
Remember me

The intestinal barrier allows water uptake and nutrients while protecting against pathogens. Furthermore, the intestinal barrier must coexist harmoniously with gut microbiota, which plays a key role in host immunology and nutrient metabolism [19, 20]. On the other hand, parasites such as T. gondii can challenge the intestinal barrier and disrupt its homeostasis [21]. When C57BL/6 mice are orally infected by T. gondii, these mice develop a dysregulated inflammatory process that shares some immunopathological features with Crohn's disease [8]. This inflammatory response promotes lesions in the ileum, and it is primarily orchestrated by Th1 cells, Nitric Oxide (NO), and cytokines, including IL-12, IFN-γ, and TNF [22].
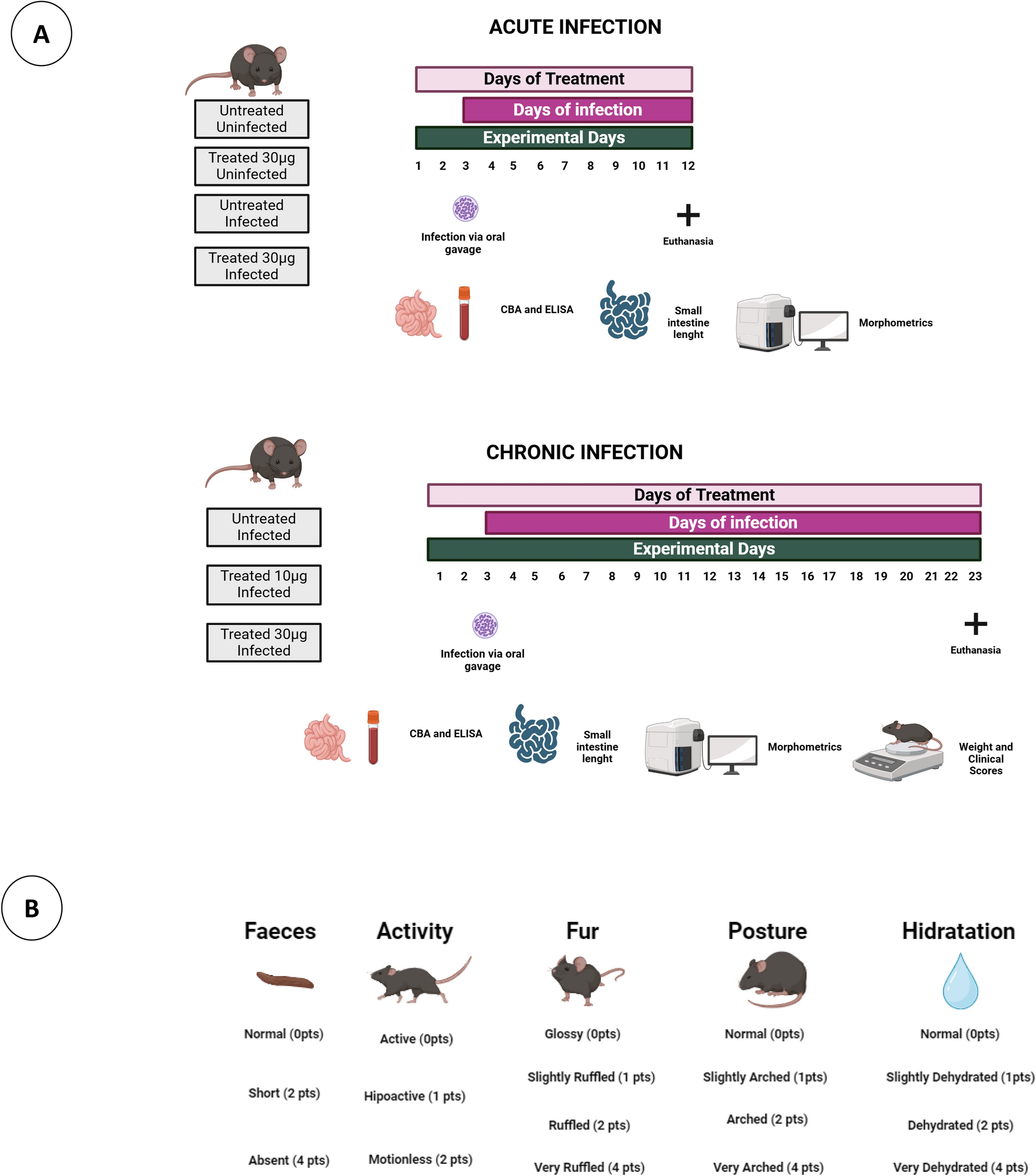
It is important to highlight that this study used C57BL/6 mice, a model known for its high susceptibility to T. gondii infection. The choice of this model is justified by its relevance in the investigation of the pathogenesis of toxoplasmosis, as the infection in these mice reproduces immunopathological characteristics observed in Crohn's disease in humans. The susceptibility of C57BL/6 mice to ileitis induced by Toxoplasma gondii is strongly associated with the activation of the CCR2 chemokine receptor and the immune response mediated by T cells. During infection, CCR2 is essential for the recruitment of CCR2 + CD4 + T cells to the intestinal lamina propria, where they interact with intraepithelial T cells (IELs), exacerbating inflammation. Additionally, the signaling of Th1 cytokines, such as TNF-α, plays a central role in pathogenesis, similar to what is observed in Crohn's disease. The elevated presence of CCR2 and its ligands, along with an increase in gram-negative bacteria in the gut, contributes to transmural damage and inflammation characteristic of ileitis. These immune and inflammatory interactions make C57BL/6 mice more susceptible to developing intestinal lesions when infected with T. gondii, with the presence of T cells and IELs further promoting the pro-inflammatory pathology [8, 23, 24]. In contrast, R. prolixus saliva contains various substances, like lipocalins, apyrases, and nitrophorins, which can induce a regulatory immune response [11]. Therefore, we aimed to explore the immunomodulatory effects of R. prolixus SGE during the dysregulated inflammatory processes induced by T. gondii in C57BL/6 mice. To assess the effectiveness of SGE in mitigating the deleterious effects of toxoplasmosis, we evaluated survival rates, clinical scores, weight loss, and small intestine length. Our data revealed that animals treated with 30 µg of SGE exhibited improved clinical parameters. In contrast, animals treated with 10 µg of SGE did not elicit a strong systemic protective response.
We hypothesized that 30 µg of SGE enhances the regulatory response during infection, thereby mitigating the harmful effects of an uncontrolled immune response. It is well-established that an intact intestinal barrier protects the host and prevents diseases [25]. In C57BL/6 mice, an impaired immune response can result in the destruction of the intestinal barrier, facilitating the translocation of bacteria and parasites, which leads to inflammation [6]. This inflammatory response can eventually progress to sepsis, worsening disease symptoms and potentially leading to death [7]. Furthermore, the small intestine plays a crucial role in digestion and nutrient absorption. Studies have shown that even mild inflammation can alter the gut's morphological structure, permeability, motility, and absorptive area, leading to impaired gastrointestinal function [26]. Based on this data, we suggest that the administration of R. prolixus SGE induced a regulatory immune response capable of mitigating the detrimental effects caused by T. gondii, leading to improvements in the clinical parameters observed in the treated animals.
To assess the immunomodulatory capacity of SGE, we analyzed the production of serum and intestinal cytokines. Our results revealed that, during the acute phase of T. gondii infection, there was an increase in both intestinal and systemic IFN-γ production, indicating the host's active defense against the parasite. Conversely, during the chronic phase of infection, we have observed a decrease in both serum and intestinal levels of this cytokine, which could be attributed to successful infection control. T. gondii infection triggers a powerful cell-mediated immune response in which IFN-γ plays a central role. Furthermore, this cytokine is essential for mediating T. gondii killing inside the parasitophorous vacuole [27].
Our data showed that, during the acute phase, treated animals exhibited significantly higher levels of systemic TNF compared to non-treated mice. TNF plays a pivotal role in immunopathology but is also crucial for combating the parasite. On the other hand, activation of the two TNF receptors (TNFRs) can mediate cell survival through the activation of the classical and alternative NFκB (Nuclear Factor kappa-light-chain-enhancer of activated B cells) pathways, as well as MAP kinase pathways [28, 29]. It is well-known that T. gondii infection initially triggers IL-12, which synergistically acts with TNF to stimulate the production of IFN-γ by NK cells. This coordinated immune response is essential for effective defense against T. gondii infection [30]. Furthermore, our data have demonstrated a significant increase in the levels of IL-12 in the small intestine of treated animals during the acute phase compared to non-infected mice infected with T. gondii.
MIF is an important cytokine that acts as a regulator of both innate and adaptive immune responses, playing a crucial role in the protection against T. gondii [31,32,33,34]. Our findings reveal elevated serum MIF levels during the chronic infection phase, indicative of a potential protective response aimed at controlling the parasite and facilitating tissue repair. This surge in MIF levels may be linked to its recognized capacity for angiogenesis and cellular proliferation [35]. Our data demonstrate that intestinal MIF increases in the acute infection phase and decreases in the chronic phase. The intestine serves as the primary inflammatory focus promoted by T. gondii and is crucial for controlling the infection. Furthermore, the reduction of MIF in the chronic infection phase may result in increased activity of regulatory cytokines, facilitating tissue repair and regeneration. Mice deficient in MIF and infected with T. gondii displayed heightened pathology and a significantly higher mortality rate than WT mice [36].
Furthermore, our data demonstrated that mice treated with SGE displayed an up-regulation of systemic IL-17 during the chronic phase, showing significantly higher levels compared to both the treated uninfected and treated acute phase groups. IL-17 is a proinflammatory cytokine that plays a crucial role in generating an optimal polymorphonuclear defense against T. gondii. IL-17 knockout mice exhibited increased mortality, which can be attributed to a defect in the migration of polymorphonuclear leukocytes to infected sites during the early stages of infection [37]. We suggest that IL-17 is involved in tissue repair and homeostasis. During the chronic infection phase, as the host attempts to control the infection and repair damaged tissues, the upregulation of IL-17 may be part of the immune system's efforts to restore normal tissue function [38].
Moreover, our results showed that T. gondii infection increased the production of serum and intestinal IL-6 both during the chronic and acute infection phases. Studies have suggested that in the absence of IL-6, mice are unable to initiate a rapid proinflammatory response against T. gondii, which allows for increased parasite growth. We propose that the presence of IL-6 is crucial for combating the parasite and effectively controlling the infection [39]. SGE-treated animals have presented significantly more intestinal IL-22 in the acute phase and more peripheral blood IL-22 in the chronic phase than to non-treated groups. IL-22 plays a pivotal role in the defense against pathogens due to its ability to promote wound healing, tissue repair, mucus production, and the production of antimicrobial proteins (AMPs) [40]. We have proposed that SGE could positively modulate the secretion of IL-22, thereby attenuating intestinal damage and facilitating tissue repair. Consequently, this modulation may lead to a more preserved intestinal environment. Additionally, IL-22 promotes the production of mucin, which acts as a protective barrier, preventing the direct invasion of bacteria into the intestinal epithelial cells [41].
A previous study has indicated that IL-23 plays a role in the development of intestinal immunopathology in response to T. gondii and in a model of inflammatory bowel disease [42]. Our findings revealed that during the acute phase, animals treated with SGE exhibited reduced intestinal IL-23 compared to the non-treated group, which may be associated with better morbidity score data in the treated group. On the other hand, in the chronic infection phase, the treated group showed a significant increase in intestinal IL-23 compared to the non-treated group. During the chronic phase, when the intestine is not the focus of infection, intestinal IL-23 may perform an alternative role. Recent studies have provided evidence that administering exogenous IL-23 can effectively restore IL-22 production and facilitate gut recovery. Furthermore, these studies have demonstrated the existence of a cytokine network involving IL-36γ, IL-23, and IL-22. This network plays a critical role in promoting antimicrobial activity, facilitating tissue repair, and supporting overall host survival [43].
During the chronic infection phase, SGE treatment has led to an increase in serum IL-10 and IL-4 levels. During infection, IL-10 exerts inhibitory effects on Th1 cells, NK cells, and macrophages, crucial for efficient pathogen clearance. However, excessive activation of these cells can also result in tissue damage. Therefore, IL-10 plays a dual role: it dampens the immune response to prevent excessive inflammation and tissue damage while maintaining a balance to support optimal pathogen clearance. IL-4 is another important cytokine due to its ability to control inflammation and down-regulate Th1 cytokines. Studies have shown that mice deficient in IL-4 or IL-10 exhibit higher mortality and increased pathology. Additionally, these studies have found significantly greater numbers of T. gondii cysts in the brains of IL-4 knockout mice than to wild-type [44]. SGE treatment increased intestinal IL-2 during the acute infection phase and serum IL-2 during the chronic phase. Studies have highlighted the critical role of IL-2 in maintaining Foxp3 + regulatory T cells (Treg cells). In the absence of IL-2, there is a significant depletion of Treg cells, leading to a severe deficiency that can contribute to the development of autoimmune disorders [45].
Our data demonstrated that intestinal IL-5 is predominantly produced during the acute infection phase compared to the chronic phase. Studies suggest that IL-5 may play a role in the production of IL-12. Additionally, IL-5 exerts pleiotropic activities on various target cells, including B cells, eosinophils, and basophils. It is produced by both hematopoietic and non-hematopoietic cells, including T cells, granulocytes, and natural helper cells [46]. Along these lines, we suggest that IL-5 plays an important role in the immune response against T. gondii during the acute phase. The present study showed that intestinal TGF-β is predominantly produced during acute infection, while serum TGF-β is more prominent during chronic infection. TGF-β is a potent immunosuppressive cytokine that plays a crucial role in developing and regulating various immune cells [47]. Nevertheless, it is known that TGF-β plays a dual role in T. gondii infection. In collaboration with IL-6 and IL-23, TGF-β promotes the production of IL-17 by NK cells and contributes to the development of Th17 lymphocytes during toxoplasmosis. This coordinated immune response is essential for parasite control [48].
In the acute phase of infection, administration of SGE has demonstrated a positive impact on the morphometric parameters of the ileum in treated animals. Treatment with SGE led to significant improvements in intestinal health. Specifically, in the acute phase, SGE reduced edema, crypt depth, and immunopathological changes while increasing the number of Paneth cells, essential for intestinal defense. In the chronic phase, SGE continued to promote recovery in the ileum, with reduced edema, increased villus size, and a higher number of Paneth cells than untreated animals. The protective effects also extended to the duodenum, where SGE treatment improved villus size, reduced crypt depth, and increased the number of goblet and Paneth cells, aiding in the recovery of intestinal architecture and function. In C57BL/6 mice, death typically occurs between 7 and 10 days after infection, accompanied by extensive necrosis of villi and mucosal cells in the ileum of the small intestine. This necrotic process leads to the destruction of the villi and the subsequent shortening of these structures [6, 22]. Necrosis depends on CD4 + T lymphocytes, IFN-γ, and nitric oxide, as demonstrated in previous studies [49, 50]. Additionally, the original study revealed that damage induction was mediated by αβTCR + cells but not by γδTCR + cells [6].
During inflammation, the connective tissue of the villi can undergo several alterations that impact its function. Increased blood vessel permeability leads to edema, while fibroblast hyperplasia and excessive collagen fiber production contribute to fibrosis and tissue thickening, impairing nutrient absorption. Additionally, the infiltration of immune cells and modifications in the extracellular matrix may further damage the tissue, compromising villus function. These changes can worsen inflammatory conditions and negatively affect intestinal health [51, 52]. Along these lines, we hypothesize that the immunoregulatory effects of SGE are responsible for mitigating the detrimental effects observed in infected animals. Infected and untreated animals during the acute phase exhibit increased deposition of connective tissue in the ileum, which correlates with a reduced intestinal epithelium. This is associated with heightened edema, inflammation, and ongoing attempts at tissue repair. The increased connective tissue indicates a robust inflammatory response, as well as the body's efforts to restore the damaged intestinal mucosa. Connective tissue plays a critical role in repairing the intestinal epithelium after injury. When the epithelium is damaged, the lamina propria, a connective tissue layer beneath the epithelium, is activated to initiate the healing process. Fibroblasts, which are responsible for producing the extracellular matrix, proliferate and generate new collagen fibers and other matrix components. This newly formed matrix provides structural support necessary for epithelial cell regeneration and the restoration of mucosal integrity [53, 54].
We observed an increase in the size and area of villi in the duodenum of treated animals during the chronic phase. Similarly, in the ileum, both treated and untreated groups showed an increase in villus size during the chronic phase. T. gondii infection may lead to a persistent enlargement of intestinal villi, both in the duodenum and ileum, during the chronic phase. This response could be attributed to chronic inflammation, tissue remodeling, changes in the microbiota, and immune mechanisms. These processes likely represent the organism's attempt to compensate for damage and maintain nutrient absorption [55]. In treated groups, the positive regulation of cytokines such as IL-22, IL-4, IL-10, and TGF-β during the chronic phase can significantly influence cell proliferation and the differentiation of stem cells in the intestinal crypts. These cytokines play pivotal roles in regulating the inflammatory environment and maintaining intestinal homeostasis, directly impacting the renewal and function of epithelial stem cells. For instance, IL-22 and TGF-β are recognized for their ability to modulate both intestinal regeneration and the inflammatory response, thereby affecting the dynamics of stem cells in the intestinal crypts [41, 56,57,58]
During the inflammatory and destructive processes affecting intestinal villi, the body initiates a repair mechanism to restore tissue integrity. Crypts, which are glandular structures located at the base of the villi, contain intestinal stem cells responsible for epithelial renewal. In response to inflammation, these stem cells are activated to proliferate and differentiate into new epithelial cells. These newly formed cells then migrate from the base to the tip of the villi to replace damaged cells. The increased proliferative activity leads to an enlargement of the crypts, reflecting the body's need for accelerated cell production to repair the injured tissue [59]. Inflammation can induce changes in intestinal tissue architecture, including the remodeling of crypts. This process often involves alterations in the size and shape of the crypts, leading to their expansion. The infiltration of immune cells during inflammation also plays a key role, as these cells release signaling molecules that stimulate the proliferation of crypt cells, further promoting their growth. Together, these mechanisms facilitate a rapid and effective response to repair tissue damage caused by inflammation, helping restore intestinal function [60, 61]. In this context, untreated animals typically exhibit larger crypts, reflecting more significant damage to the intestinal barrier and a more intense inflammatory response. As a result, there is an increased in stem cells proliferation to compensate for the extensive tissue damage.
Our results demonstrated that both in the ileum and the duodenum, animals treated with SGE showed an increase in the number of goblet cells. In the context of T. gondii infection, goblet cells play a crucial role in the host's defense. The mucus secreted by these cells acts as a physical barrier, preventing the adhesion and penetration of the parasite into the intestinal mucosa. Additionally, mucus contains antimicrobial molecules, such as immunoglobulins, antimicrobial peptides, and enzymes, which contributes to the control of T. gondii proliferation. Studies also suggest that goblet cells participate in the immune response against the parasite by modulating the activity of immune cells and secreting pro-inflammatory cytokines. In this context, a higher number of goblet cells may be associated with reduced parasitism during the chronic phase of infection [62, 63].
Our results highlighted a significant reduction in the number of goblet cells in animals during the chronic phase. Oral infection with T. gondii can lead to a marked decrease in goblet cell numbers due to a combination of factors. The inflammatory response triggered by the infection, similar to what occurs in chronic inflammations such as inflammatory bowel diseases, can directly damage these cells or disrupt the intestinal microenvironment, impairing their survival and differentiation. Furthermore, the parasite may alter the intestinal microbiota, affect cellular signaling pathways involved in goblet cell differentiation, and modulate the immune response in the mucosa, indirectly impacting goblet cell population dynamics [21]. In the context of SGE treatment, the observed increase in the number of goblet cells, particularly in the duodenum during the chronic phase, underscores its positive impact on intestinal protection and regeneration. This finding suggests that SGE plays a crucial role in maintaining the integrity of the intestinal mucosa by promoting the proliferation of goblet cells and enhancing mucus production, which is essential for defense against pathogens. Furthermore, the increase in goblet cells may indicate an effective repair process and a strengthening of the mucosal barrier function [21, 62].
The SGE from various species of triatomines exhibits immunomodulatory potential, influencing the immune response in distinct ways. In vitro studies demonstrated that the SGE from P. lignarius, M. pallidipennis, T. lecticularia, and R. prolixus inhibited dendritic cell (DC) differentiation and modulated the expression of costimulatory molecules on mature DCs. Additionally, the SGE suppressed the production of pro-inflammatory cytokines while promoting the production of IL-10 in LPS-stimulated DCs. In vivo studies further support the immunomodulatory capacity of SGE in mitigating inflammatory damage. In the DSS-induced colitis model, the SGE from T. lecticularia alleviated the severity of intestinal inflammation by reducing levels of the inflammatory cytokine IL-6 and increasing the regulatory cytokine IL-10 in the intestine [9]. It is important to note that the composition of SGE varies across triatomine species, and this variation may account for the differences in the observed effects.
The susceptibility of the C57BL/6 mouse model to Toxoplasma gondii infection likely influenced the magnitude of the protective effects observed with SGE treatment at 30 µg. The intense intestinal inflammation characteristic of this strain may have amplified the therapeutic benefits of SGE, underscoring its potential as a modulator of exaggerated inflammatory responses. While the widespread use of the C57BL/6 model in T. gondii research facilitates comparative studies, it also limits the generalizability of findings to other strains or to humans. Nonetheless, this model was instrumental in elucidating the immunopathological mechanisms of toxoplasmosis and the effects of SGE in the context of severe inflammation. SGE demonstrated significant protective effects, including reduced weight loss during the chronic phase, preservation of intestinal integrity, and a balanced immune response (Fig. 13). These findings align with the broader immunomodulatory properties of salivary gland extracts SGE from various triatomine species, which influence immune responses and hold therapeutic potential for infectious and inflammatory diseases.
Fig. 13
Schematic model representing T. gondii infection in C57BL/6 mice and the influence of SGE treatment on cytokine release in serum and the small intestine. Our data demonstrate that T. gondii infection increases the levels of inflammatory cytokines such as TNF and IFN-γ in both mouse serum and small intestine tissue. Additionally, animals treated with the highest concentration of SGE experienced less weight loss and lower clinical scores. Specifically, mice treated with SGE 30 µg exhibited a significant increase in systemic regulatory cytokines, including IL-4, IL-2, and IL-10, during the chronic phase of infection. Cytokine analysis further revealed that SGE-treated mice secreted more intestinal IL-4 in the chronic phase and increased levels of IL-2 and IL-22 in the acute phase. Moreover, cyst counts indicated that SGE-treated groups had significantly fewer cysts in brain tissue compared to the untreated group. Therefore, our findings demonstrate that SGE has the ability to induce a regulatory response, mitigating the detrimental effects of uncontrolled inflammation and providing protection against T. gondii infection
Future research should explore the mechanisms of SGE more comprehensively, examining its impact on immune cell populations, signaling pathways, intestinal microbiota, and gene expression to identify potential therapeutic targets. Moreover, we acknowledge the importance of this analysis for a more comprehensive understanding of the infection, and thus, we plan to include parasite load quantification in our future studies to better correlate the immune effects with parasite burden.
Declaration of generative AI and AI-assisted technologies in the writing processDuring the preparation of this work the author(s) used ChatGPT 3.5/OpenAI in order to improve readability and language. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Comments (0)