Main findings
This study uncovered several important findings regarding the relationships between ABE with 30-day and 90-day ICU all-cause mortality outcomes in sepsis patients. First, we observed significant differences across ABE quartiles in baseline characteristics, indicating the clinical heterogeneity of patients based on ABE levels. Second, ABE was associated with a U-shaped association with the risk of 30-day and 90-day all-cause mortality in the ICU among patients with sepsis, in which both the lowest (Q1) and highest (Q4) quartiles of ABE were associated with increased 30-day and 90-day ICU and hospital all-cause mortality. This indicates that a deviation from the normal value of ABE may indicate an adverse prognosis. Third, our threshold analysis identified inflection points of ABE (2.5 mmol/L for 30-day ICU all-cause mortality and 2.2 mmol/L for 90-day ICU all-cause mortality), indicating a change in the mortality risk relationship, which is negatively correlated below these thresholds and positively correlated above them. Fourth, subgroup analysis revealed a significant interaction between age and obesity with ABE quartiles. Finally, combining ABE with the SOFA score significantly improved the predictive performance for 30-day and 90-day ICU all-cause mortality.
Mechanistic insights of ABE in sepsis prognosis
The correlation between ABE and mortality in sepsis may be explained by several mechanisms: first, sepsis is often accompanied by systemic inflammatory response syndrome, which can directly stimulate the glycolytic pathway through inflammatory mediators (such as tumor necrosis factor-α and interleukin-6), increasing lactate production. High levels of lactate indicate significant tissue hypoxia, which usually suggests severe illness and increased risk of mortality [20]. In addition, liver dysfunction in sepsis patients leads to reduced lactate clearance [9]. Second, lactate accumulation is a significant cause of metabolic acidosis, which itself has detrimental effects on multiple organ systems, including myocardial depression, reduced vascular responsiveness, immune suppression, and altered enzyme activity. These factors collectively exacerbate organ dysfunction and increase mortality in sepsis patients [20,21,22]. Furthermore, the interaction between inflammation and metabolic disturbances leads to elevated lactate levels and changes in acid–base excess, creating a vicious cycle that results in persistently negative ABE values, a condition often associated with higher mortality [5] In addition, sepsis patients often receive saline for fluid management, and hyperchloremic acidosis, which is common in clinical practice, can further increase negative ABE values [22]. In addition, high ABE values may indicate metabolic alkalosis due to hyperventilation, bicarbonate therapy, volume depletion, or electrolyte imbalance, all of which impair oxygen delivery and cardiovascular stability, leading to increased mortality. Moreover, hepatic dysfunction associated with sepsis may reduce ammonia clearance, further contributing to systemic alkalosis. Together, these mechanisms explain why both low and high ABE values are associated with increased mortality, showing a U-shaped association.
ABE is also linked to sepsis-related complications through various mechanisms. The kidneys are crucial in maintaining acid–base balance, and sepsis-related acute kidney injury can result in the buildup of acidic substances and a loss of buffering capacity [21], manifesting as negative ABE. Poor tissue perfusion and systemic inflammatory responses can exacerbate sepsis, leading to septic shock and further tissue hypoxia, creating a vicious cycle [23]. In patients presenting with acute respiratory distress syndrome, both respiratory and metabolic acidosis may be present due to disruption of the alveolar–capillary barrier, impaired oxygen exchange, and limited carbon dioxide excretion. This combined acidosis significantly decreases ABE, indicating severe metabolic derangement and a poor prognosis [24].
Comparison with previous study
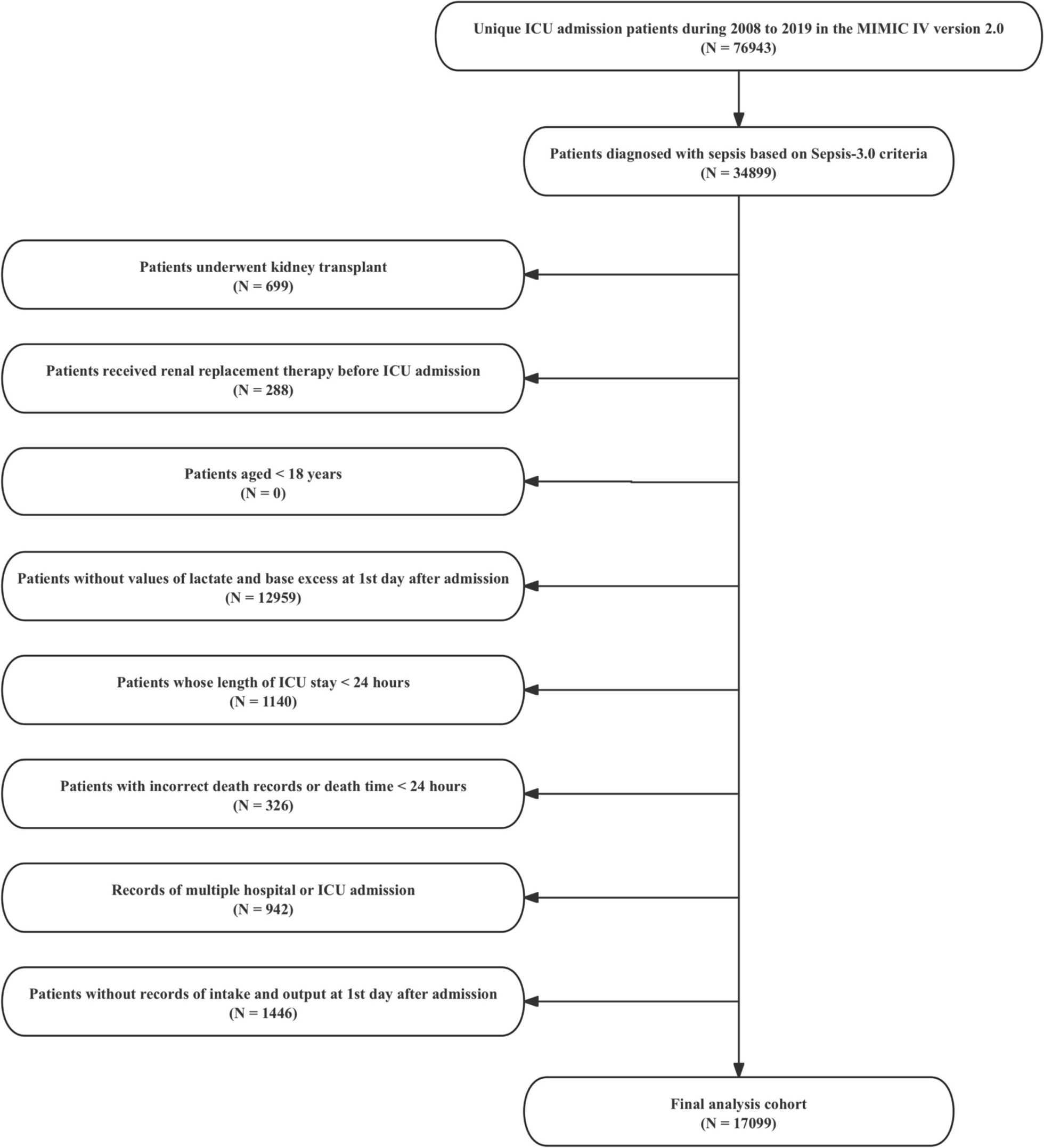
To date, only one study has been conducted on the relationship between ABE and death in patients with sepsis (N = 1178). Cantos et al. also reported a U-shaped relationship between ABE and hospital mortality in sepsis patients, after Inverse Probability of Treatment Weighting, compared with neutral ABE (≥ − 3 and < 4 mmol/L), negative ABE (< − 3 mmol/L) was associated with a higher risk of hospital mortality (HR = 1.56; 95% CI 1.11–2.18), while there was no significant difference in the risk of hospital mortality among patients with positive ABE (≥ 4 mmol/L) [13]. However, this study provides a more nuanced understanding of the critical effect of ABE in a cohort of more than 17,000 ICU sepsis cohort. Specifically, our threshold analysis found inflection points of 2.5 mmol/L for 30-day mortality and 2.2 mmol/L for 90-day mortality, suggesting that there are different optimal cutoffs for risk stratification. Unlike the classifications (negative, neutral, positive ABE) used in previous studies, our approach highlights a U-shaped relationship, where both significantly low and high ABE values are associated with increased mortality. This distinction suggests that a more refined threshold can better capture the complex interactions of metabolic disorders. These findings hold important implications for clinical practice. Identifying distinct inflection points for 30-day and 90-day mortality allows for more tailored risk stratification in critically ill sepsis patients. The discovery of a U-shaped relationship between ABE and mortality further underscores the complexity of metabolic disturbances, suggesting that both extremes of ABE warrant close monitoring. This nuanced understanding may facilitate the development of individualized therapeutic strategies aimed at correcting severe acid–base imbalances.
Clinical implications and future research directions
Based on our findings, the combination of ABE and the traditional score for ICU mortality, the SOFA score, [25] plays a key role in improving the accuracy of mortality prediction in sepsis patients. This combined method provides a more reliable assessment of sepsis prognosis, highlighting the added value of ABE in improving the performance of the traditional SOFA model. A significantly negative ABE accurately reflects metabolic disturbances and helps in the early identification of sepsis patients at high risk due to metabolic imbalances. Changes in ABE, whether improvement or deterioration—can directly reflect shifts in the patient’s metabolic status, indicating whether the treatment is effective or the condition is worsening. ABE is derived from routine blood gas analysis data and can be obtained through simple calculations, making it widely applicable to various types of sepsis patients. However, ABE’s sensitivity to fluctuations in lactate levels—affected by liver function, systemic inflammation, and clinical interventions (e.g., fluid resuscitation and vasopressor agents), [26, 27] which may introduce variability in its predictive accuracy, particularly in specific clinical contexts.
Specifically, the observed association between high ABE levels and worse outcomes highlights the complex physiological implications of its components, particularly BE and lactate. Our analysis demonstrated that elevated ABE values were primarily driven by markedly positive BE, while lactate remained elevated but did not appear to be the primary driver, indicating a predominantly metabolic alkalosis with a potential contribution from lactic acidosis. A large BE typically reflects metabolic alkalosis, which may arise from conditions, such as hypochloremia, hypokalemia, prolonged vomiting, or excessive bicarbonate therapy [28]. These disturbances can impair oxygen delivery at the tissue level through a leftward shift in the oxygen–hemoglobin dissociation curve, exacerbate systemic hypoperfusion, and worsen hemodynamic instability [29]. Concurrently, elevated lactate serves as a marker of ongoing tissue hypoxia and cellular stress, reflecting a state of metabolic derangement rather than recovery [30]. The coexistence of these abnormalities likely represents a maladaptive response to systemic stress, contributing to microvascular dysfunction, impaired organ perfusion, and multi-organ failure, which could explain the increased mortality associated with high ABE levels. These findings underscore the importance of interpreting high ABE values in conjunction with its individual components and the broader clinical context, rather than as an isolated biomarker. Further research is warranted to elucidate these mechanisms and to determine whether metabolic disturbances identified by ABE could become targets for intervention or remain primarily useful for clinical monitoring.
ABE enhances acid–base assessment by integrating both lactate-dependent and lactate-independent disturbances, making it valuable in ICU settings. It helps differentiate metabolic acidosis causes, distinguishing lactate-driven hypoxia from non-lactate imbalances, such as renal dysfunction or hyperchloremic acidosis, guiding tailored resuscitation. ABE is also more stable in patients receiving fluid resuscitation or mechanical ventilation, where BE may be confounded by hyperchloremic acidosis or respiratory alkalosis. Clinically, ABE is easily implemented as it is derived from lactate and BE of standard arterial blood gas analysis, requiring no additional testing, making it a practical and cost-effective tool for risk stratification in sepsis patients.
According to the current evidence, a significantly negative ABE value is consistently related to increased mortality, positioning ABE as an important biomarker for adverse prognosis of sepsis patients. The simplicity and reliability of ABE in assessing the patient’s metabolic status make it an essential component in developing robust multivariate prediction models. In addition, machine learning models trained on comprehensive data sets including ABE can identify complex nonlinear interactions and provide a more nuanced understanding of patient’s prognosis [31]. Integrating ABE into machine learning algorithms may bring significant benefits and improve the accuracy of sepsis risk stratification. This approach has the potential to improve predictive capabilities, promote early intervention, support dynamic patient monitoring, and ultimately improve the prognosis of sepsis patients.
Further studies are needed to explore ABE’s utility in different sepsis subgroups, such as pneumonia-related sepsis, abdominal infections, and sepsis in immunocompromised patients. Moreover, combining ABE with other biomarkers, such as C-reactive protein, interleukin-6, D-dimer, and fibrinogen could further improve the predictive performance. Large-scale prospective studies are required to refine the sepsis prognosis model and support its use in developing personalized treatment strategies for high-risk sepsis population in ICU setting. In addition, our results demonstrated that combining ABE with the SOFA score resulted in a statistically significant improvement in predictive performance, as measured by the AUC. However, it is important to acknowledge that this improvement, while statistically significant, may have limited clinical relevance in its current form. The modest increase in AUC highlights the need to explore further combinations of ABE with other clinical variables beyond the SOFA score. Such efforts could potentially yield novel evaluation tools with greater predictive accuracy and clinical utility. Moreover, the findings underscore the potential role of ABE as a complementary biomarker in sepsis prognosis, which warrants further investigation in larger, prospective studies. Future research should also focus on determining whether these enhancements in predictive performance translate into improved clinical decision-making and sepsis patient outcomes.
Limitations
However, there are several limitations in this study. First, this study is a single-center retrospective analysis, which may restrict the generalizability of our findings, especially when applied to broader populations outside of ICU setting. Second, certain confounding variables that could influence outcomes, such as chronic comorbidities and medication histories, were not fully accounted for in our analysis. This may have introduced residual confounding and limited the accuracy of our findings. Third, we primarily analyzed baseline ABE values on first day after ICU admission, without considering dynamic changes in ABE levels over time, which could provide additional prognostic insights. Fourth, the use of electronic health records may have led to misclassification or incomplete recording of clinical data, thus potentially affecting the reliability of our findings. Fifth, as ABE may be dynamic and multiple consecutive ABE measurements may provide additional prognostic insights, future studies incorporating dynamic trends in ABE are warranted. Sixth, although the predictive properties of ABE were statistically significant when used in combination with the SOFA score, the absolute increase in AUC was modest, and overall AUC values remained relatively low. Future studies should explore the potential value of continuous ABE measurements and their integration with other biomarkers to enhance risk stratification in patients with severe sepsis. Finally, the ABE is highly sensitive to lactate levels, which may be affected by factors unrelated to sepsis, complicating its interpretation in different clinical scenarios. Future prospective studies should aim to validate our findings through multi-centre prospective studies.






Comments (0)