. Further work is now needed to understand the reasons for these associations and to reduce potential inequalities in recognition which may have clinical implications, for management both acutely and in the long-term, given the growing evidence of the long-term consequences of AKI [33,34,35].
However, this study has limitations. Not all laboratories across England submitted data in time for linkage to HES; we estimate this report represents data from 66% of NHS laboratories across England [5]. Analyses were restricted to clinical codes for AKI using the N17.x code, which may have missed cases classified using procedural (kidney replacement therapy) or other diagnostic ICD-10 codes, for example N19 (unspecified kidney failure). Additionally, the presence of an AKI code (yes/no) was determined by a diagnostic code present at any time during an AKI-associated hospitalisation; given that corresponding diagnostic codes may be entered later in the electronic record, this may again underestimate the validity of the electronic record for detecting episodes derived from AKI alert data [15]. This study defined AKI using a national algorithm which uses relative changes in serum creatinine, which in children may inadvertently misclassify spurious values; this method may also miss cases of AKI using alternative measures, such as urine output [36]. There are now validated studies which impute baseline serum creatinine values which may support AKI identification in children who have not previously had a kidney function test performed [37, 38].
Finally, to what extent alerts truly reflect AKI, particularly stage one, requires further evaluation. While a standardised algorithm is used nationally, it is our understanding that locally, units may suppress alerts for certain populations (e.g., neonates, children known to kidney teams) therefore to what extent this influences clinical recognition (and therefore management) also requires review.
In conclusion, coding in hospital records shows poor agreement with AKI episodes defined using a rise in serum creatinine from baseline for children and young people, suggesting a lack of clinical recognition. Factors associated with lower levels of coding included lower stages of AKI, younger age, experiencing an AKI episode around the time of birth and living in a more deprived area. At hospital-level, the presence of AKI coding, as a proxy measure for recognition, did not correlate with 30-day mortality. Further work is now required to understand how e-alerts can be used to improve clinical recognition of AKI in children, to enhance care and outcomes.





Comments (0)